Introduction
Regional anesthesia (RA) techniques have been shown to reduce perioperative opioid requirements [1], postoperative length of stay [2,3], and positively impact long-term outcomes such as the risk of persistent postsurgical pain (PPSP) [4], morbidity, and mortality [5]. RA is thus an important component of multimodal anesthetic and analgesic strategies. However, rebound pain after RA is increasingly recognized as an adverse effect [6] that can compromise analgesic benefit. This phenomenon is incompletely understood but appears more evident with RA techniques designed to provide surgical anesthesia or to otherwise completely abolish pain perception well into the early postoperative period; most commonly, single-injection peripheral nerve blockade (PNB) [2,7,8]. In this article we will provide an overview of our current understanding of rebound pain, discuss prevention strategies, and provide practical recommendations for the management of acute postoperative pain arising after the use of RA.
Definition and characteristics of rebound pain
Several definitions of rebound pain have been published in the literature (Table 1). The essential characteristics of rebound pain are that it (1) is acute postoperative pain, (2) ensues following resolution of PNB, and (3) is clinically significant [9], either with regard to the intensity of pain or the impact on psychological well-being, quality of recovery, and activities of daily living. Rebound pain frequently occurs at night [10,11] but this is likely related to the 8 to 12 h duration of most single-injection PNB and the fact that most elective surgery is completed during daytime hours [12]. Rebound pain is also often described as ŌĆśburningŌĆÖ in nature [9] but lacks other neuropathic features such as allodynia. It often remains severe for 2ŌĆō6 h, but the subsequent pain trajectory is consistent with the expected recovery and healing process from the surgical insult. Rebound pain is therefore a transient phenomenon and distinct from PPSP [13].
Does rebound pain represent a RA-induced state of hyperalgesia?
A fundamental question is whether rebound pain merely represents an unmasking of the expected nociceptive response in the absence of adequate systemic analgesia, or if it reflects an exaggerated nociceptive response for which RA may be partially responsible. Hyperalgesia to heat stimuli has in fact been documented after PNB in animal studies. Subparaneural sciatic nerve blockade with ropivacaine in rats induced transient heat hyperalgesia of their hindpaws that lasted 5ŌĆō7 h after sensory block resolution [14]. Similar findings have been reported in subsequent animal studies [15,16]. However, the clinical significance of the intensity and duration of this hyperalgesic response is questionable. It is also unclear if these findings are generalizable to human subjects. As previously mentioned, although patients receiving PNB often describe the subsequent breakthrough pain as having ŌĆśburningŌĆÖ characteristics [9], this does not necessarily reflect the presence of heat hyperalgesia as described in animal studies [14ŌĆō16].
Hyperalgesia as a normal response to tissue injury
More importantly, hyperalgesia to heat stimuli occurs as a consequence of surgical trauma even in the absence of RA, and is part of a well-recognized spectrum of post-incisional primary hyperalgesia that can last up to 7 days after surgery [17]. Secondary hyperalgesia is a similar response that occurs in the uninjured tissue surrounding the site of trauma. This represents the general phenomenon of peripheral sensitization to pain that is a normal physiologic response [18]. Tissue injury initiates a local inflammatory cascade, and the various inflammatory mediators (e.g., calcitonin gene-related peptide, cyclooxygenase [COX]-1, COX-2, prostaglandins [PGE], cytokines, interleukines, neurotrophins) activate peripheral nociceptors both at the site of injury and in surrounding tissues [19].
The effect of RA on pathways of pain perception
RA, and more specifically PNB, prevents the perception of pain by blocking impulse propagation in peripheral nerves from tissue nociceptors to second-order neurons in the dorsal horn of the spinal cord, and onward via ascending pathways in the lateral spinothalamic tract and subsequent thalamocortical pathways in the brain. As a result, RA will inhibit central sensitization to pain that is upregulation of the activity and responsiveness of spinal dorsal horn neurons [17,20]. However, PNB will not have a significant effect on peripheral sensitization, and this inflammatory process will continue unabated in the absence of systemically-administered medications [18]. Therefore, as peripheral neural blockade resolves, the nociceptive input from the hyperalgesic area at the site of injury will become apparent as rebound pain. This distinction between the effect of RA on peripheral and central sensitization may also be responsible for the lack of any observed association between acute rebound pain and the subsequent development of PPSP.
