Introduction
The use of cardiac implantable electronic devices (CIEDs) has dramatically increased in recent years, resulting in substantially improved quality of life and increased survival of patients with cardiovascular disease. Consequently, more patients with CIEDs may be exposed to diseases requiring surgery or invasive procedures during their lifetime [1,2].
CIEDs utilized for rhythm management include the permanent pacemaker (PPM) for control of bradyarrhythmias, implantable cardioverter defibrillator (ICD) for treatment of lifeŌĆÉthreatening ventricular arrhythmias, cardiac resynchronization therapy-pacemaker/defibrillator (CRTŌĆÉP/CRTŌĆÉD) for treatment of heart failure with dyssynchronization, and implantable loop recorder (ILR) for monitoring cardiac arrhythmias.
The presence of these devices may present a problem during procedures that could expose the patient to electromagnetic interference (EMI), leading to inappropriate device functioning. Thus, precautions should be followed prior to performing these types of procedures to ensure the safe management of patients with CIEDs.
This review provides an overview of the perioperative management of patients with CIEDs and a discussion of the various responses of CIEDs to the application of a magnet according to the device manufacturer, type, and programming.
Indications for device implantation and nomenclature
Permanent pacemaker
Indications for pacemaker insertion include symptomatic bradycardia caused by atrioventricular block (AVB) and sick sinus syndrome. AVB is classi’¼üed according to the extent of the delay (’¼ürst degree: PR interval prolongation > 200 ms) or interruption (second degree: intermittent interruption or third degree: complete interruption) of electrical conduction between the atria and ventricle. Several congenital or acquired etiological factors can cause deterioration of the atrioventricular conduction system, leading to AVB [3]. AVB occurs most commonly in the absence of significant cardiac disease and is generally attributed to idiopathic fibrosis of the conduction system [4]. Other causes of acquired AVB include iatrogenic, infectious, infiltrative, autoimmune, or ischemic processes [5ŌĆō9]. Sinus node dysfunction with intermittent loss of P-waves or sinus arrest causing symptomatic episodes is known as sick sinus syndrome.
Leadless pacemaker
A leadless pacemaker, which is a novel alternative consisting of a capsule-like device containing a generator and an electrode system, is implanted into the right ventricle through the femoral vein. By eliminating the need for transvenous leads and a generator pocket, a leadless pacemaker can be placed in patients with subclavian venous stenotic disease and thus may help prevent lead- and pocket-related complications.
Implantable cardioverter de’¼übrillators
The indications for ICD implantation can be divided into primary and secondary prevention. Primary prevention indicates prevention of sudden cardiac death in patients with symptomatic heart failure and left ventricular ejection fraction Ōēż 35% after optimal medical therapy [10]. In most cases, ICDs are implanted for secondary prevention in patients who have survived a cardiac arrest or intolerable ventricular arrhythmias. Patients with heart failure or congenital heart disease or post-myocardial infarction are selected for ICD implantation. Patients with familial cardiac conditions, such as long QT syndrome, Brugada syndrome, or hypertrophic cardiomyopathy, are also at a high risk of sudden death due to ventricular arrhythmias. A small proportion of ICDs are subcutaneous ICDs, which are typically implanted in the left midaxillary region. Subcutaneous ICDs do not require leads located within the heart and offer no conventional pacing support [11,12].
Cardiac resynchronization therapy-pacemaker/defibrillator
Cardiac dyssynchronization is defined as a difference in the timing of electrical and mechanical activation of the ventricles, which can result in impaired cardiac efficiency. The purpose of CRT is to increase cardiac output by simultaneous biventricular pacing [13]. The function of these devices is to coordinate ventricular contraction; thus, they are programmed to ensure continuous pacing of the heart. For patients at risk of ventricular arrhythmias with indications for biventricular pacemakers, specialized ICDs that enable CRT are also available [14]. These devices, which are predominantly inserted for primary prevention, are known as CRT-D.
Implantable loop recorder
ILRs are small devices implanted or injected subcutaneously under local anesthesia in the left side of the chest. With an ILR, a patientŌĆÖs electrocardiogram (ECG) is continuously recorded and deleted by the deviceŌĆÖs retrospective memory and can be stored during syncope or significant arrhythmia [15]. ILRs can be useful for diagnosing arrhythmias in patients with potentially life-threatening symptoms, such as unexplained syncope.
