Introduction
Since the Korean national insurance began to cover durable left ventricular assist device (LVAD) implantations in September 2018, the number of LVAD implantations performed in South Korea has been increasing [1]. The annual volume of LVAD implantations in South Korea has increased from 30 cases in 2018 to 61 in 2019, 58 in 2020, 82 in 2021, and 123 in 2022 per the Korean Society of Heart Failure Surgery. Considering the increasing volume of patients undergoing LVAD implantations and their improved longevity [2–4], the possibility of these patients requiring non-cardiac surgery has increased. Therefore, anesthesiologists need to understand the physiology of this unique patient population and adequately prepare for optimal perioperative management. According to the US Medicare data analysis, one in six patients with LVAD underwent various types of non-cardiac surgery [5]. In this review, we will cover perioperative considerations and intraoperative management of patients with implanted LVADs undergoing non-cardiac surgeries.
Types of left ventricular assist device (LVAD)
From the first implantation of an LVAD (the HeartMate II) in August 2012 until September 2020, the HeartMate II and HeartWare VAD (HVAD), were the most commonly implanted devices in Korean patients. After the HeartMate 3 was introduced in September 2020, the HVAD and HeartMate 3 became the most commonly implanted devices. However, in June 2021, the HVAD system was recalled as a result of safety concerns associated with potentially fatal pump malfunctions from electrical faults causing battery failure [6]. Therefore, the HeartMate 3 is currently the most commonly implanted LVAD in South Korea. Although patients scheduled for non-cardiac surgery are more likely to have third-generation devices (the HVAD or HeartMate 3) implanted, surviving patients who received their LVADs earlier may have any of these devices.
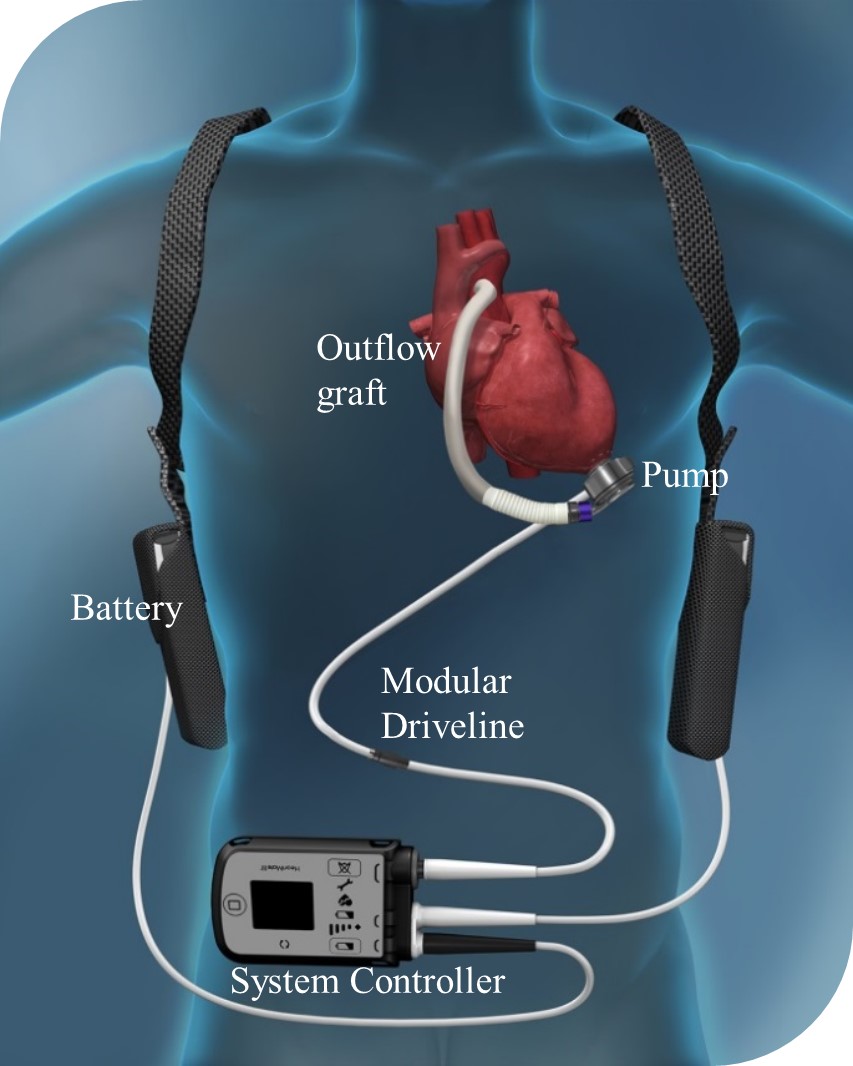
For an optimal hemodynamic profile or according to concerns regarding hemorrhagic or thrombotic complications, the recommended ranges for the device parameters differ according to the type of LVAD (Table 1, Fig. 1) [7,8]. Therefore, prior to surgery, physicians need to identify the type of device implanted in each patient scheduled for non-cardiac surgery. Details regarding the different types of LVADs have been described in previous articles [9–11].
