-
 Receiver operating characteristic curve: overview and practical use for clinicians
Receiver operating characteristic curve: overview and practical use for clinicians
- Francis Sahngun Nahm
-
Korean J Anesthesiol. 2022;75(1):25-36.
-
Statistical Round
January 18, 2022
|
-
 Remimazolam – current knowledge on a new intravenous benzodiazepine anesthetic agent
Remimazolam – current knowledge on a new intravenous benzodiazepine anesthetic agent
- Seong-Hyop Kim, Jörg Fechner
-
Korean J Anesthesiol. 2022;75(4):307-315.
-
Review Article
May 19, 2022
|
-
 Anatomical classification and clinical application of thoracic paraspinal blocks
Anatomical classification and clinical application of thoracic paraspinal blocks
- Shin Hyung Kim
-
Korean J Anesthesiol. 2022;75(4):295-306.
-
Review Article
April 4, 2022
|
-
Mechanisms underlying lipid emulsion resuscitation for drug toxicity: a narrative review
- Soo Hee Lee, Ju-Tae Sohn
-
Korean J Anesthesiol. 2023;76(3):171-182.
-
Review Article
January 26, 2023
|
-
 Cadaveric investigation of the spread of the thoracoabdominal nerve block using the perichondral and modified perichondral approaches
Cadaveric investigation of the spread of the thoracoabdominal nerve block using the perichondral and modified perichondral approaches
- Bahadir Ciftci, Haci Ahmet Alici, Gamze Ansen, Bayram Ufuk Sakul, Serkan Tulgar
-
Korean J Anesthesiol. 2022;75(4):357-359.
-
Letter to the Editor
April 26, 2022
|
-
 Regional analgesia techniques for video-assisted thoracic surgery: a frequentist network meta-analysis
Regional analgesia techniques for video-assisted thoracic surgery: a frequentist network meta-analysis
- Yumin Jo, Seyeon Park, Chahyun Oh, Yujin Pak, Kuhee Jeong, Sangwon Yun, Chan Noh, Woosuk Chung, Yoon-Hee Kim, Young Kwon Ko, et al.
-
Korean J Anesthesiol. 2022;75(3):231-244.
-
Clinical Research Article
October 13, 2021
|
-
 The effect of ultrasound-guided bilateral thoracic retrolaminar block on analgesia after pediatric open cardiac surgery: a randomized controlled double-blind study
The effect of ultrasound-guided bilateral thoracic retrolaminar block on analgesia after pediatric open cardiac surgery: a randomized controlled double-blind study
- Ibrahim Abdelbaser, Nabil A. Mageed, Sherif I. Elfayoumy, Mohamed Magdy, Mohamed M. Elmorsy, Mahmoud M. ALseoudy
-
Korean J Anesthesiol. 2022;75(3):276-282.
-
Clinical Research Article
January 12, 2022
|
-
 Different perspectives for monitoring nociception during general anesthesia
Different perspectives for monitoring nociception during general anesthesia
- Pablo Martinez-Vazquez, Erik Weber Jensen
-
Korean J Anesthesiol. 2022;75(2):112-123.
-
Review Article
February 17, 2022
|
-
 Comparison of postoperative nausea and vomiting between remimazolam and propofol: a propensity score-matched, retrospective, observational, single-center cohort study
Comparison of postoperative nausea and vomiting between remimazolam and propofol: a propensity score-matched, retrospective, observational, single-center cohort study
- Yuji Suzuki, Shingo Kawashima, Hiroshi Makino, Matsuyuki Doi, Yoshiki Nakajima
-
Korean J Anesthesiol. 2023;76(2):143-151.