CIED nomenclature
The nomenclature for pacemakers established by the North American Society of Pacing and Electrophysiology (NASPE) and the British Pacing and Electrophysiology Group (BPEG) is designated as the NBG code for pacing nomenclature [16]. The code consists of up to five letters (Table 1). Positions 1ŌĆō3 refer to the chamber-paced, chamber-sensed, and response-to-sensing positions, respectively. The fourth position of the generic PPM code is rate-responsive pacing, whereby the paced heart rate can be altered by the CIED in response to motion or detection of physiological conditions. Importantly, all modern ICDs and CRTs also include pacemaker functions. Most commonly, activity during exertion is detected by an accelerometer, which increases the paced rate to optimize cardiac output. Other sensing mechanisms may detect an increase in physiological parameters, including minute ventilation or myocardial contractility, and adjust the heart rate accordingly. The fifth position is used to indicate the presence of multisite pacing.
Considerations for patients with CIEDs before surgical or invasive procedures
Electromagnetic interference
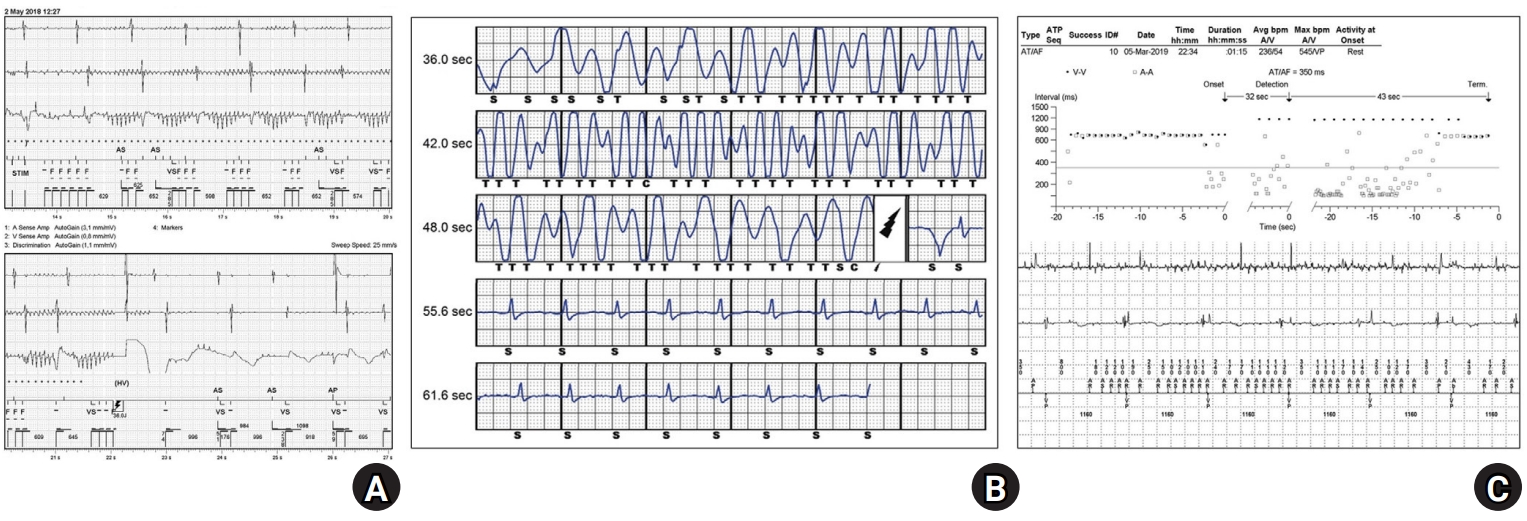
The combination of the electric and magnetic fields is known as the electromagnetic field. Electric fields exist in the presence of electrical charges. The flow of electric current in a conductor with magnetic field lines perpendicular to the current flow produces a magnetic field. EMI can occur as a result of conducted or radiated electromagnetic energy. EMI can also occur when an electronic device is exposed to an electromagnetic field. Oversensing of EMI by the device may cause pacing inhibition in patients with PPMs and inappropriate shocks in patients with ICDs. Fig. 1 shows some examples of adverse responses to EMI in patients with CIEDs. Two patients with ICDs (intravenous and subcutaneous) received inappropriate shocks due to EMI oversensing during external electronic stimulation therapy (Figs. 1A and B). In a patient with a pacemaker (DDD mode), atrial oversensing of EMI caused failure of ventricular tracking following atrial contraction, and the pacing mode was ultimately changed from DDD to VVI (Fig. 1C).
