Introduction
Steroids are commonly used in general anesthesia. Because steroids have been shown to prevent nausea and vomiting [1], reduce postoperative sore throat [2], and improve postoperative outcomes, and they are needed for corticosteroid supplementation [3ŌĆō4]. Previous studies have indicated that steroids exert presynaptic facilitator effects on neuromuscular transmission [5ŌĆō7]. This may contribute to resistance to non-depolarizing neuromuscular blocking agents, such as rocuronium, during the induction of general anesthesia [8ŌĆō10]. Therefore, we should validate the inhibitory effects of steroids on neuromuscular blockade. On the other hand, during recovery from general anesthesia, steroids could inhibit the effects of sugammadex, the reversal agent of steroidal non-depolarizing neuromuscular blocking agents. Sugammadex reverses neuromuscular blockade by encapsulating steroidal neuromuscular blocking agents and reducing their free concentration at the neuromuscular junction [11,12]. Because steroids and steroidal neuromuscular blocking agents have similar structures, there is concern that steroids may hinder the action of sugammadex. If there is a displacement interaction of steroids with sugammadex, then caution is required when using steroids in conjunction with sugammadex. Previous in vitro studies [13,14] have shown that dexamethasone inhibits sugammadex reversal of the rocuronium-induced neuromuscular blockade. However, in clinical studies, dexamethasone did not show an inhibitory effect on sugammadex reversal [15ŌĆō17]. One explanation for this discrepancy is a dose difference between in vivo and in vitro studies [18]. Therefore, this interference effect, observed in vitro, requires further study at clinical doses.
Since dexamethasone and hydrocortisone are widely used during surgery, we explored the effects of these two steroids in vitro using a phrenic nerve-hemidiaphragm rat model. To account for steroidal resistance of neuromuscular blockade [10,18], we calculated the effective dose of rocuronium, that commonly used non-depolarizing neuromuscular blocking agent in various doses of these steroids. We also explored whether various clinical doses of steroids could affect the ability of sugammadex to reverse a rocuronium-induced neuromuscular blockade.
Materials and Methods
Basic study design and sample preparation
The study protocol was approved by the ethics committee of the laboratory of animal research, Asan Institute of Life Sciences (Protocol No. 2015-13-197). All animals were housed at a constant temperature of 22Ōäā and maintained under a regular diurnal cycle with food and water supplied ad libitum. This animal study complied with the ARRIVE guidelines [19].
We did not estimate the sample size statistically. Previous studies have conducted experiments with about 10 animals per group to achieve statistically significant results [12]. To allow for attrition, a total of 88 male Sprague-Dawley rats (6ŌĆō7 weeks old, 150ŌĆō250 g) were included in this study and randomly divided into a dexamethasone or hydrocortisone group that were each further subdivided into four subgroups according to the concentration of steroid: dexamethasone (DexamethasoneŌōć, Jeilpharm, Korea) 0, 0.5, 5, and 50 ╬╝g/ml, or hydrocortisone (CotisoluŌōć, Hanall Biopharm, Korea) 0, 1, 10, and 100 ╬╝g/ml. In each experiment, an independent researcher, who did not participate in data collection or analysis, added one of the four concentrations of dexamethasone or hydrocortisone to the preparations in accordance with a computer-generated randomization table. An identification of the preparations performed by only the number of specimens and the group allocation concealed to other researchers, who did participate in data collection.
Rats were anesthetized with 40 mg/kg of zolazepam and tiletamine mixture (Zoletil50Ōōć, Virbac, France) through intraperitoneal injection, and an adequate depth of anesthesia was confirmed by the absence of a withdrawal response to toe clamping. Phrenic nerve-hemidiaphragm tissue specimens were immediately obtained with a 1 cm base width (diaphragm width attached to the thoracic wall). To ensure tissue viability throughout the experiments, tissue specimens were immersed in 75 ml of Krebs buffer solution (118 mM NaCl, 5.0 mM KCl, 2.5 mM CaCl2, 1.0 mM MgSO4, 30 mM NaHCO3, 1.0 mM KH2PO4, and 11.4 mM glucose, pH 7.4), maintained at 35Ōäā and bubbled with 95% O2/5% CO2. For each specimen, the tendinous portion of the diaphragm was attached to a Grass FT03 force transducer (Grass Instruments, USA), and 2 g of resting tension was applied. The phrenic nerve was attached to a bipolar electrode and stimulated using a Grass S88 stimulator (Grass Instruments, USA), at supramaximal constant-voltage impulses of 2 Hz for 2 seconds (train-of-four, TOF) every 20 seconds. The isometric twitch tension was recorded by the transducer, and the acquired waveforms were displayed using a PowerLab 4/26 data acquisition System (AD Instruments, Australia) and stored on an offline personal computer system using LabChart 7 software (AD Instruments, USA).
