Ultrasound-guided regional anesthesia (USGRA) is commonly performed with B-mode (2D) imaging using high-frequency linear array and low-frequency curved array transducers. With biplane imaging (BI), phased array and high-frequency curved array (endocavity) transducers are available to evaluate cardiac and fetal anatomy and for needle guidance during transrectal procedures. BI capabilities have recently been incorporated into high-frequency linear transducers, making BI technology available for USGRA. During a peripheral nerve block (PNB), real-time BI eliminates the need to rotate the transducer to obtain both short-and long-axis views of the nerves, vessels, bones, muscles, or fascial planes. In addition, the needle is displayed in-plane and out-of-plane, and the spread of the local anesthetic can be visualized in two orthogonal planes simultaneously. Using BI for USGRA can decrease procedure time and the number of attempts and needle passes, improve block success and quality, and maximize safety by mitigating the risk of unintended intraneural, intrapleural, and intravascular injection. We report the novel use of BI for USGRA of the thorax, abdomen, and upper and lower extremities.
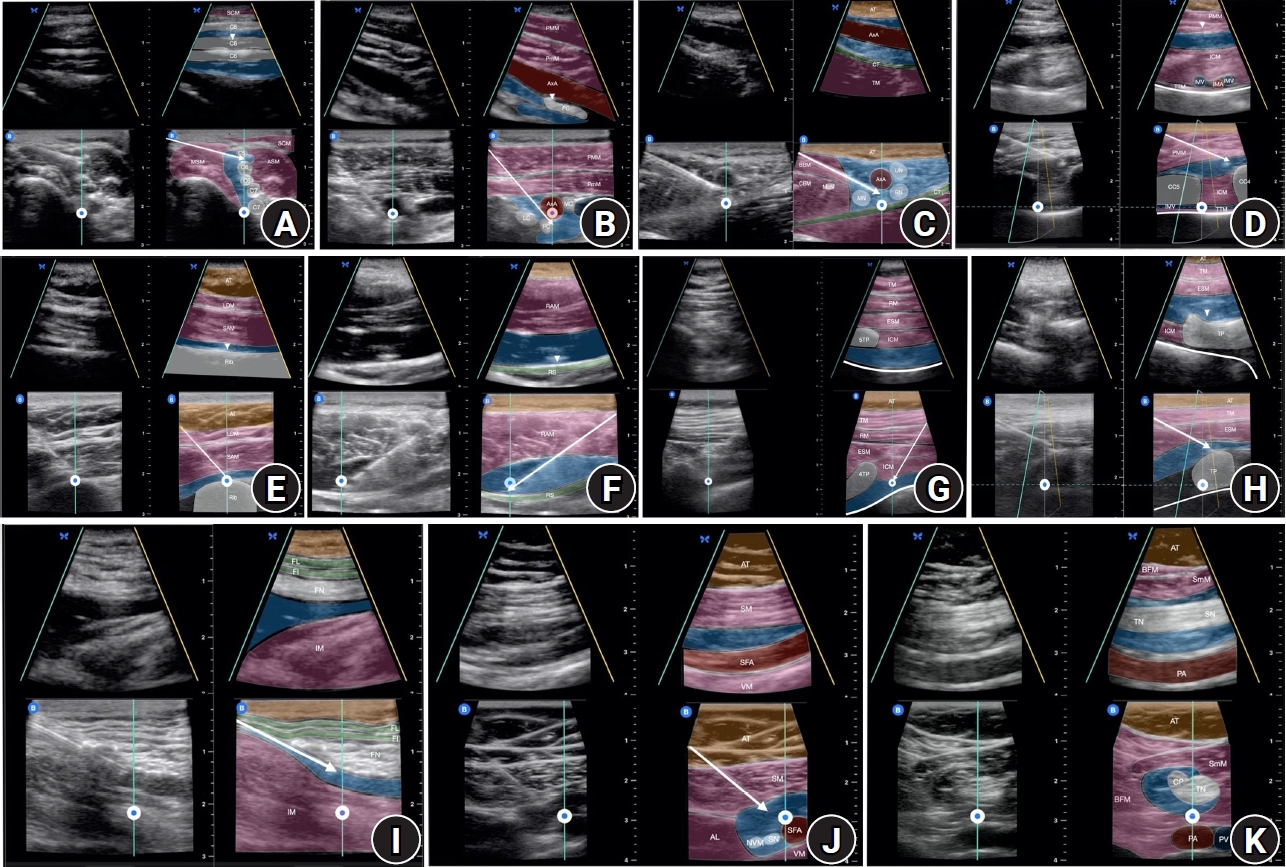
This technical report was exempt from internal review board approval since patient identifiable information were removed per institutional policies at the University of Texas Health Science Center at Houston and Memorial Hermann Hospital System, USA. Deidentified images were obtained from a regional anesthesia image bank. The highest quality images from each major region of the body were selected. Upper extremity biplane USGRA images, which are shown in Figs. 1AŌĆō1C, include interscalene, infraclavicular, and axillary brachial plexus blocks. Images of truncal fascial plane blocks are presented in Figs. 1DŌĆō1F, which include the superficial parasternal block, deep serratus plane block, and rectus sheath block. Figs. 1G and 1H highlight the high thoracic paravertebral block and the low thoracic erector spinae plane block. Finally, lower extremity biplane USGRA images of the femoral nerve block, distal femoral triangle block and popliteal sciatic nerve block are depicted in Figs. 1IŌĆō1K.