Potential sources of EMI in surgical settings include intraoperative magnetic resonance imaging, monopolar electrocautery [17], bipolar electrocautery [18], nerve stimulators [19], transcutaneous electrical nerve stimulation machines [20], argon plasma coagulation [21], and radiofrequency ablation devices [22].
Preoperative evaluation of patients with CIEDs
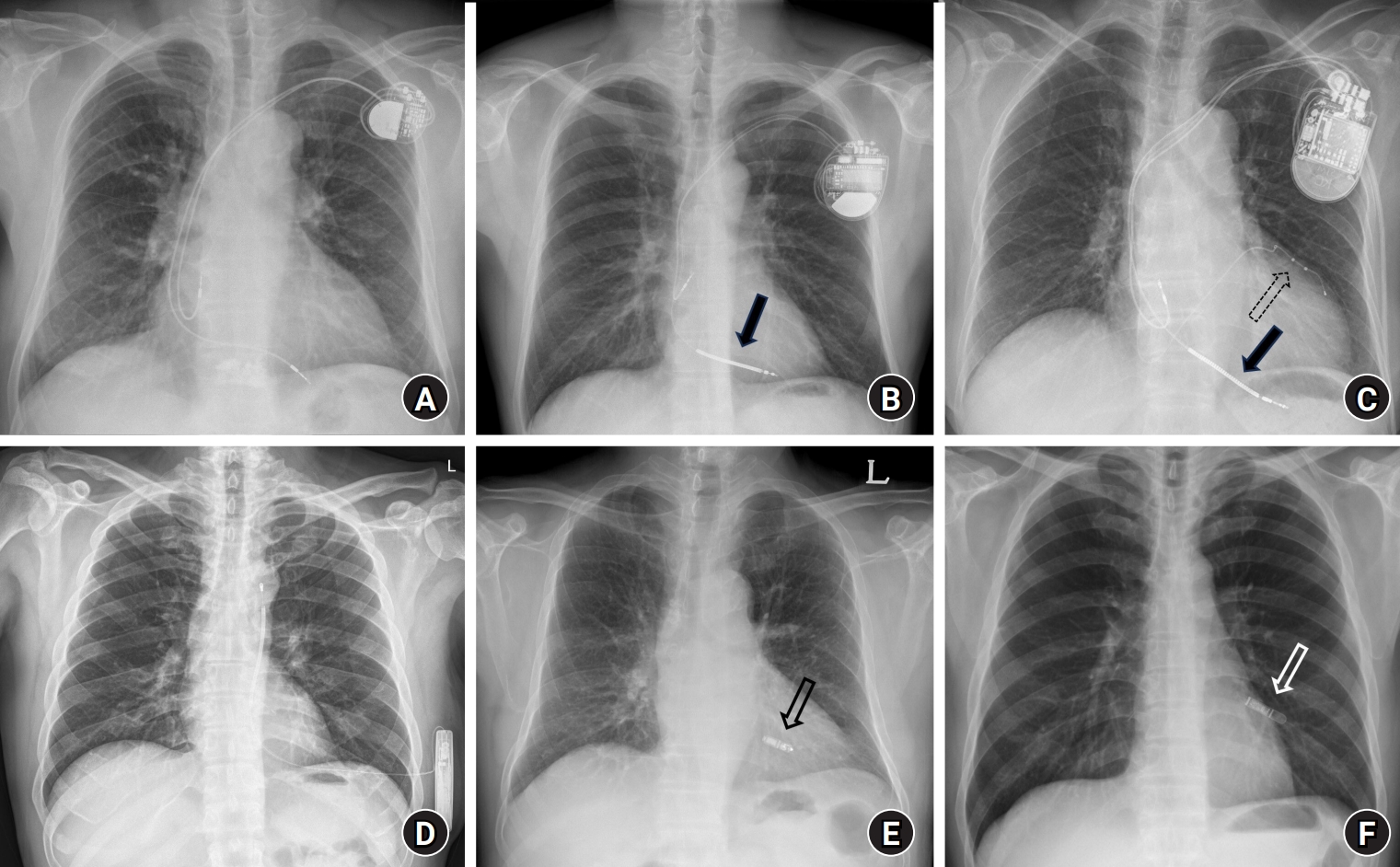
The preoperative evaluation of patients with CIEDs should include both a multidisciplinary and systematic approach. The manufacturerŌĆÖs identification card should be obtained from each patient. The device identification card contains the date of implantation, type of CIED, and type of leads. A chest X-ray should be examined to confirm the device type and location of the generator and leads (Fig. 2). In general, the right ventricular lead of an ICD includes one or two thick radio-opaque sections representing high-voltage coils for the delivery of shock energy. A CRT device has two ventricular leads (one located in the right ventricle and the other that enters the coronary sinus and travels towards the lateral side of the left ventricle). A 12-lead ECG should be performed to determine baseline rhythm and pacing spikes. If pacemaker spikes are observed in front of all or most P-waves and/or QRS complexes, pacemaker dependency should be considered. Medical records should be reviewed for the device type, manufacturer, and indication for implantation. The CIED should be examined before surgery if this has not been performed electively during the preceding 12 months for PPM (6 months for ICD/CRT) or when battery longevity is unknown [14]. The patient should be informed about the potential risk of EMI during the procedure, and preventative measures should be taken in accordance with the needs and preferences of the patient. During the preoperative evaluation of a patient with a CIED, surgical information, including the type of procedure, location of the surgical site, patient position during the procedure, source of EMI, and anatomic location of EMI delivery, should be provided to the CIED team (defined as the physician, nurse, and technicians who care for the patientŌĆÖs CIED).
Clinical status affecting risk of arrhythmia or device function
Most patients with CIEDs have underlying structural heart disease, significant intrinsic rhythm abnormalities, and risk of arrhythmias and thus are at an increased risk of developing fatal arrhythmias during the perioperative period. Additionally, depending on the type of procedure performed and the presence of significant fluid shifts, electrolyte and acid-base alterations, and hemodynamic deterioration of anesthetics, myocardial ischemia may occur and further increase the patientŌĆÖs susceptibility to fatal arrhythmias.