Study protocol
This experiment consisted of two phases. In the first phase, we analyzed dose-response relationships and calculated the ED5 (effective dose for 5% neuromuscular blockade; the dose of rocuronium required to depress T1 by 5%), ED10, ED25, ED50, ED75, ED90, and ED95 of rocuronium for neuromuscular blockade. After stabilization of the twitch response for more than 30 minutes, we administered a single bolus of steroid to the Krebs solution and incubated for 30 minutes. Subsequently, a muscle relaxant was administered at increasing concentrations. In a pilot study, we determined the dose required for the complete blockade and applied 20% of this dose as a loading dose and 10% of this dose for incremental dosing. The initial dose was 2.7 ╬╝g/ml and the incremental dose was 1.3 ╬╝g/ml of rocuronium (EsmeronŌōć, MSD, The Netherlands). Each subsequent dose was administered when the decrease in twitch height from the previous dose reached a stable plateau and until a complete depression of the first twitch tension of TOF stimulation (T1) was achieved. The percentage of twitch suppression with the muscle relaxant was calculated. The data were converted to logits, and the effective doses of rocuronium for twitch suppression were calculated from the regression line.
In the second phase of the experiment, following complete depression of T1, sugammadex (BridionŌōć, MSD, The Netherlands) was administered at a dose equimolar to rocuronium. Recovery of the TOF ratio and T1 (percentage of T1 compared to T1 checked just before muscle relaxant administration) were evaluated for 30 minutes in 5-minute intervals. The recovery index calculated by the difference between the time to recover to T1 of 25% and the time to recover to 75% of the initial T1 or two times of the difference between the time to recover to 25% and the time to recover to 50% when it did not reach 75% of the initial T1.
Statistical analysis
In phase 1 of the experiment, the primary endpoint was the ED95 of rocuronium and the secondary endpoints were the ED5, ED10, ED25, ED50, ED75, and ED90 of rocuronium. Dose-response relationships are generated through nonlinear regression of neuromuscular blocking agent dose versus logit of percentage of twitch suppression. Differences between the concentrations of each steroid were evaluated statistically using the Kruskal-Wallis test and Mann-Whitney U test with BonferroniŌĆÖs correction for post hoc analysis. The ED95 and ED5, ED10, ED25, ED50, ED75, ED90 of rocuronium and total dose of rocuronium required for complete block are presented as the mean ┬▒ SD for each group.
In phase 2 of the experiment, the primary endpoint was the TOF ratio at 30 minutes after administration of rocuronium-equimolar sugammadex. The phase 2 secondary endpoints were the T1 recovery at 30 minutes after sugammadex was administered, and the recovery index and TOF ratio patterns for 30 minutes after sugammadex was administered. The TOF ratio and T1 recovery at 30 minutes after administration of sugammadex and recovery index were estimated and expressed as the median and inter-quartile range for each group. The values were compared using the Kruskal-Wallis test followed by Mann-Whitney U test with BonferroniŌĆÖs correction for post hoc analysis. The TOF ratios, recorded every 5 minutes for 30 minutes, were analyzed using generalized estimating equations and graphs were plotted. For validation of the TOF ratio data, all TOF ratio and T1 recovery ratio regardless of group allocation are plotted against time. Statistical analyses were performed using SPSS 18.0 software (SPSS Inc., USA). Statistical significance was accepted for P values < 0.05; all statistical tests were two-sided.
Results
We obtained 81 phrenic nerve-hemidiaphragm tissue specimens from 88 male Sprague-Dawley rats; we excluded seven specimens because we were unable to preserve the phrenic nerves.
During the first phase of the experiment, no significant effects of dexamethasone or hydrocortisone were observed on the ED95 or ED5, ED10, ED25, ED50, ED75, ED90 of rocuronium, regardless of the concentration of dexamethasone or hydrocortisone (Table 1).