The Butterfly IQ+ (Butterfly Network, Inc., USA) ultrasound attached to either an iPhone 11 (iPhone 11 Pro-Butterfly iQ app) or a fifth generation iPad mini (iPad Butterfly iQ app) was utilized to perform biplane USGRA. The standard B-mode image (reference plane) is displayed at the bottom of the screen, while the orthogonal plane that correlates to the curser (perpendicular plane) is shown at the top of the screen. The transducer was positioned to be simultaneously perpendicular to the object of interest in the short axis and parallel in the long axis to ensure optimal BI. A 20ŌĆō22 gauge blunt-tip 50ŌĆō100 mm echogenic block needle (B Braun Ultraplex 360, USA) or 18-gauge SonoTAP Tuohy needle (PAJUNK GmbH Medizintechnologie, Germany) was advanced to the target location for each block using the reference plane and an in-plane technique. The biplane cursor was placed over the needle tip for visualization in the short-axis view, on the neurovascular structures to obtain images of the entire nerve or artery in the long-axis view, and/or bone, muscle, or fascial planes of interest to obtain an orthogonal view. The biplanar spread of the local anesthetic was observed upon injection.
BI can be activated at any time; however, due to the reduced screen size and image quality, we recommend timing it on a case-by-case basis. For superficial blocks, where needle visualization is less challenging, BI can be activated when the optimal monoplane image is obtained in B-mode. For deeper blocks, where needle localization is more difficult to confirm sonographically, we recommend advancing the needle in B-mode and activating BI once the needle tip is in the desired location to improve the accuracy and visualization of the local anesthetic injectate as it spreads orthogonally through the tissue planes.
The use of BI for superficial ultrasound-guided (USG) vascular access has been reported using low- and high-frequency matrix transducers. One study concluded that the enhanced visualization of structures and needles leads to improved performance and feasibility. For internal jugular vein (IJV) cannulation using the short-axis approach, applying BI with a low-frequency matrix transducer resulted in fewer puncture attempts and needle redirections, a lower incidence of posterior wall punctures, and successful puncture of the IJV on the first attempt in 90% of cases vs. 50% with B-mode [1]. The low-frequency transducer used in this study, which is designed for imaging large, superficial vascular structures, is acceptable for IJV cannulation; however, it provides suboptimal visualization of small superficial structures, such as nerve roots for USGRA [2]. For the case presented by Convissar et al. [3], a semiconductor-based ultrasound with a high-frequency setting (vascular) was used to perform radial artery cannulation with BI. To date, this case is the only report of BI needle-guidance for high-frequency ultrasound. The use of BI for USGRA has not previously been reported. Therefore, in this study, we included images of the USG PNB and fascial plane blocks using the novel application of a high-frequency ultrasound transducer (Figs. 1AŌĆō1K).
The spread of injectate following the PNB was studied through cadaveric dissection after dye or radiologic contrast injections. However, this type of study has been criticized since postmortem alterations in tissue integrity could affect the patterns of injectate spread and may not accurately represent clinical situations. In the clinical setting, arterial pulsations, muscle contractions, respirations, and differences in tissue resistance can influence the spread of local anesthetics [4]. Although BI technology is not currently available in the most common ultrasound systems used for USGRA, enhanced imaging may improve our understanding of sonoanatomy and the spread of local anesthesia. In 2019, a high-frequency matrix linear array piezoelectric transducer was introduced into the market for vascular applications (Philips XL 14-3 mMatrix, Netherlands). In 2020, BI for a high-frequency handheld ultrasound became commercially available (Butterfly Network, Inc., USA). Rapid technological advances in ultrasound coupled with the potential for enhanced superficial imaging might lead to a future where matrix 3- and 4-dimensional imaging for USGRA is the standard.
BI is a new feature in high-frequency matrix ultrasound transducers that can improve needle localization and enhance visualization of local anesthetic spread during USGRA. We reported on the novel application of BI for USGRA. More studies are needed to assess the utility of BI in USGRA and evaluate its impact on the safety and delivery of regional anesthesia.