Several cases have suggested that the pacing threshold of CIEDs increase during surgery, resulting in pacing failure. This is associated with various pathological conditions, including myocardial ischemia, acid-base disturbances, electrolyte abnormalities, and elevated plasma concentrations of antiarrhythmic drugs as well as the local injection of sodium channel blockers (e.g., bupivacaine, lidocaine) [23ŌĆō25].
Pacing dependence
In general, no intrinsic rhythm > 40 beats/min will be detected in patients with pacemaker dependency or the patient will have a hemodynamically unstable rhythm. However, pacemaker dependency is complex. Although no standard definition currently exists, pacemaker dependency can be described as the abrupt cessation of pacing resulting in the development of bradycardia-related symptoms or signs that lead to an emergent or urgent clinical situation [26]. Note that patients who are not usually pacemaker-dependent may become dependent intraoperatively (e.g., with sedation, direct or indirect vagal stimulation, certain high-potency opiates, other anesthetics, or other pharmacological agents) [26].
Intraoperative management of patients with CIEDs
General considerations
Patients with CIEDs are susceptible to both local and systemic infections. An association between CIED infections and increased mortality has been reported [27]; therefore, the use of ipsilateral central lines should be minimized. In cases of CIEDs placed less than three months prior, insertion and removal of the pulmonary artery catheter or central line should be performed under fluoroscopic guidance to prevent dislodgement of the lead. In addition, care should be taken to avoid advancement of the guidewire into the right ventricle, which could cause artifacts resulting in the delivery of an inappropriate ICD shock.
As most patients with ICDs typically exhibit impaired cardiac function and are potentially at risk of developing malignant arrhythmias, anesthetic management should be customized based on baseline left ventricular systolic function. In patients with heart failure, heart rate is considered a crucial factor affecting myocardial oxygen demand. An increased heart rate reduces the time spent in diastole, leading to premature cessation of diastole and decreased ventricular filling, causing a mismatch between supply and demand. This discrepancy can result in ischemia and malignant arrhythmia. It is essential to consider factors that may precipitate tachycardia, such as intubation, surgical stimuli, hypovolemia, anemia, hypoxia, hypercapnia, and postoperative pain.
