-
Risk factors for chloral hydrate sedation failure in pediatric patients: a retrospective analysis
- Young-Eun Jang, Jung-Bin Park, Pyoyoon Kang, Sang-Hwan Ji, Eun-Hee Kim, Ji-Hyun Lee, Hee-Soo Kim, Jin-Tae Kim
-
[Epub ahead of print]
-
Clinical Research Article
July 2, 2024
|
-
Effect of lipid emulsion on vasoconstriction induced by epinephrine or norepinephrine in isolated rat aorta
- Soo Hee Lee, Kyeong-Eon Park, Kibaek Eum, Yeran Hwang, Seong-Ho Ok, Gyujin Sim, Dumidu Perera, Henri K. Ravald, Youngho Park, Susanne K. Wiedmer, et al.
-
[Epub ahead of print]
-
Experimental Research Article
June 25, 2024
|
-
Venous air emboli during esophagoscopy confirmed by computed tomographic pulmonary angiography -a case report-
- Thadakorn Tantisarasart, Thara Tantichamnankul, Chanatthee Kitsiripant, Panjai Choochuen
-
[Epub ahead of print]
Corrects: Korean J Anesthesiol 2024 4; 77(2): 278
-
Corrigendum
June 25, 2024
|
-
Utilization of the pericapsular nerve group block in preoperative rehabilitation of patients with femoral neck fractures: a case series
- Zhuan Jin, Daisuke Sugiyama, Fumiya Higo, Takahiro Hirata, Osamu Kobayashi, Hiroshi Morimatsu, Kenichi Ueda
-
[Epub ahead of print]
-
Case Report
June 19, 2024
|
-
The effects of sugammadex on isolated human internal mammary artery and saphenous vein rings
- Mert C. Ongun, Bahar Oc, Mehmet Oc, Hulagu Bariskaner
-
[Epub ahead of print]
-
Letter to the Editor
May 22, 2024
|
-
Response to letter
- Byungjin Choi, Ah Ran Oh, Jungchan Park, Seunghwa Lee
-
[Epub ahead of print]
-
Letter to the Editor
May 20, 2024
|
-
Effect of perioperative intravenous ibuprofen versus acetaminophen on postoperative opioid consumption and pain after general anesthesia: a systematic review and meta-analysis with trial sequential analysis of randomized controlled trials
- Sung Hye Kim, Hyun Kang, In-Jung Jun, Hye Won Park, Byung Hoon Yoo, Yun-Hee Lim, Kye-Min Kim
-
[Epub ahead of print]
-
Clinical Research Article
May 7, 2024
|
-
Comparison of remimazolam and desflurane in emergence agitation after general anesthesia for nasal surgery: a prospective randomized controlled study
- Sung-Ae Cho, So-min Ahn, Woojin Kwon, Tae-Yun Sung
-
[Epub ahead of print]
-
Clinical Research Article
May 7, 2024
|
-
Renal implications of pneumoperitoneum in laparoscopic surgery: mechanisms, risk factors, and preventive strategies
- Gianluca Villa, Marco Fiorentino, Eleonora Cappellini, Sergio Lassola, Silvia De Rosa
-
[Epub ahead of print]
-
Review Article
April 26, 2024
|
-