Pump flow principle and basic physiology
The components of the HeartMate 3 LVAD are shown in Fig. 1. The volume flow rate generated by the LVAD is mainly determined by the pump speed and the pressure gradient across the pump. With the same afterload, the pump flow increases proportionally with a higher rotor speed, and at the same rotor speed, the pump flow is inversely related to the pressure gradient across the pump [11,12]. The pump speed can be adjusted; however, the surgeon usually sets a fixed value that is optimized to the patient. The recommended ranges for the pump speed (in revolutions per minute [RPM]) for each device type are listed in Table 1. The pressure gradient across the pump is the difference between the left ventricle (at the pump inlet) and aortic pressure (at the pump outlet). In situations where this pressure gradient increases, such as excessively high aortic blood pressure or reduced left ventricular filling, the pump flow decreases. Therefore, patients with LVADs have a preload-dependent and afterload-sensitive physiology. Afterload sensitivity means that, at any given speed, increased resistance (abrupt hypertension) can decrease the flow.
LVAD parameters
The four LVAD parameters are pump speed, power, flow, and the pulsatility index (PI) (Fig. 2A), and the recommended ranges are listed in Table 1. Each parameter is described in the following sections.
Speed
As briefly described above, the LVAD operates at a fixed speed (reported in RPM), and the recommended ranges differ according to the device type (Table 1). This fixed speed is determined or set by the physician, but it is not the same as a constant-speed mode. The HeartMate 3 in particular produces periodic variations in speed, generating an artificial pulse every two seconds (Fig. 2B).
Power and flow
While power (in watts [W]) is a direct measurement of pump motor voltage and current by the system controller, displayed flow (in liters per minute [L/min]) is an estimation based on power. The device power and flow generally exhibit a linear relationship at a given speed. Changes in pump speed, flow, or physiological demand can affect the pump power. Gradual increases in power (over hours or days) may indicate aortic insufficiency or thrombus deposits inside the pump. Gradual decreases in power may indicate an obstruction of flow and require evaluation. Occlusion of the flow path may decrease the flow through the pump and cause a decrease in power.
Pulsatility index (PI)
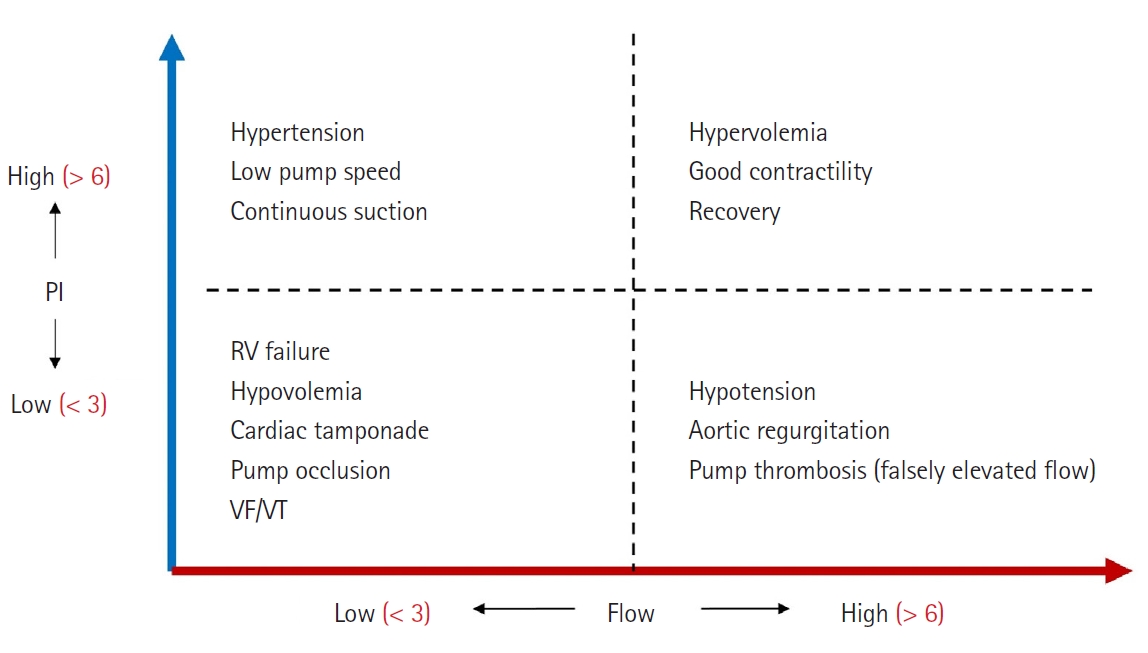
When the native left ventricle contracts during cardiac systole, the increase in ventricular pressure causes an increase in pump flow, and the magnitude of flow pulses through the pump is measured and averaged over 15 s intervals to produce the PI. The PI represents the degree of pump power variability (usually the same as the flow variability) and, ultimately, native heart contractility. Typical ranges of the PI values are shown in Table 1. In general, the magnitude of the PI is related to the amount of assistance provided by the LVAD pump. Higher values indicate greater ventricular filling and higher pulsatility (i.e., the LVAD provides less support to native heart contractility). Lower values indicate less ventricular filling and lower pulsatility (i.e., the LVAD provides greater support to unload the ventricle). The PI is useful in the management of patients with a HeartMate 3 implanted, particularly when combined with the pump flow (Fig. 3).
