Introduction
Surgical resection is the mainstay of treatment for solid cancers. However, surgery can cause local tissue damage that activates the neuroendocrine and immune systems, and micrometastasis through the spread of cancer cells into the systemic circulation [1,2]. Similar to surgery, anesthetics also play a crucial role in this pathophysiology [3ã5]. Anesthetic agents can affect immunomodulation, metabolic pathways, and cancer progression through various mechanisms; therefore, they may be associated with long-term oncological prognosis [3,6,7]. Propofol has more favorable anti-tumor effects than inhalation agents with respect to recurrence-free survival (RFS) and overall survival (OS) in patients undergoing major cancer surgery for gastroesophageal, colorectal, and hepatobiliary cancers [3,6,8ã10]. Additionally, preclinical studies have shown that propofol can suppress the growth, invasion, and metastasis of cancer cells as well as promote apoptosis [11,12]; contrastingly, volatile anesthetics have inconsistent effects on the metastasis and invasion of cancer cells [13ã15].
Lung cancer is among the most common cancers worldwide [16]. The main subtypes of lung cancer are small-cell and non-small cell lung cancers (NSCLC), and NSCLC accounts for approximately 80%ã85% of all lung cancer diagnoses. According to US statistics, the five-year relative survival rate for lung and bronchial cancer is approximately 61.2% for local cancer. However, it remarkably decreases when cancer metastasizes to local lymph nodes (33.5%) or distant metastases (7%) [17]. Curative resection for lung cancer is one of the major lengthy surgeries; furthermore, all patients should undergo one-lung ventilation that can induce physiological and pathological alterations [4]. However, the effects of anesthetics on lung cancer prognosis remain unclear. Previous studies have assessed a relatively small sample size, or an inhomogeneous patient population diagnosed with stage IãIV NSCLC [18ã20]. Moreover, the patients included in these studies could have had residual confounders. Validated data analysis using large-scale cohorts may reliably determine the anti-tumor protective effects of propofol in patients undergoing surgical resection for NSCLC.
Therefore, we aimed to compare RFS and OS between propofol-based total intravenous anesthesia (TIVA) and volatile agent-based inhalation anesthesia in patients undergoing curative resection for stage I or II NSCLC in a larger cohort than those in previous studies. In addition, we aimed to investigate the clinical factors affecting long-term oncological outcomes. We hypothesized that compared with volatile agent-based inhalation anesthesia, propofol TIVA allowed improved OS and RFS in patients with stage I or II NSCLC.
Materials and Methods
This study was approved by the Institutional Review Board of the Catholic University Seoul St. Maryãs Hospital (approval number: PC20RISI0031; date: March 19, 2020) that waived the requirement for informed consent, as this was a retrospective analysis. This study was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Study population
We reviewed the electronic medical records of all patients who were diagnosed with stage I or II NSCLC and underwent curative resection through video-assisted thoracoscopy (VAT) or thoracotomy (such as pneumonectomy, lobectomy, segmentectomy, and wedge resection) at a tertiary care teaching hospital between January 2010 and December 2017 (follow-up closure: May 1, 2021). The exclusion criteria were as follows: (1) primary cancer in other organs, except for cervical carcinoma in situ, treated basal cell carcinoma, superficial bladder tumors (Ta, Tis, and T1), or any cancer curatively treated less than three years before enrolment; (2) pathologic staging M1 or N3; (3) incomplete resection; (4) loss to follow-up within five postoperative years; (5) death within one month due to surgery-related complications; (6) occurrence of other primary cancers within five postoperative years; (7) incomplete medical records; (8) administration of both intravenous and inhalation anesthetics; (9) American Society of Anesthesiologists (ASA) physical status more than IV and unknown anesthesia type; and (10) administration of the same anesthesia type for multiple surgeries during the study period.
Anesthetic technique
Patients were grouped according to whether they received propofol-based TIVA (TIVA group) or inhalation anesthesia (Inhalation group) for lung cancer surgery. The type of anesthesia was chosen at the discretion of the attending anesthesiologist. Patients in the TIVA group underwent continuous administration of propofol (target effect-site concentration: 3ã6 ö¥g/ml) and remifentanil (target effect-site concentration: 2.5ã4.5 ng/ml) via a target-controlled infusion pump. Patients in the Inhalation group received either sevoflurane 1.5ã2.5 vol% or desflurane 4ã8 vol% with 50%ã100% oxygen in the air and continuous remifentanil infusion (0.02ã0.15 ö¥g/kg/min).