Potential pro-nociceptive effects of local anesthetics
Laboratory research in cellular and animal models has reported several effects of local anesthetic administration that may affect acute nociception. Mice receiving sciatic nerve block with bupivacaine had microscopic evidence of early-phase peripheral nerve injury secondary to Wallerian degeneration and axonal demyelination [21]. Local anesthetics have also been implicated in neurotoxicity [22,23] and cytotoxicity [24] via disruption of mitochondrial membrane potentials and release of cytochrome C, accompanied by activation of caspases ultimately leading to cell apoptosis [24,25]. Proinflammatory effects such as COX-2 gene expression and subsequent increases in PGE2 production at the surgical site, as well as in cerebrospinal fluid, have been documented after local infiltration [26] and intrathecal [27] administration of bupivacaine, respectively. However, pain resulting from structural damage to neural tissue would be expected to be more prolonged than is typical of rebound pain. The relevance of these experimentally-derived neurotoxic and proinflammatory effects of local anesthetics to the clinical application of RA is therefore currently uncertain.
In summary, it appears unlikely that RA contributes to postoperative hyperalgesia to any clinically significant extent, and consequently it can be assumed that rebound pain does not represent an exaggerated nociceptive physiological response.
Is there a significant difference in the pain trajectory of patients who receive RA versus those who do not?
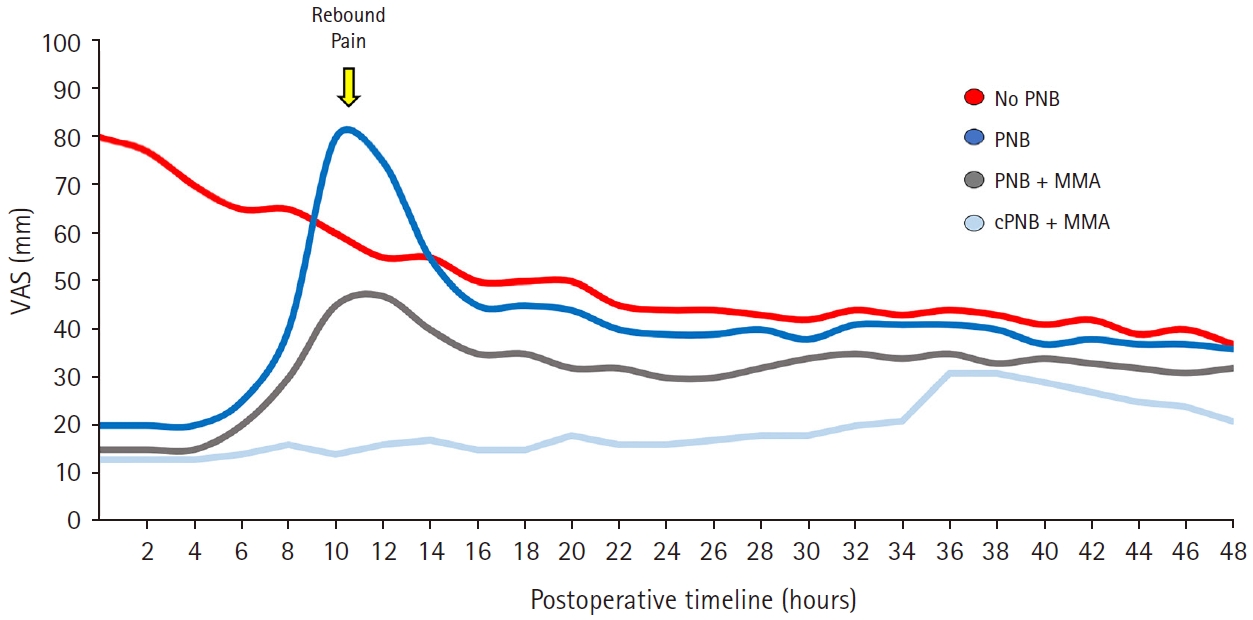
By definition, rebound pain is characterized by a delayed increase in patient-reported pain scores, often accompanied by increased analgesic consumption, that corresponds to the resolution of the analgesic effect of RA [28]. As discussed above, this does not necessarily reflect exaggerated hyperalgesia. It is instead largely related to the unexpected termination of conduction blockade and unmasking of the nociceptive response to surgery in the absence of adequate systemic analgesia [13,29]. This is in fact analogous to the situation in which a patient emerges from general anesthesia (GA) and abruptly becomes aware of wound pain ŌĆō initial pain scores on admission to the postoperative care unit (PACU) are often high, and then decline as the patient receives appropriate analgesic therapy. Thus, the difference in pain trajectories between patients who receive RA and those who do not is largely a function of the timing of unmasking of the underlying acute post-surgical pain (Fig. 1).