-
Clinical Research Article
October 17, 2022
|
-
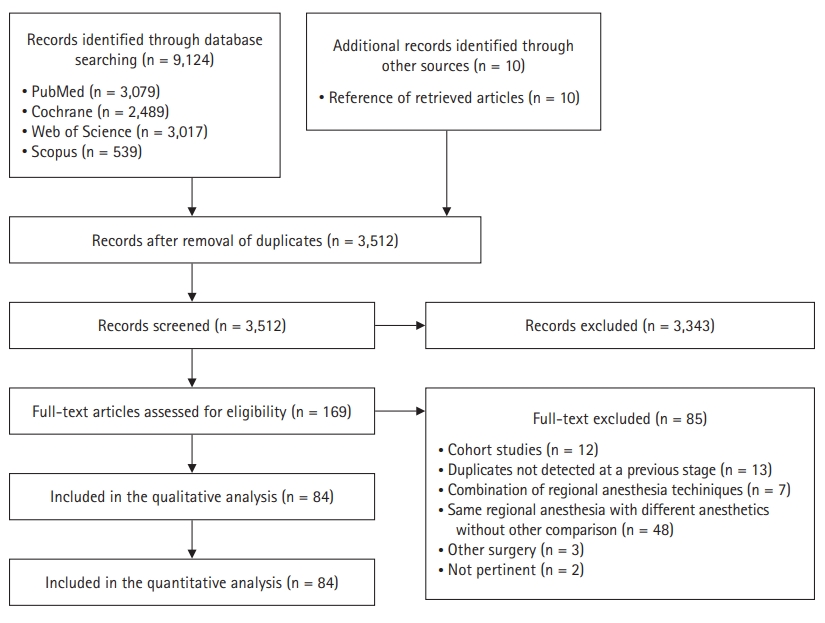 Single-shot regional anesthesia for laparoscopic cholecystectomies: a systematic review and network meta-analysis[commentary-article]
Single-shot regional anesthesia for laparoscopic cholecystectomies: a systematic review and network meta-analysis[commentary-article]
- Alessandro De Cassai, Nicolò Sella, Federico Geraldini, Serkan Tulgar, Ali Ahiskalioglu, Burhan Dost, Silvia Manfrin, Yunus Emre Karapinar, Greta Paganini, Muzeyyen Beldagli, et al.
-
Korean J Anesthesiol. 2023;76(1):34-46.
-
Clinical Research Article
November 8, 2022
|
-
 Role of carotid corrected flow time and peak velocity variation in predicting fluid responsiveness: a systematic review and meta-analysis
Role of carotid corrected flow time and peak velocity variation in predicting fluid responsiveness: a systematic review and meta-analysis
- Deepak Singla, Bhavna Gupta, Pragya Varshney, Mishu Mangla, Beeraling Ningappa Walikar, Tiajem Jamir
-
Korean J Anesthesiol. 2023;76(3):183-193.
-
Clinical Research Article
November 15, 2022
|
-
 Artificial intelligence in perioperative medicine: a narrative review
Artificial intelligence in perioperative medicine: a narrative review
- Hyun-Kyu Yoon, Hyun-Lim Yang, Chul-Woo Jung, Hyung-Chul Lee
-
Korean J Anesthesiol. 2022;75(3):202-215.
-
Review Article
March 29, 2022
|
-
 Comparison of the pericapsular nerve group block with the intra-articular and quadratus lumborum blocks in primary total hip arthroplasty: a randomized controlled trial[commentary-article]
Comparison of the pericapsular nerve group block with the intra-articular and quadratus lumborum blocks in primary total hip arthroplasty: a randomized controlled trial[commentary-article]
- Tayfun Et, Muhammet Korkusuz
-
Korean J Anesthesiol. 2023;76(6):575-585.
-
Clinical Research Article
April 4, 2023
|
-
 Erector spinae plane block in children: a narrative review
Erector spinae plane block in children: a narrative review
- Monica Lucente, Giulia Ragonesi, Marco Sanguigni, Fabio Sbaraglia, Alessandro Vergari, Rosa Lamacchia, Demetrio Del Prete, Marco Rossi
-
Korean J Anesthesiol. 2022;75(6):473-486.
-
Review Article
July 5, 2022
|
-
 Determination of the 95% effective dose of remimazolam to achieve loss of consciousness during anesthesia induction in different age groups
Determination of the 95% effective dose of remimazolam to achieve loss of consciousness during anesthesia induction in different age groups
- Juyeon Oh, Sung Yong Park, Sook Young Lee, Ju Yeol Song, Ga Yun Lee, Ji Hyun Park, Han Bum Joe
-
Korean J Anesthesiol. 2022;75(6):510-517.
-
Clinical Research Article
August 1, 2022
|
-
 Effects of dexamethasone on catheter-related bladder discomfort and emergence agitation: a prospective, randomized, controlled trial
Effects of dexamethasone on catheter-related bladder discomfort and emergence agitation: a prospective, randomized, controlled trial
- Sung-Ae Cho, Inho Huh, Seok-Jin Lee, Tae-Yun Sung, Gwan Woo Ku, Choon-Kyu Cho, Young Seok Jee
-
Korean J Anesthesiol. 2022;75(1):71-78.
-
Clinical Research Article
September 17, 2021
|
-
 The impact of preoperative glycated hemoglobin (HbA1c) on postoperative complications after elective major abdominal surgery: a meta-analysis
The impact of preoperative glycated hemoglobin (HbA1c) on postoperative complications after elective major abdominal surgery: a meta-analysis
- Joanna K. L. Wong, Yuhe Ke, Yi Jing Ong, HuiHua Li, Ting Hway Wong, Hairil Rizal Abdullah
-
Korean J Anesthesiol. 2022;75(1):47-60.