Although the anesthetics used were different (volatile agents vs. propofol), patients in both groups received similar general care. Regional anesthesia for analgesia was not administered during the study period. None of the patients received nitrous oxide. For hemodynamic and fluid management, conventional variables, including heart rate, continuous arterial pressure, central venous pressure, and urine output, were measured.
Variables and outcome measurements
All data relating to the procedure and anesthesia were obtained from hospital electronic medical records. Specifically, we retrospectively collected the following data: date of surgery, anesthetic technique, ASA physical status, age at the time of surgery, sex, body mass index (BMI), smoking history, comorbid diseases, operation title (lobectomy, segmentectomy, wedge resection, pneumonectomy, and others), location of primary cancer, postoperative stage, primary tumor size, surgical resection margin, intraoperative packed red cells (PRC) transfusion, anesthesia time, postoperative ventilator care, and the presence of distant metastasis at the time of surgery. We categorized the operations as sub-lobectomy, lobectomy, and pneumonectomy. Less invasive operations than lobectomy were defined as sub-lobectomy that included segmental and wedge resection. Pneumonectomy included pneumonectomy with modified lymph node dissection, pneumonectomy with pleurolysis, and pneumonectomy with pulmonary artery angioplasty.
The primary study endpoint was the between-group comparison of long-term oncological outcomes, including RFS and OS, after lung cancer surgery. OS was defined as the period from the date of curative surgery to the date of death, while RFS was defined as the period from the date of surgery to the date of recurrence or death. The secondary endpoint was the investigation of other clinical factors, including anesthesia type that affected RFS and OS.
Statistical analysis
Patient characteristics and surgery type were described using numbers and proportions for categorical variables and medians with ranges for continuous variables. Between-group comparisons of continuous and categorical variables were performed using the t-test and ü2 test, respectively. Cox proportional hazards regression analysis was performed to obtain the hazard ratio (HR) and 95% CI of prognostic factors for RFS and OS. Multivariable analysis was conducted with factors significant in the univariate analysis to examine their independent association with RFS and OS. Additionally, between-group comparisons of OS and RFS were made using the Kaplan-Meier method and tested using the log-rank test. Statistical significance was set at P < 0.05. All statistical analyses were performed using SPSSôÛ software (version 24.0; SPSS Inc., USA) for WindowsôÛ (Microsoft Corp., USA).
Results
Patients, tumor, and surgical characteristics
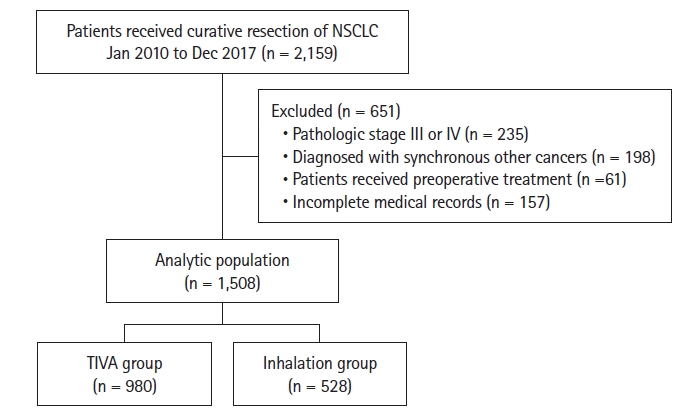
Among 2,159 patients who underwent curative-intent resection for NSCLC between January 2010 and December 2017, we included 1,508 patients diagnosed with stage I/II NSCLC (TIVA group, n = 980; Inhalation group, n = 528) (Fig. 1).
Baseline characteristics were well balanced between the groups (Table 1). There was male predominance; moreover, two-thirds of the patients had a BMI < 25. Most patients had an ASA physical status of I or II. The proportion of patients with underlying diseases, including hypertension, diabetes mellitus (DM), chronic obstructive pulmonary disease (COPD), ischemic heart disease, and cerebrovascular disease, was similar to that in the general population. More than two-thirds of the patients had stage I NSCLC. Most patients (84.7%) underwent VAT surgery, and the proportion of patients was not significantly different between the two groups (839 [85.6%] in the TIVA group and 438 [83.0%] in the Inhalation group, P = 0.178). The anesthesia time was less than 3 h in more than 90% of cases. More patients in the TIVA group underwent postoperative ventilator care (n = 82 [8.37%] in the TIVA group, n = 9 [1.70%] in the Inhalation group; P < 0.001).