Preanesthesia assessment
Anesthetic considerations and preparations may vary depending on the type of non-cardiac surgery scheduled for the patient with an LVAD. Because LVADs only function effectively when the left ventricle is adequately filled by the right ventricle, preoperative assessment of right ventricular function, the presence of ventricular tachyarrhythmia, and the degree of pulmonary hypertension are crucial for identifying patients who need invasive monitoring (e.g., central venous catheters, pulmonary artery catheters, or transesophageal echocardiography [TEE]), early initiation of inotropic therapy, or other right ventricular optimization strategies (e.g., judicious volume therapy or ventilator setting adjustments) [12–14]. To facilitate awareness of any patient-specific or device-specific problems, preoperative discussions with knowledgeable clinicians (e.g., a specialized VAD team, if available) is important [12,15].
Device-related history
The LVAD-specific medical history must be reviewed, including the type of device, date of implantation, current device parameter values on the VAD monitor (pump speed, pump flow, pump power, and PI), and any previous LVAD-related alarms or events, such that the patient’s ideal flow parameters can be estimated. If the patient underwent aortic valve closure at the time of LVAD surgery because of aortic insufficiency, the patient’s native heart will not be able to generate any forward blood flow and will be completely dependent on the flow from the LVAD [10]. Additionally, the driveline and externalized abdominal site must be inspected for any signs of infection or perioperative changes.
Assessment of the overall condition
In addition to the severity and urgency of the current surgical problem, the degree of impairment in the function of any major organ; current medications; post-implantation complications; and most recent blood test results, including blood cell counts, electrolytes, coagulation, and renal and hepatic function tests, should be reviewed. The most recent echocardiography also provides vital information on cannula position and valvular and right ventricular function [3,9,11,12,16,17].
Management of cardiovascular implantable electronic devices
The main concern regarding the presence of cardiovascular implantable electronic devices (CIEDs) is the potential for interactions between the CIED and electromagnetic interference due to the intraoperative use of electrocautery [18]. Because up to 40% of patients with LVADs have a pacemaker or implantable cardioverter defibrillator, collectively known as CIEDs [4], deactivation should be planned before surgery to avoid inappropriate shocks in the operating room [19,20]. Deactivation may involve reprogramming the CIED to asynchronous pacing mode (VOO or DOO) or placing a magnet over the CIED. These patients require continuous 5-lead electrocardiography monitoring, and external adhesive defibrillation pads should be applied during the inactivation period [19].