-
Clinical Research Article
October 8, 2021
|
-
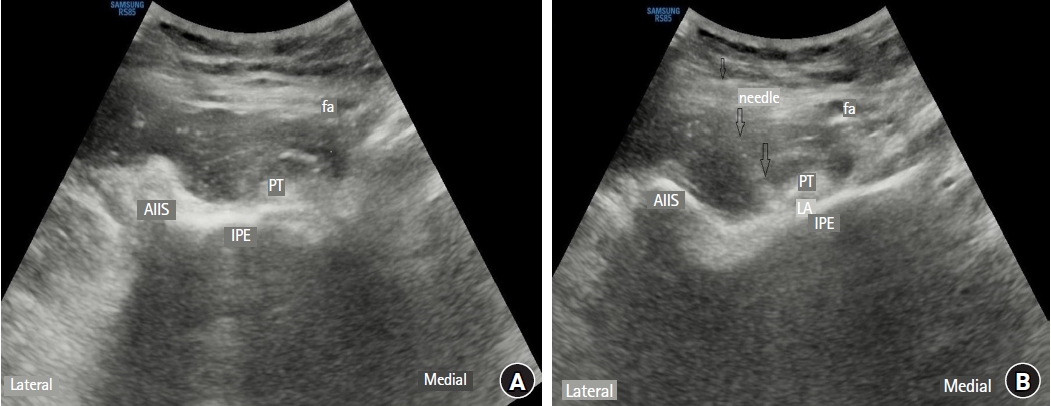
 Efficacy of ultrasound-guided transversalis fascia plane block in pediatric ureteroneocystostomy surgery
Efficacy of ultrasound-guided transversalis fascia plane block in pediatric ureteroneocystostomy surgery
- Uğur Peksöz, Ahmet Murat Yayık, Erkan Cem Çelik
-
Korean J Anesthesiol. 2022;75(2):188-190.
-
Letter to the Editor
November 4, 2021
|
-
 Standard digit-based versus 90° rotation technique for supraglottic airway device insertion: a meta-analysis of randomized controlled trials
Standard digit-based versus 90° rotation technique for supraglottic airway device insertion: a meta-analysis of randomized controlled trials
- Chang-Hoon Koo, Ah-Young Oh, Young-Tae Jeon, Jung-Won Hwang, Jung-Hee Ryu
-
Korean J Anesthesiol. 2022;75(3):266-275.
-
Clinical Research Article
December 9, 2021
|
-
 Efficacy of perineural versus intravenous dexamethasone in prolonging the duration of analgesia when administered with peripheral nerve blocks: a systematic review and meta-analysis
Efficacy of perineural versus intravenous dexamethasone in prolonging the duration of analgesia when administered with peripheral nerve blocks: a systematic review and meta-analysis
- Elizabeth Sein Jieh Tan, Yan Ru Tan, Christopher Wei Yang Liu
-
Korean J Anesthesiol. 2022;75(3):255-265.
-
Clinical Research Article
December 29, 2021
|
-
 Therapeutic hypothermia for acute myocardial infarction: a narrative review of evidence from animal and clinical studies
Therapeutic hypothermia for acute myocardial infarction: a narrative review of evidence from animal and clinical studies
- Ki Tae Jung, Aneesh Bapat, Young-Kug Kim, William J. Hucker, Kichang Lee
-
Korean J Anesthesiol. 2022;75(3):216-230.
-
Review Article
March 30, 2022
|
-
 Feasibility and efficacy of erector spinae plane block versus transversus abdominis plane block in laparoscopic bariatric surgery: a randomized comparative trial [commentary-article]
Feasibility and efficacy of erector spinae plane block versus transversus abdominis plane block in laparoscopic bariatric surgery: a randomized comparative trial [commentary-article]
- Mohamed Elshazly, Yasser Mohamed EL-Halafawy, Dina Zakaria Mohamed, Khaled Abd El Wahab, Tamer Mohamed Kheir Mohamed
-
Korean J Anesthesiol. 2022;75(6):502-509.
-
Clinical Research Article
May 18, 2022
|
-
 Preemptive visceral analgesic effect of thoracic paravertebral block on postoperative opioid consumption in patients undergoing laparoscopic cholecystectomy: a prospective, randomized, assessor-blind study
Preemptive visceral analgesic effect of thoracic paravertebral block on postoperative opioid consumption in patients undergoing laparoscopic cholecystectomy: a prospective, randomized, assessor-blind study
- Jong-Hyuk Lee, Chan-Sik Kim, Hyungtae Kim, Jae Moon Choi, Youngmu Kim, Sung-Moon Jeong, Seong-Soo Choi
-
Korean J Anesthesiol. 2023;76(3):203-212.