The median follow-up periods in the TIVA and Inhalation groups were 73.7 months (53.1, 99.9) and 73.5 months (36.3, 99.5), respectively. The overall mortality rates in the TIVA and Inhalation groups were 22.4% and 30.1%, respectively. The proportions of recurrence and death in the TIVA and Inhalation groups were 28.8% and 35.2%, respectively.
The effect of anesthesia type on survival outcomes
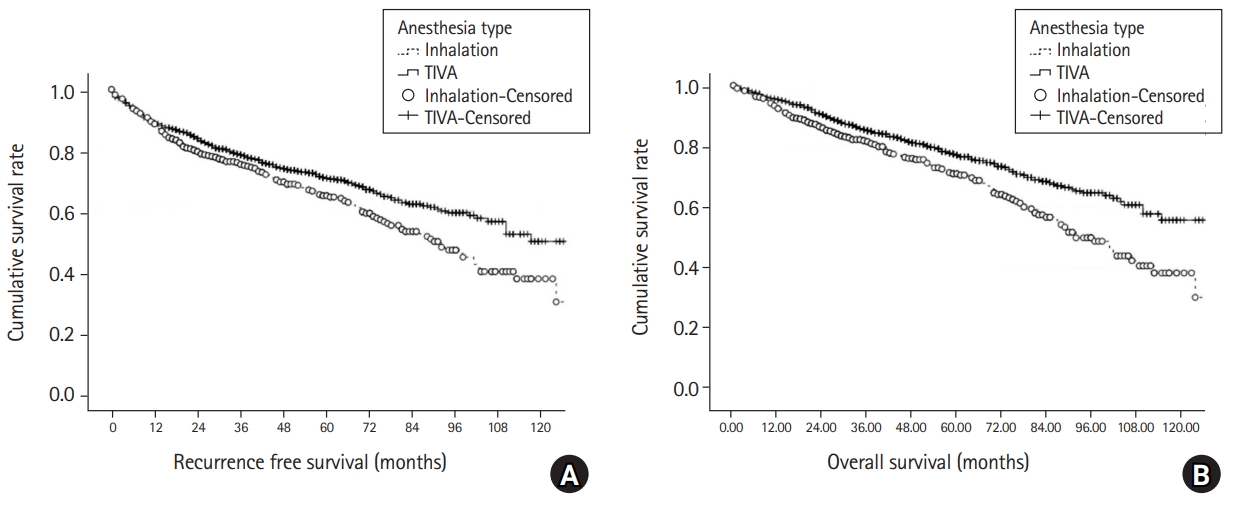
In the univariate analysis, anesthesia type was significantly associated with RFS. Among the factors significantly associated with RFS in the univariate analysis, age, sex, BMI, DM, COPD, cancer stage, intraoperative PRC transfusion, and anesthesia type were significant factors in the multivariate analysis (Table 2). Patients in the Inhalation group had a more than 20% higher risk of recurrence than patients in the TIVA group that was significantly different. Additionally, the tumor, nodes, and metastases (TNM) stage was a strong independent prognostic factor affecting recurrence. Older patients showed more frequent recurrences (> 30%) than younger patients. Male patients had a 27% higher risk of recurrence than female patients. The presence of underlying diseases, including DM and COPD, independently affected recurrence rates. The five-year RFS rates were 67% and 59% in the TIVA and Inhalation groups, respectively. The TIVA group had better RFS (7.7 years, 95% CI [7.37, 8.02]) than the Inhalation group (6.8 years, 95% CI [6.30, 7.22], P = 0.003) (Fig. 2A).
Moreover, anesthesia type was independently associated with OS in the multivariate analysis (Table 3). The Inhalation group showed a nearly 40% higher mortality risk than the TIVA group. ASA physical status and resection margin were other independent prognostic factors for OS in the multivariable analysis. The TIVA group showed a longer median OS (8.4 years, 95% CI [8.08, 8.69]) than the Inhalation group (7.3 years, 95% CI [6.81, 7.71], P < 0.001). The five-year OS rates were 74% and 65% in the TIVA and Inhalation groups, respectively (Fig. 2B).