Management of anticoagulation
Discontinuing anticoagulation therapy must be decided on a case-by-case basis, with the risk of bleeding weighed against the risk of a pump thrombus. Currently, anticoagulation with a vitamin K antagonist (warfarin) is recommended for patients with an LVAD, with a target international normalized ratio (INR) between 2.0 and 3.0 [21,22]. Aspirin can be added as antiplatelet therapy [21]. However, as an adverse effect of antithrombotic therapy, bleeding episodes, such as bleeding from the gastrointestinal tract, can occur in over 50% of patients with LVADs. As such events are most commonly associated with an INR > 2.5 [23], some centers have lowered the target INR to 2.0–2.5 for centrifugal pumps [24,25]. In addition, the development of acquired von Willebrand disease (vWD) also contributes to bleeding predisposition in patients with an LVAD. Acquired vWD is an acquired loss of large von Willebrand factor (vWF) monomers by increased proteolysis of vWFs, mediated by shear stress-induced amplification of vWF-cleaving protease (ADAMTS 13) [26,27]. This acquired vWD can prevent the binding of collagen and platelets at the sites of vascular injury [28].
If the risk of bleeding is low, aspirin and warfarin may be continued perioperatively or the goal may be decreased to the lower limit of therapeutic levels for most elective non-cardiac surgeries [21,29]. However, if the risk of bleeding is high, warfarin may be discontinued and bridged with heparin or heparin alternatives to be discontinued on the morning of the procedure [21,30]. For emergency, neurosurgical, or ophthalmologic surgeries, the anticoagulation effect may be rapidly reversed with fresh frozen plasma or prothrombin complex concentrate [16,29]. After the procedure, the early initiation of warfarin and antiplatelet therapy is recommended when the risk of surgical bleeding is acceptable [31].
Selection of anesthetic technique
Patients with an LVAD receive general anesthesia during most surgical procedures. However, if the surgical procedure can be performed under local anesthesia or an ultrasound-guided peripheral nerve block, sedation with monitored anesthetic care may be a safe option for upper- or lower-extremity surgeries. Although regional anesthesia is not inherently contraindicated in the presence of an LVAD, literature supporting the use of spinal anesthesia in patients with LVADs is extremely limited, and the use of neuraxial anesthesia is particularly infrequent (< 1%) [3,32,33]. The American Society of Regional Anesthesia recommends that the coagulation status be normalized before placing a neuraxial block [34]. When regional anesthesia is planned, interruption of warfarin therapy for five days before the elective procedure and normalization of the clotting status are recommended [32]. Another worrisome potential complication following neuraxial anesthesia is acute sympathectomy, which may provoke hemodynamic instability in patients with LVADs. Because these patients are dependent on adequate venous return, acute peripheral vasodilation and subsequent decrease in preload can increase the risk for “suction” events with inflow cannula obstruction [3,33].
Multidisciplinary care
When possible, surgical procedures should be performed in an LVAD-specialized center with a cardiac anesthesiologist or with access to an LVAD specialist, especially for major procedures or for patients with significant comorbidities [16,20]. However, as the number of patients with an LVAD increases, the proportion of care that must be provided by non-cardiac anesthesiologists also increases. [3]. Moreover, for several patient outcome indicators, no significant differences according to anesthesia provider type have been reported, at least for low-risk procedures [35]. However, up to 72% of patients with an LVAD may require some intraoperative cardiovascular pharmacological support; thus, anesthesiologists caring for these patients must be familiar with the administration of vasopressors and inotropic medications [3].
Patient transfer and management of the VAD power source
When the patient is ready to be transferred after the LVAD’s main power is transitioned to battery power, the console is moved together, accompanied by a VAD specialist nurse to maintain intraoperative VAD monitoring. During both patient transfer and surgery, care must be taken to avoid dropping the system controller or monitor or pulling the driveline, because this may induce unexpected interruption of the pump or soft tissue injury, leading to a driveline tunnel infection [36]. Because the driveline carries power to the pump and communicates information with the system controller, any damage to or mishandling of the driveline (e.g., bending, twisting, or allowing to get wet) should be prevented.
Intraoperative monitoring
Both reduced native cardiac contractility and LVAD-induced unloading of the left ventricle result in low pulse pressure in patients with an LVAD. If a palpable pulse is present, an automated cuff system can provide reliable measurements. However, a pulse pressure < 15 mmHg is not palpable and will not be detected by an automated blood pressure cuff. Thus, patients with an LVAD may not have a pulse, especially during anesthesia, making pulse oximetry and noninvasive blood pressure monitoring difficult. The mean arterial pressure (MAP) should therefore be measured and reported in these patients [37], and intra arterial MAP monitoring is advisable for surgeries requiring general anesthesia [21]. The ultrasound-guided technique can facilitate arterial catheter placement in patients with diminished palpable pulses [38]. The HeartMate 3 generates an artificial pulse every 2 s by an algorithm that produces periodic variations in the impeller speed (Fig. 2B). Pulsatility reduces blood stasis and the potential for thrombus formation. Tissue oxygenation can be monitored using arterial blood gasses, and cerebral oximetry can be used to ensure brain oxygenation. A central venous catheter may be indicated for central venous pressure (CVP) monitoring and vasoactive drug administration during major surgical procedures or in patients that are unstable [21,38]. When TEE is used, the position of the interventricular septum can be monitored to provide information on volume status and the proper speed of the LVAD.