The important question, therefore, is not whether there is a delayed peak in reported pain scores and opioid consumption, but rather, what the relative height of this peak is compared to the pain experienced after GA alone, and what factors may influence this. This can be quite variable. For example, in comparing patients undergoing shoulder surgery with or without PNB, multiple studies have reported increased pain scores between 12 and 24 h after single-injection interscalene blocks with ropivacaine [2,7,10,30,31] that roughly corresponds to the expected resolution time for this block (Table 2). A 2015 meta-analysis reported a statistically significant difference in rest pain scores 24 h postoperatively in favor of the GA-only group, but the mean difference was only 0.96 on a 0ŌĆō10 visual analog scale and thus of limited clinical significance [32]. Furthermore, pain scores and opioid consumption were lower or similar in both groups at all other time points and patients who received an interscalene block were more satisfied with their analgesia at 24 h.
A more marked difference in rebound pain scores, as reported in other studies of supraclavicular [13] and infraclavicular brachial plexus block [13,29] as well as lower extremity RA techniques [3], may be at least partially explained by the postoperative analgesic regimen in place. Patients who do not undergo RA receive carefully titrated analgesic medication in the PACU to achieve satisfactory analgesia as a condition of discharge, and this is maintained thereafter with further doses as needed. In contrast, patients who have had effective RA usually require and receive little to no additional analgesics in PACU prior to discharge. Pain scores will naturally rise as the sensory block wears off and may reach or even exceed the levels experienced by GA-only patients at emergence, if they do not receive timely or appropriate doses of systemic multimodal analgesics. Patients who receive RA thus usually have significantly lower cumulative opioid consumption in the first 12 h postoperatively, and this difference becomes less marked (but not higher) in the 24ŌĆō48 h time period [32].
Balanced against this evidence for the occurrence of rebound pain are several studies that report the opposite results: compared to no block, single-injection PNBs (e.g., femoral [33,34] or combined axillary/suprascapular [12]) actually result in decreased pain scores even after the effect has worn off, and may also decrease primary and secondary hyperalgesia [35]. How do we account for these widely disparate findings? An individualŌĆÖs pain trajectory and experience are clearly dependent not only on the analgesic strategy utilized, but also on the type of surgery [36] and patient factors. Pain is ultimately a subjective experience that is influenced to varying degrees by biological, social, and psychological factors [37].
Cognitive influences on rebound pain
Cognitive and other higher-order cortical processes exert a powerful influence on the perception of acute pain. A cognitive bias [38] is a systematic pattern of deviation from rational judgment [39] that may lead to perceptual distortion. In the ŌĆścontrast effectŌĆÖ bias, a given stimulus is perceived as more intense when it is contrasted with a prior stimulus of lower intensity. The abrupt appearance of pain after a period of relative comfort, as the effect of a PNB wears off, can, therefore, cause a patient to rate the intensity of rebound pain higher than usual.