Defibrillation patch
External defibrillation therapy should always be available in the preoperative setting. Defibrillator pads should be placed in an anteriorŌĆōposterior electrode position at a distance Ōēź 8 cm from the implanted device; never directly over the device itself. CIEDs rarely result in permanent damage by direct current cardioversion/defibrillation [28]. If cardioversion or defibrillation is performed, the device should be reprogrammed immediately after surgery.
Cardiac monitoring in the operating or procedure room
Intraoperative monitoring of patients with CIEDs is more complex than that of patients without CIEDs. The objective of intraoperative monitoring is to provide a safe environment for patients with a CIED undergoing a surgical or interventional procedure with expected EMI. Anesthesiologists should be aware of the potential limitations of ECG monitoring, such as heart rate overestimation due to double counting of the pacing spike and QRS complex. The use of intraoperative monitoring equipment can help prevent the misinterpretation of ECG artifacts as intrinsic QRS complexes. The monitoring process may include pulse palpation, auscultation of heart sounds, intra-arterial pressure curve monitoring, pulse plethysmography, and/or oximetry.
Diagnosing myocardial ischemia in patients who are unable to report chest pain due to general anesthesia is challenging. Diagnosing ischemic heart disease via ECG is particularly difficult in patients with CIEDs given the presence of ventricular paced rhythms [29].
Perioperative CIED management
CIED-related problems during surgery
Appropriate pacing may be inhibited by a pacemaker sensing EMI, as the device can incorrectly interpret EMI as an intrinsic cardiac rhythm. In patients with pacemaker dependency, EMI may lead to oversensing (interpreted as myocardial electrical activity) and inappropriate inhibition of pacing, with a risk of asystole. In addition, when a CIED uses a vibration sensor or minute ventilation sensor (impedance-based rate-responsive pacing function), manual ventilation for pre-oxygenation or manipulation of the device can be sensed by the CIED, resulting in inappropriate high-rate pacing, although this is unlikely to cause any clinical harm. In patients with an ICD, EMI may induce inappropriate anti-tachycardia pacing (ATP) or shock therapy, causing the patient to move suddenly, possibly at a critical moment during surgery [30,31]. Additionally, ventricular arrhythmia could occur with possible fatal outcomes in these patients [32].
PPM and ICD manufacturers either prohibit the use of surgical electrocautery or have issued strong warnings, particularly for the monopolar (most frequently used) mode of operation. Despite the minor risks associated with EMI, bipolar electrocautery should be considered (as opposed to monopolar electrocautery), wherever possible. If monopolar electrocautery is used at a site remote from the device, with the dispersive electrodes located away from the area of the device generator and leads, the current pathway does not pass through the device generator and leads. Thus, the risk of any effect on the device that may cause inappropriate functioning is low [33].
ILRs monitor cardiac signals but do not provide therapies. Patients with ILRs who undergo surgical procedures are not at risk. When using the device, EMI may be interpreted as a rapid heart rhythm and recorded as an episode of tachyarrhythmia. However, this can be easily determined by examining the device. No additional precautions are required for patients with an ILR. However, elective examination of the device before the procedure and clearing of the diagnostic memory after the procedure may be useful if the memory is filled with episodes of detected EMI.
Magnet application
Magnets have been used during the perioperative period to convert PPMs into an asynchronous pacing mode at a rate of 80ŌĆō100 beats/min (Table 2) and to turn off the tachycardia treatment of an ICD (Table 3). However, the magnetic response can vary depending on the CIED, manufacturer, and individual settings determined by the CIED team.
For PPMs, when applying the magnet, reprogramming is performed automatically in an asynchronous pacing mode (AOO, VOO, DOO). This means that the PPM is ŌĆśneglectingŌĆÖ impulses that are being sensed and paced. The rate at which PPM pacing occurs during magnet application depends on the manufacturer and the battery life of the generator. If the battery life is low, PPM pacing will occur at lower rates, which may not be adequate in the perioperative period. Higher pacing rates may be required for patients with PPMs who are undergoing major surgery than for those who typically require pacing in daily life. An increase in the heart rate is a normal response to decreased systemic vascular resistance and hypovolemia. However, the application of a magnet may place the patient in an asynchronous mode; therefore, the pacing rate may not meet the physiological demands of the patient.