Response to "Comment on Comparison of the pericapsular nerve group block with the intra-articular and quadratus lumborum blocks in primary total hip arthroplasty: a randomized controlled trial"
- Tayfun Et, Muhammet Korkusuz
-
[Epub ahead of print]
-
Letter to the Editor
April 25, 2024
|
-
Assessment of fluid infusion rate using a pulse oximeter: a pilot study
- Yeiheum Park, Sungho Moon
-
[Epub ahead of print]
-
Letter to the Editor
April 24, 2024
|
-
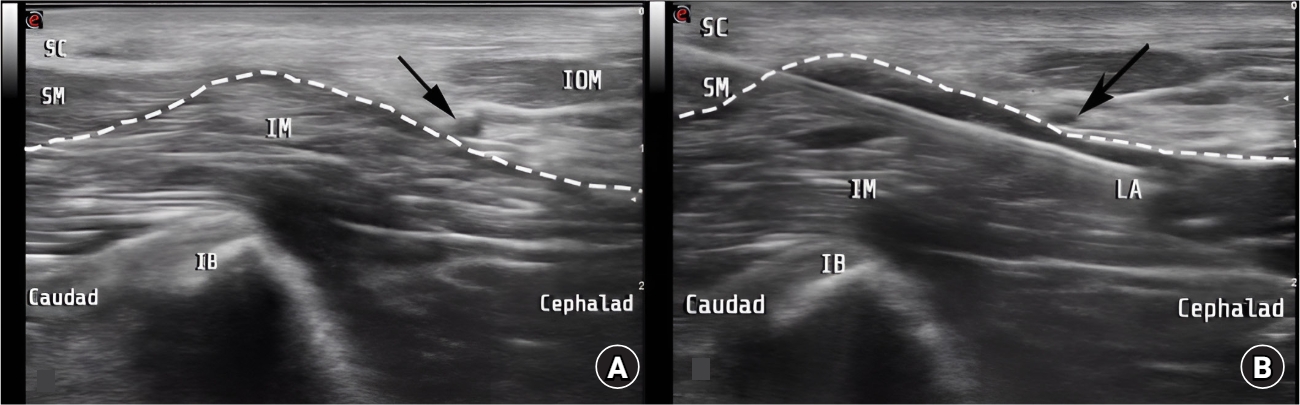
Ultrasound mapping of soft tissue vascular anatomy proximal to the larynx: a prospective cohort study
- Alessandro De Cassai, Margherita Iuzzolino, Silvia De Pinto, Giovanni Zecchino, Tommaso Pettenuzzo, Annalisa Boscolo, Eugenio Biamonte, Paolo Navalesi, Marina Munari
-
[Epub ahead of print]
-
Clinical Research Article
April 23, 2024
|
-
The incidences of nausea and vomiting after general anesthesia with remimazolam versus sevoflurane: a prospective randomized controlled trial
- Yeong Min Yoo, Jae Hong Park, Ki Hwa Lee, Ah Hyeon Yi, Tae Kyun Kim
-
[Epub ahead of print]
-
Clinical Research Article
April 19, 2024
|
-
Retro superior costotransverse ligament space block as an effective analgesia after laparoscopic gastrectomy -a case report-
- Youngin Lee, Seunguk Bang, Jihyun Chung, Jookyoung Moon
-
[Epub ahead of print]
-
Case Report
April 15, 2024
|
-
Postoperative neurocognitive disorders in ambulatory surgery: a narrative review
- Junyong In, Brian Chen, Hansu Bae, Sakura Kinjo
-
[Epub ahead of print]
-
Review Article
April 3, 2024
|
-
Damage-associated molecular patterns as a mechanism of sevoflurane-induced neuroinflammation in neonatal rodents
- Young-Eun Joe, Ji Hae Jun, Ju Eun Oh, Jeong-Rim Lee
-
[Epub ahead of print]
-
Experimental Research Article
April 1, 2024
|
-
Tranexamic acid - a promising hemostatic agent with limitations: a narrative review
- Dong Joon Kim, Su Yeon Cho, Ki Tae Jung
-
[Epub ahead of print]
-
Review Article
August 21, 2023
|
-
Robot-assisted radical prostatectomy: comparison of subarachnoid analgesia, erector spine plane block, and intravenous analgesia for postoperative pain management
- Pasquale Buonanno, Nicola Logrieco, Annachiara Marra, Lorenzo Spirito, Gianluigi Califano, Federica Blasio, Nausica Di Falco, Achille Aveta, Gianluca Spena, Giuseppe Servillo
-
[Epub ahead of print]
-
Clinical Research Article
June 14, 2023
|
-
WITHDRAWN:Smartphones are definitely a boon in operation theatre if used smartly enough
- Anju Gupta, Nishkarsh Gupta
-
[Epub ahead of print]
-
Letter to the Editor
June 20, 2019
|












")














")