Discussion
This study demonstrated that compared with inhalation anesthesia, propofol-based TIVA was associated with improved RFS and OS rates in patients who underwent curative resection for stage I/II NSCLC. Both RFS and OS were approximately one year longer in the TIVA group than in the Inhalation group. In addition to anesthetic agents, older age, male sex, BMI > 25, DM, COPD, a higher TNM stage, and intraoperative PRC transfusion were significantly associated with RFS. Moreover, ASA physical status and resection margin involvement were significantly associated with OS.
There have been numerous studies on the effects of different anesthetic types, including propofol and volatile agents, on long-term outcomes of cancer surgeries [3,5,6,8ã10,21]. It is difficult to conclusively determine the relationship between anesthetics and cancer recurrence or survival, considering the wide range of cancer types and patient conditions. Therefore, it is important to investigate the distinct effects of anesthetics on different cancer types. According to recent meta-analyses, the anesthetic type influences long-term outcomes in patients undergoing major surgery for hepatobiliary and gastroesophageal cancer with high surgical stress [3,5]. Contrastingly, anesthesia type was not associated with survival in patients who underwent less invasive surgery for cancers such as breast cancer or gliomas [3,5].
During lung cancer surgery, major physiological changes, including respiratory stress and activation of inflammation and immune response, can occur due to one-lung ventilation and surgical stimulation [4]. Therefore, anesthetics may affect the outcome of lung cancer surgery. However, the optimal anesthetic for one-lung ventilation and pulmonary resection of lung cancer remains unclear [4,22]. Regarding one-lung ventilation-induced pathophysiology, propofol could be beneficial since it decreases the intraoperative shunt and maintains oxygenation better than inhalation anesthetics. Contrastingly, a few studies have reported that inhalation anesthetics exerted better anti-inflammatory properties than propofol [4,23]. Lee et al. [22] investigated the short-term prognosis of patients with lung cancer who underwent propofol-based TIVA or inhalation anesthesia for anatomical lung resection. They found that patients who received propofol-based TIVA had shorter hospital and intensive care unit stays as well as chest tube indwelling durations than patients who received inhalation anesthesia; however, there was no significant between-group difference in 30-day postoperative mortality [22]. In long-term prognosis, propofol TIVA was associated with better OS and RFS than inhalation anesthesia in patients with esophageal cancer who underwent one-lung ventilation [8]. For patients with NSCLC, there have been inconsistent reports on the effects of propofol-based TIVA on OS or RFS in patients undergoing surgical resection [18ã20]. A study on 943 Korean patients indicated that propofol-based TIVA did not affect OS or RFS in patients with stage IãIV NSCLC [20]. However, more than a quarter of the patients presented lymph node metastasis and showed a remarkable increase in the HR for recurrence or death with the pathological stage in their study. The outcomes of advanced-stage NSCLC may be highly influenced by additional chemotherapy or radiation therapy before and after surgery that impedes the evaluation of the independent effects of anesthetics during radical resection. Furthermore, a recent multicenter study including 746 patients with stage IãIII NSCLC reported that OS and cancer-specific survival did not differ between patients who underwent propofol-based TIVA and inhalation anesthesia [18]. However, their study cohort only included open thoracotomy, had a relatively short mean follow-up period (3.65 years), and did not consider the patientsã underlying disease. Another study on 230 patients with pathologic stage I NSCLC reported a significantly longer RFS in patients who underwent propofol-based TIVA than in those who underwent inhalation anesthesia [19]. This is in line with our findings; however, compared with our study, this previous study had a shorter follow-up period and a relatively smaller sample. This study included a larger number of consecutive patients and more homogenous groups with a longer follow-up period than the previous studies.