Patient expectations can also significantly influence pain perception [40ŌĆō42]. Cumulative evidence shows that subjects who have been primed to expect good pain relief subsequently exhibit decreased pain perception and associated cerebral activity in response to noxious stimulation ŌĆō a phenomenon known as placebo analgesia [43ŌĆō47]. However, if the expectation of low pain intensity is not met, the disappointment may instead bias them towards reporting higher pain scores. This is relevant as patients who receive a PNB are often advised that they can expect excellent postoperative analgesia [13]; however, the finite duration of the sensory block may not be sufficiently emphasized and thus they are unpleasantly surprised by the pain that is unmasked.
What is the impact of rebound pain on other patient and health-related outcomes?
Poorly managed postoperative pain can result in adverse consequences including impaired quality of recovery, opioid dependence, PPSP, and increased medical costs [48]. It is therefore important to examine if rebound pain may have a significant impact on other health-related outcomes.
Patient satisfaction
Despite the issue of rebound pain, the use of RA for outpatient surgery results in increased patient satisfaction stemming from the avoidance of GA, effective postoperative analgesia with reduced opioid requirements, and decreased incidence of postoperative nausea and vomiting [49]. In a detailed study that interviewed patients who received PNB for ankle fracture surgery, Henningsen et al. [9] confirmed that despite the presence of rebound pain, patients reported high levels of satisfaction with RA and a preference for a similar technique in the future. These findings are mirrored in other studies that find that even though patients describe increased pain scores after PNB resolution, satisfaction scores remain high and similar to the GA-only group [2,8,50]. It, therefore, appears that from the patientŌĆÖs perspective, rebound pain does not outweigh the early postoperative benefits of a pain-free interval [49], reduced opioid consumption and side-effects, superior recovery profile, and a shorter time to readiness for discharge [2].
PPSP
Although poorly controlled acute postoperative pain has been implicated as a risk factor for the development of PPSP [51], there is no evidence to indicate that rebound pain per se predisposes to PPSP [13]. On the contrary, a recent Cochrane review reported that RA may instead reduce the incidence of PPSP after breast surgery and cesarean section [4]. As described above, the transitory nature of rebound pain, coupled with the early conduction block of nociceptive transmission, makes it unlikely that central sensitization will be exacerbated.
Healthcare resource utilization
Rebound pain after RA has been implicated in higher rates of unanticipated health care resource utilization [13]. A retrospective study of 195 patients undergoing surgery for wrist fracture reported a higher incidence of unplanned physician visits (12% vs. 4%) because of severe pain in the first 48 h by those who received RA versus GA [13]. This may be partly explained by the fact that RA patients were far less likely to have received opioid and non-opioid analgesics prior to discharge, and there was no systematic patient education plan in place regarding post-discharge management of the postoperative transition from RA to systemic analgesia. A negative impact of RA (and the associated rebound pain) on healthcare utilization was not however borne out in a much larger retrospective study of over 59,000 patients undergoing outpatient shoulder surgery [52]. Patients who received a PNB, in fact, had a significantly lower rate of unplanned admissions, readmissions, or emergency department visits (9% vs. 12%) in the first seven postoperative days. Nevertheless, it is only logical that risk factors for rebound pain should be identified when performing RA for individual patients and strategies should be implemented to prevent and mitigate any potential impact on their postoperative recovery. This will be the focus of the remainder of this article.
Which patients are at risk of rebound pain?
Patient factors
The presence of preoperative pain [53] and younger age have been identified as patient risk factors for severe acute postoperative pain and PPSP [54]. Both of these have also been associated with a predisposition to rebound pain. Patients with pre-existing joint pain were more likely to report rebound pain following the use of PNB in total hip or knee arthroplasty [53]. Rebound pain following ankle fracture surgery with PNB as the primary anesthetic was also more common and more severe in patients under 60 years of age [55]. The mechanisms for this are incompletely understood, but include age-related differences in deep tissue (muscle) and superficial tissue (skin) nociception [56], increases in sensitivity of peripheral nerves to local anesthetics, and cationic acceptor site availability to local anesthetics [57], along with lower peripheral nerve conduction velocities in the elderly [58].