This difference in function is critical when applying a magnet to an ICD versus a PPM. For ICDs, to prevent inappropriate treatment of tachycardia due to EMI oversensing, both ATP and defibrillation are deactivated by the application of a magnet. This has no effect on the pacing function of an ICD. Therefore, the application of a magnet to an ICD cannot cause the pacing function to shift into asynchronous mode. The effect of a magnet on an ICD can be programmed and can differ according to the manufacturer; thus, some ICDs do not exhibit typical behavior when a magnet is applied. Because this variation depends on the manufacturer and attending cardiologist, the effect of magnet application on each patientŌĆÖs device should be determined prior to any operative procedure whenever possible. Patients should be continuously monitored for possible spontaneous or surgical stress-induced ventricular arrhythmias when deactivating ICDs using a magnet.
Magnets should be available in all operating rooms or units where surgical or invasive procedures are performed. In addition, all staff members should know the location of the magnet, situations requiring its use, and how to use it. Leadless pacemakers do not respond to magnets with asynchronous pacing; therefore, programming changes must be performed using the programmer for the speci’¼üc device.
CIED reprogramming
EMI can cause CIED dysfunction, resulting in pacing failure in pacing-dependent patients with PPMs or CRT devices and inappropriate shocks in patients with ICDs. In general, determining whether to reprogram the CIED, place a magnet, or do nothing is the most important perioperative decision regarding a CIED. Although reprogramming the CIED is generally regarded as the most established method for managing patients with CIEDs, this can be a time- and resource-consuming process and may not be ideal in certain situations. In particular, hemodynamically unstable bradycardia due to EMI is rare in patients with PPMs without pacing dependence; thus, ECG monitoring during the procedure is sufficient. Pacing dependence is rare in patients with an ICD. However, for patients with pacing dependence who are exposed to EMI, the ICD must be deactivated and asynchronous pacing should be performed. The ICD cannot be programmed for asynchronous pacing when the ATP therapy is turned on.
Evidence indicates that CIED functioning is more likely to be affected by EMI when it is used near the generator or leads [34]. The greatest risk is associated with situations in which the current path crosses the CIED and/or leads. Therefore, the procedural site is the most important factor. During the perioperative period, reprogramming a CIED may not be necessary when EMI is not anticipated, bipolar electrocautery alone is used 15 cm away from the CIED [35], or when the procedural site is located below the umbilicus [36]. A postprocedural CIED checkup is usually not required in such cases. The suggested guidelines for reprogramming a CIED or applying a magnet in various clinical situations are listed in Table 4.
Troubleshooting
In cases of detectable inhibition of a PPM or evidence indicating that ICD shock therapy is being delivered, the surgeon should be informed immediately, and the use of equipment capable of producing EMI should be intermittent (breaks of 5 s between use) for short bursts (< 5 s) or discontinued [37]. The application of a magnet can also be considered. Therefore, it is important to establish a secondary method of pacing in the event of asystole. Alternative methods include transesophageal, transcutaneous, and transvenous pacing using a temporary cardiac pacing wire or a pacing pulmonary artery catheter. Regardless of the method chosen, all necessary equipment and support should be organized and available prior to starting the procedure.
Postoperative CIED management
Postoperative management of patients with CIEDs primarily involves the examination and restoration of device function. Ideally, patients with CIEDs should be managed in a postoperative recovery environment with continuous monitoring and the immediate availability of appropriate resuscitation equipment. The de’¼übrillator function of an ICD and any rate modulator pacing function of a PPM that has been suspended should be reactivated by the CIED team as soon as possible after the surgical procedure. The device should be checked at the earliest opportunity if a magnet is used for intraoperative CIED deactivation or in the event of significant arrhythmic events. Device interrogation should be performed before the patient leaves the monitored environment. Precautions should be followed during the perioperative period even if the procedure does not cause EMI. The recommendations for pre-, intra-, and postoperative CIED management are summarized in Table 5.
Conclusion
The perioperative management of patients with CIEDs can be challenging because of the potential for EMI-induced device malfunction. To avoid CIED-related perioperative complications, the indication for device implantation should be assessed and clinicians should have a thorough understanding of perioperative management of CIEDs, including magnet application and device reprogramming. This review describes potential indications for device implantation, presurgical considerations, and the perioperative management of patients with CIEDs. We hope that this review will be helpful to anesthesiologists involved in the perioperative management of CIEDs.