We found that propofol-based TIVA improved both OS and RFS that is consistent with the results in several preclinical reports. Propofol plays a role in inhibiting cell proliferation, migration, and invasion; further, it promotes apoptosis in various tumor cells by regulating the expression of various signaling pathway components and micro- and long non-coding RNAs [7,11]. In NSCLC cells, exposure to propofol increases the activity of the extracellular signal-regulated kinase 1/2 dependent p53-upregulated modulator of the apoptosis signaling pathway that decreases cell viability and promotes cell apoptosis [24]. Furthermore, propofol inhibits cell invasion by reducing hypoxia-inducible factor 1öÝ expression in lipopolysaccharide-treated NSCLC cells [25]. In addition, propofol upregulates the expression of micro-RNA (miR)-486 and miR-1284 as well as downregulates the expression of miR-372 in NSCLC cells that inhibits cell growth, migration, and invasion [25ã27]. However, there have been inconsistent reports regarding the effects of inhalation anesthetics on NSCLC cells. Isoflurane activates the Akt-mTOR signaling pathway; further, it promotes the proliferation, migration, and invasiveness of NSCLC cells, resulting in pro-tumor effects [15]. Exposure of Lewis lung carcinoma cells to sevoflurane promotes cell proliferation in vitro [28]. However, another in vitro study reported that sevoflurane exerts antitumor effects by inhibiting the proliferation and invasion of lung adenocarcinoma cells and enhancing apoptosis by regulating the long-chain RNA PCAT6/miR-326/Wnt5a/öý-catenin axis [29]. A recent prospective clinical study reported that compared with sevoflurane anesthesia, propofol anesthesia could decrease the serum concentration of tumor angiogenesis-related factors, including vascular endothelial growth factor and transforming growth factor beta, in patients undergoing radical resection of NSCLC that indicates that propofol exerts anti-tumor effects [30]. Therefore, there is a need for prospective clinical studies on biomarkers or miRNA expression to elucidate the exact mechanism underlying the effects of propofol or volatile anesthetics on oncologic outcomes. Our findings could provide evidence for future prospective randomized multicenter studies.
In our study, the five-year RFS rates were 67% and 59% in the TIVA and Inhalation groups, respectively, while the corresponding values for the five-year OS rates were 74% and 65%. Patients in the TIVA group showed approximately one year longer RFS and OS than those in the Inhalation group. A previous study on stage I NSCLC showed similar results; however, both the five-year RFS (91.7% and 77.4% in the TIVA and Inhalation groups, respectively) and OS rates (94.4% and 83.5% in the TIVA and Inhalation groups, respectively) were higher than those in our study, as the patients had a lower cancer stage [19]. Another study on patients with stage IãIII NSCLC showed no difference in the five-year cancer-specific survival rate between the TIVA (68.1%) and the Inhalation groups (70.8%) [18]. Although we did not investigate cancer-specific survival, we analyzed data regarding longer follow-up periods and observed between-group differences in the number of years of survival. Our findings could be evidence for the selection of anesthetics not only during general anesthesia but also during sedation for intervention, ventilator care, and radiological examination in patients with NSCLC.
Several perioperative factors other than the anesthesia type can affect the long-term outcomes of cancer surgery. Previous studies have reported that not only advanced cancer stages and lymph node invasion but also demographic characteristics such as male sex and older age were commonly associated with RFS or OS in patients undergoing resection for NSCLC [19,20]. Regarding anesthesia-related factors, surgery, anesthesia time, and intraoperative PRC transfusion are associated with recurrence and death [20]. Our findings are similar to previous findings; however, DM and COPD were independent factors related to both RFS and OS. As an anesthesia-related factor, intraoperative PRC transfusion was associated with both RFS and OS. Perioperative blood transfusion modulates the immune system that increases the risk of cancer recurrence and mortality [31,32]. Previous studies on esophageal, digestive, and other mixed cancer types have also reported that perioperative blood transfusion was associated with worse OS and RFS [6,8,33].
This study has several limitations. First, this was a retrospective, single-center study. Additionally, the choice of anesthetic was not standardized. Both sampling and selection biases may have influenced our findings. Therefore, our findings should be interpreted with caution. Second, we did not evaluate postoperative acute respiratory or renal complications, sepsis, or other organ injuries that could affect long-term outcomes. A previous study on patients with stage I NSCLC suggested that postoperative pulmonary complications were significantly associated with OS, but not RFS, as indicated by multivariate analysis [19]. However, another prospective, multicenter study on morbidity and mortality in lung surgery reported no difference in the rates of major complications during the hospital stay and at six postoperative months between patients who received propofol and those who received inhaled anesthesia [34]. Additionally, Oh et al. [20] reported that postoperative complications were not associated with recurrence or death in patients with stage IãIV NSCLC. Further studies are warranted to address this issue. Third, although analgesia could affect metastatic recurrence [32], we did not consider factors regarding perioperative pain control, including opioids and NSAID use. However, two previous studies reported that the number of opioids or systemic opioid use was not associated with the recurrence risk and mortality in patients with NSCLC [18,35]. Finally, although we performed multivariable analyses and the baseline characteristics were balanced between both groups, there could have been other unmeasured confounders.
In conclusion, propofol-based TIVA was associated with better RFS and OS than was inhalation agents in patients with stage I/II NSCLC who underwent curative resection. Our findings could inform future prospective randomized multicenter studies.