Intraoperative hemodynamic management
The LVAD is preload-dependent and afterload-sensitive. Adequate filling of the left ventricle is essential for the optimal function of an LVAD, and afterload sensitivity indicates that hypertension can decrease pump flow.
Afterload to the LVAD
Maintaining an adequate depth of anesthesia and analgesia is important to avoid excessive sympathetic stimulation during laryngoscopy for tracheal intubation and surgical procedures. Light anesthesia may acutely increase the systemic vascular tone (afterload) and decrease the forward pump flow, which can be associated with myocardial or cerebral ischemia, ventricular arrhythmia, and end-organ injury [39,40]. The recommended range of the MAP for patients with an LVAD is 70–85 mmHg [21,31]. High blood pressure can be controlled by antihypertensive medications, but beta-blockers should be used cautiously in patients with right ventricular dysfunction.
A decrease in afterload due to anesthetic agents, especially during anesthesia induction, can induce intraoperative hypotension. On the lower side, a MAP < 60 mmHg is associated with hypoperfusion and therefore must be avoided. If necessary, vasopressors should be used judiciously in small bolus doses to avoid excessive right ventricular afterload. Low-dose vasopressin can be used given its minimal effect on the pulmonary vasculature [41].
Preload to the LVAD
Factors critical to preload include intravascular volume status, patient positioning, surgical approach (laparoscopic vs. open), arrhythmias, and right ventricular function or afterload. In the event of decreased venous return, strategies for placing the patient in a slight Trendelenburg position, initiating judicious fluid loading, and adjusting ventilatory settings are advisable until recovery of the pump preload or vascular tone [14]. Possible hemodynamic effects of intraoperative patient positioning should also be considered. Preload can be reduced if the surgical approach requires a position other than the supine position, such as reverse Trendelenburg, beach chair, lateral decubitus with one-lung ventilation, or prone positions. Therefore, positioning changes should be made slowly with calibrated fluid therapy according to the situation, and limiting the duration or degree of the position to minimize venous pooling in the limbs may be considered [42–44]. In addition, high positive end-expiratory pressure applied with a pneumoperitoneum can significantly reduce venous return [45,46]. During laparoscopic procedures, stepwise peritoneal gas insufflation with judicious fluid therapy could be beneficial, and an intra-abdominal pressure > 15 mmHg should be avoided when the reverse Trendelenburg position is incorporated [45]. The overall effect of pneumoperitoneum on venous return can vary depending on the position, and preload may increase as a result of blood shifting from the abdomen to the thorax in the steep Trendelenburg, lithotomy, or lateral positions [47].
Adequate right ventricular function must be maintained, and an increase in the pulmonary vascular resistance (often resulting from hypoxia, hypercarbia, or acidosis) should be avoided [48].
Monitoring and management of PI
PI values should be monitored and significant variation should not be present. If sudden and substantial changes in the PI (i.e., PI events) occur, the causes must be identified. Most PI events are not suction events, and often result from other causes. Under otherwise stable conditions, a significant drop in the PI value in the operating room indicates a sudden change in the intravascular volume status due to surgical bleeding, and adequate fluid therapy or a blood transfusion is required. Other possible causes include arrhythmias, sudden changes in the power or pump speed, and ventricular suction (Fig. 3). Suction events, which can be easily confirmed using TEE imaging, are more common when the left ventricle is relatively underfilled. Immediate management involves momentarily decreasing the LVAD speed while administering intravenous volume therapy.
When excessive unloading of the left ventricle is encountered, momentarily decreasing the LVAD speed may improve left ventricular filling, although this requires close coordination with the VAD specialist [15]. In the HeartMate 3, when the calculated PI (per second) differs by more than 45% from the PI value averaged for 15 s, the system detects a PI event and the pump speed automatically drops to the low-speed limit and slowly ramps back up to the fixed set-point value. This drop in speed is accompanied by a reduction in the pump flow; therefore, it is important to differentiate between clinically important PI events and effectively address the causes.