Surgical factors
There is a perception that certain surgical procedures (e.g., shoulder, foot, and ankle) confer a higher risk of rebound pain. At present there is no data on the relative incidence of rebound pain among different surgeries; however, there are several logical contributing factors to consider. These include outpatient surgery, procedures associated with moderate-to-severe postoperative pain, and the use of single-injection PNBs (rather than continuous catheters) that provide near-complete analgesia [11,32]. Outpatient surgery patients are often discharged with a ŌĆśone size fits allŌĆÖ pain prescription that may be inadequate, and those who have received an effective single-injection PNB will usually have the first onset of breakthrough pain at home, where professional guidance and titration of analgesia is not available [13]. Patients often lack understanding of optimal medication dosing or timing and may also inappropriately limit the use of opioids at home because of fears of addiction or side-effects [13].
Regional anesthetic techniques
Rebound pain is a phenomenon that primarily manifests following PNB that provide dense sensory blockade (e.g., brachial plexus [2,7,10], popliteal sciatic [3,9] nerve blocks). Dramatic increases in pain scores and opioid consumption related to block offset are not usually seen in studies of fascial plane blocks such as transversus abdominis plane [59], pectoral nerves [60], erector spinae plane, [61] and quadratus lumborum [62,63] blocks. This requires further investigation for confirmation, but it may be related to factors that include a degree of visceral contribution to both pain and analgesic effect, an expectation of incomplete analgesic coverage by the block, and routine incorporation of these techniques into a multimodal analgesic regimen [64ŌĆō66].
Strategies for prevention of rebound pain
Continuous PNB catheter techniques
Extending the duration of sensory blockade to allow more time for healing and subsidence of the inflammatory process, as well as a less precipitous offset of block, should mitigate the impact of rebound pain. It is therefore not surprising that continuous catheter RA techniques with an infusion of dilute local anesthetic for 48 h or longer will preserve all of the early postoperative benefits of single-injection PNB while largely abolishing the phenomenon of rebound pain. Salviz et al. [67] randomized patients undergoing outpatient arthroscopic rotator cuff repair to receive GA alone, or GA combined with either a single-injection or continuous interscalene block. Compared to the GA-only group, both RA groups had shorter PACU stays, were discharged home earlier, and had a longer interval to first analgesic use. Most notably, the incidence of severe pain (8ŌĆō10/10 on a numerical rating scale) on the first postoperative day was only 15% in the continuous interscalene block group, compared to 78% and 40% in the single-injection and GA-only groups respectively. By the second postoperative day, the single-injection and GA-only groups had similar pain profiles, but the continuous catheter group continued to exhibit lower pain scores with only 10% reporting severe pain compared to 35% in the other two groups. A similar effect was reported for continuous versus single-injection popliteal sciatic PNB in patients undergoing ankle fracture surgery. The peak in pain score trajectory was both delayed and attenuated in the continuous catheter group, and at 48 and 72 h postoperatively, pain scores were similar in both groups. However, the overall value of outpatient PNB catheters is controversial [68]. Continuous RA techniques are technically more challenging to perform, have an inherent failure rate [69], are time and labor-intensive to manage, and consequently are likely to remain under-utilized in this setting [68].
Local anesthetic adjuncts in single-injection PNB
A more accessible alternative to continuous catheter techniques is the use of local anesthetic adjuncts to prolong the duration of single-injection PNBs. In a mouse model of sciatic nerve block with bupivacaine, the addition of perineural (but not intramuscular) dexamethasone prevented the appearance of a rebound hyperalgesic response to thermal stimulation [21]. Research indicates that perineural dexamethasone prevents bupivacaine-induced demyelination and Schwann cell degeneration [21], suggesting that any protective effect against rebound pain may be mediated by both anti-neurotoxic and anti-nociceptive mechanisms and effects. At present though, while it is well-established that dexamethasone (perineural more so than intravenous) [70] can prolong the analgesic benefit of PNB, there are no clinical studies specifically examining its impact on rebound pain per se.