-
Clinical Research Article
December 21, 2022
|
-
 Erector spinae plane versus fascia iliaca block after total hip arthroplasty: a randomized clinical trial comparing analgesic effectiveness and motor block
Erector spinae plane versus fascia iliaca block after total hip arthroplasty: a randomized clinical trial comparing analgesic effectiveness and motor block
- Edoardo Flaviano, Silvia Bettinelli, Maddalena Assandri, Hassam Muhammad, Alberto Benigni, Gianluca Cappelleri, Edward Rivera Mariano, Luca Ferdinando Lorini, Dario Bugada
-
Korean J Anesthesiol. 2023;76(4):326-335.
-
Clinical Research Article
January 12, 2023
|
-
 Comparison of upper and lower body forced air blanket to prevent perioperative hypothermia in patients who underwent spinal surgery in prone position: a randomized controlled trial
Comparison of upper and lower body forced air blanket to prevent perioperative hypothermia in patients who underwent spinal surgery in prone position: a randomized controlled trial
- Jae Hwa Yoo, Si Young Ok, Sang Ho Kim, Ji Won Chung, Sun Young Park, Mun Gyu Kim, Ho Bum Cho, Sang Hoon Song, Yun Jeong Choi, Hyun Ju Kim, et al.
-
Korean J Anesthesiol. 2022;75(1):37-46.
-
Clinical Research Article
May 13, 2021
|
-
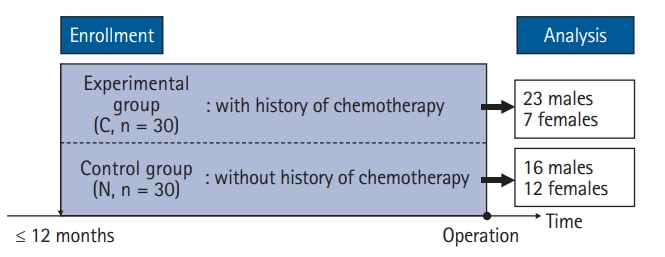 Effect of chemotherapy on effect-site concentration of propofol for loss of consciousness in patients with colorectal cancer
Effect of chemotherapy on effect-site concentration of propofol for loss of consciousness in patients with colorectal cancer
- Seunghee Ki, Yongwon Cho, Youngkyung Choi, Sehun Lim, Myounghun Kim, Jeonghan Lee
-
Korean J Anesthesiol. 2022;75(2):160-167.
-
Clinical Research Article
September 17, 2021
|
-
 Preoperative dexmedetomidine and intraoperative bradycardia in laparoscopic cholecystectomy: a meta-analysis with trial sequential analysis
Preoperative dexmedetomidine and intraoperative bradycardia in laparoscopic cholecystectomy: a meta-analysis with trial sequential analysis
- Alessandro De Cassai, Nicolò Sella, Federico Geraldini, Francesco Zarantonello, Tommaso Pettenuzzo, Laura Pasin, Margherita Iuzzolino, Nicolò Rossini, Elisa Pesenti, Giovanni Zecchino, et al.
-
Korean J Anesthesiol. 2022;75(3):245-254.
-
Clinical Research Article
January 12, 2022
|
-
 Ultrasound-guided lumbar erector spinae plane block versus caudal block for postoperative analgesia in pediatric hip and proximal femur surgery: a randomized controlled study
Ultrasound-guided lumbar erector spinae plane block versus caudal block for postoperative analgesia in pediatric hip and proximal femur surgery: a randomized controlled study
- Mohamed Elshazly, AbdelKhalek Shaban, Nevine Gouda, Mahitab Rashad, Sherif M. Soaida
-
Korean J Anesthesiol. 2023;76(3):194-202.
-
Clinical Research Article
October 24, 2022
|
-
Survival analysis: Part II — applied clinical data analysis
- Junyong In, Dong Kyu Lee
-
Korean J Anesthesiol. 2023;76(1):84-85.
Corrects: Korean J Anesthesiol 2019 10; 72(5): 441
-
Corrigendum
January 4, 2023
|
-
 Effect of total intravenous versus inhalation anesthesia on long-term oncological outcomes in patients undergoing curative resection for early-stage non-small cell lung cancer: a retrospective cohort study[commentary-article]
Effect of total intravenous versus inhalation anesthesia on long-term oncological outcomes in patients undergoing curative resection for early-stage non-small cell lung cancer: a retrospective cohort study[commentary-article]
- Kwon Hui Seo, Ji Hyung Hong, Mi Hyoung Moon, Wonjung Hwang, Sea-Won Lee, Jin Young Chon, Hyejin Kwon, Sook Hee Hong, Sukil Kim
-
Korean J Anesthesiol. 2023;76(4):336-347.
-
Clinical Research Article
December 28, 2022
|












")














")