Common causes of decreased pump flow in the operating room include right ventricular dysfunction and hypovolemia. Since these two conditions require different management strategies, it is important to diagnose right ventricular dysfunction early based on the clinical situation, TEE imaging, and monitoring parameters for high CVP (> 15 mmHg, as an estimate of right ventricular filling pressure) or low pulmonary arterial pressure, if available [11]. Examples of TEE images indicating severe right ventricular dysfunction resulting in LVAD suction events are shown in Supplementary Videos 1A and B. When severe right ventricular dysfunction is observed, a careful combination of therapies is required, including inotropic medication; optimization of right ventricular preload (judicious volume management) and afterload; optimal ventilation strategies to avoid hypoxemia, hypercapnia, or excessive mean airway pressure; and maintaining normal cardiac rhythm with atrioventricular synchrony [49].
Management of intraoperative ventricular arrhythmias
Because ventricular arrhythmias may impair right ventricular function and decrease inflow to the LVAD, patients should be kept in normal sinus rhythm when possible [50]. Causes of arrhythmia include a previous history of arrhythmia, electrolyte abnormality, metabolic imbalance, the effect of inotropic drugs, or mechanical irritation of the ventricular wall from the inflow cannula (e.g., suction events). If a patient is hemodynamically stable, reversible causes should be identified and corrected. Cardioversion is recommended when ventricular tachycardia or atrial fibrillation with rapid ventricular rates compromise the LVAD flow and/or hemodynamic status [21]. Amiodarone infusion is considered acceptable, and beta blockers should be used carefully. With recurrent ventricular arrhythmias that are difficult to treat, the MAP must be maintained at approximately 80 mmHg to ensure coronary perfusion. Slower arrhythmia is well-tolerated and may not always require therapy.
Advanced cardiovascular life support (ACLS) in patients with an LVAD
There are several unique considerations for cardiopulmonary resuscitation in patients with LVADs [10]. Because the assessment of pulse or noninvasive blood pressure is limited by continuous flow physiology, replacing the pulse concept with perfusion is necessary. The two most common causes of pump failure are disconnection of the power and failure of the driveline; therefore, all connections must be assessed and an adequate power source confirmed, along with frequent checks for device parameters/alarms and auscultation for the LVAD hum when these patients are unresponsive perioperatively [10,51]. When the MAP is monitored, the protocol should be the same as any other peri-arrest situation. If blood pressure is not detectable in an intubated patient, the partial pressure of end-tidal carbon dioxide (EtCO2) can be measured. If volume refractory hypotension is present with the MAP < 30 or 40 mmHg and/or EtCO2 < 20 mmHg in an intubated patient, advanced cardiovascular life support (ACLS) should be initiated, as with any other patient, including chest compressions. Although performing external chest compressions on patients with LVADs has been controversial, a recent consensus states that in cardiac arrest, withholding chest compressions may cause more harm than that associated with the potential dislodgment of the inflow cannula [10]. During resuscitation, a backup plan, such as a venoarterial extracorporeal membrane oxygenator, can be prepared. If inevitable, bolus doses of epinephrine or other vasopressors should be used with caution to avoid an extremely high increase in afterload, which can lead to decreased pump flow, a rapid increase in left atrial pressure, and resultant pulmonary edema.
Postoperative management
Care should be taken to minimize hemodynamic changes, such as hypertension and tachycardia, during extubation or the postoperative recovery period for optimal LVAD function. Deactivated CIEDs must be reprogrammed for active therapy. The patient can recover in the standard post-anesthesia care unit after minor procedures; however, it would be safer for the patient to be transferred to an intensive care unit after major surgeries [28]. As anesthetic effects and subsequent hypoventilation have resulted in unexpected adverse outcomes [52], common causes of an increase in right ventricular afterload, such as hypoxia, hypercarbia, and acidosis, should be avoided
Conclusion
To safely and successfully manage patients with an LVAD undergoing non-cardiac surgery, anesthesiologists must know the type of LVAD and understand the preload-dependent and afterload-sensitive physiology of this population. Additionally, collaborative preoperative multidisciplinary discussions, perioperative management aimed at optimizing intravascular volume and right ventricular function, and management of systemic vascular resistance within adequate ranges for optimal LVAD function are essential.