Perineural buprenorphine is another local anesthetic adjunct used to prolong block duration, but again no studies have specifically investigated if it attenuates rebound pain compared to a control group. There is also a question of what constitutes an effective dose. In a retrospective cohort study describing their experience with a perineural combination of bupivacaine, clonidine, dexamethasone, and buprenorphine, Williams et al. [53] reported that a reduction in rebound pain after PNBs for total hip and knee arthroplasty was associated with > 300 ╬╝g buprenorphine but not lower doses.
Finally, although liposomal bupivacaine has been touted as an effective strategy to prolong the duration of analgesia (up to 72 h) with single-injection PNB [71], current evidence fails to support its routine use. Superior analgesia and opioid-sparing compared to conventional long-acting local anesthetics has not been demonstrated to date [72,73], and no studies have examined if it reduces the incidence and magnitude of rebound pain.
Multimodal analgesic regimens
As discussed above, PNB only blocks the transmission of nociceptive input to the spinal cord and higher centers. Peripheral sensitization and other physiological responses mediated by the humoral inflammatory response to surgery remain unaffected. Combining RA with systemic multimodal analgesia is therefore recommended for the potential additive or even synergistic benefits [74ŌĆō76] in improving postoperative pain and related outcomes. Nevertheless, many studies investigating rebound pain after PNB do not routinely incorporate perioperative systemic multimodal analgesia, and outpatient surgery patients usually receive significantly less analgesic medication prior to discharge [13,29,77].
Although there is no direct evidence that a consistent and comprehensive multimodal analgesic regimen will reduce rebound pain, it should be prescribed on a routine basis as part of good clinical practice [3,11ŌĆō13,29,67,78]. This should include a combination of acetaminophen, non-steroidal anti-inflammatory drugs/COX-2 inhibitors, and oral opioids [28,53,67,79ŌĆō81], in the absence of any patient or surgical contraindications.
Preoperative education and counseling
As already mentioned, patients and caregivers should be clearly informed about both the advantages and limitations of RA. Day surgery patients should receive preoperative education on the finite duration of analgesia provided by PNBs, and depending on the surgical procedure, should specifically be warned to expect moderate/severe pain commensurate with the surgical procedure as the block wears off. They should be instructed to begin taking analgesic medication earlier rather than later, with an emphasis on the 15ŌĆō20 min onset time for most oral analgesics versus the rapid offset of sensory block. A discussion of the expected interindividual variability [82] in block duration, pain thresholds, and response to analgesic therapy is also useful in assisting patients to self-titrate their medication. Supplementing verbal instructions with written or multimedia educational material will help improve compliance and lower perioperative anxiety and uncertainty [83].
Conclusion
Rebound pain is a transient perceptual phenomenon that occurs when the sensory blockade of RA resolves and unmasks ongoing nociceptive stimuli. Fortunately, in the majority of patients, it does not appear to significantly impact cumulative postoperative opioid consumption, quality of recovery, or patient satisfaction, and is not associated with longer-term sequelae such as PPSP. Rebound pain can, therefore, be viewed as a side-effect of RA but one that usually does not negate its favorable benefit-risk ratio. Nevertheless, rebound pain can cause acute distress and is an important consideration when formulating a perioperative management plan that involves RA, especially in outpatient surgery. Preoperative education is essential for setting appropriate patient expectations and coaching them on the importance of early preemptive initiation of systemic multimodal analgesia therapy. Prolonging the duration of action of PNB with continuous catheter techniques or with local anesthetic adjunctive medication may help alleviate rebound pain, although further research is required to confirm this.