In the second phase, the TOF ratio at 30 minutes following sugammadex administration differed significantly only between 0 and 50 ╬╝g/ml of dexamethasone (P < 0.001, Table 2). There were no differences in 0.5 or 5 ╬╝g/ml of dexamethasone compared to 0 ╬╝g/ml. No differences were observed in T1 recovery at 30 minutes following sugammadex administration and in the recovery index in the dexamethasone group, regardless of the concentration (Table 2). The TOF ratio at 30 minutes following sugammadex administration did not decrease significantly at hydrocortisone concentrations of 1 and 10 ╬╝g/ml compared to 0 ╬╝g/ml but decreased significantly at only 100 ╬╝g/ml compared to 0 ╬╝g/ml (P = 0.042), 100 ╬╝g/ml compared to 1 ╬╝g/ml (P < 0.001), and 100 ╬╝g/ml compared to 10 ╬╝g/ml (P < 0.001). The T1 recovery at 30 minutes following sugammadex administration did not differ significantly at hydrocortisone concentrations of 1 and 10 ╬╝g/ml compared to 0 ╬╝g/ml but decreased significantly at hydrocortisone concentration of 100 ╬╝g/ml compared to 0 ╬╝g/ml (P < 0.001), compared to 1 ╬╝g/ml (P = 0.036), and compared to 10 ╬╝g/ml (P < 0.001). Recovery index was significantly different only between 100 and 0 ╬╝g/ml of hydrocortisone (P = 0.03) (Table 2).
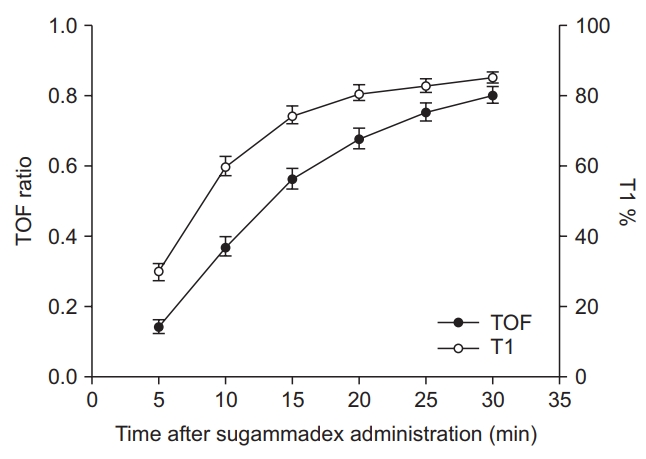
The TOF ratio patterns over 30 minutes after sugammadex was administered are presented in Figs. 1 and 2. There was no significant difference between 0 and 0.5 ╬╝g/ml of dexamethasone. There were statistical significances between 0 and 50 ╬╝g/ ml of dexamethasone (P = 0.015, Table 3), also between 0 and 5 ╬╝g/ml of dexamethasone (P = 0.022, Table 3). Although the graph patterns of 0.5 and 5 ╬╝g/ml of dexamethasone are visually similar (Fig. 1), the standard error is small in 5 ╬╝g/ml of dexamethasone. There was significant difference at only hydrocortisone concentration of 100 ╬╝g/ml compared to 0 ╬╝g/ml (P = 0.018, Table 3). All the TOF and T1 recovery ratios plotted against time are presented in Fig. 3.
Discussion
In this study, acute administration of dexamethasone or hydrocortisone did not alter the effective dose of rocuronium. Therefore, we were unable to clarify the direct effect of these steroids on rocuronium-induced neuromuscular blockade. In phase 2, at the high experimental concentration, steroids had a significant effect on sugammadex reversal of rocuronium-induced neuromuscular blockade. However, these concentrations (50 ╬╝g/ml of dexamethasone or 100 ╬╝g/ml of hydrocortisone) far exceed typical clinical doses. In clinical concentrations of steroids, there was no effect on sugammadex reversal.
We were interested in the effects of steroids on the neuromuscular blockade because steroids facilitate neuromuscular transmission, and therefore may induce resistance to neuromuscular blockade [5ŌĆō10]. The mechanisms of facilitator effect on neuromuscular transmission have been reported stimulating synthesis and release of acetylcholine presynaptically [5ŌĆō9]. Soltesz et al. [10] conducted a clinical study that demonstrated that a single dose of dexamethasone attenuated rocuronium-induced blockade by 15%ŌĆō20% if administered 2ŌĆō3 hours prior to the induction of anesthesia. However, dexamethasone administration during the induction of anesthesia did not influence the time course of the neuromuscular blockade. In our study, dexamethasone and hydrocortisone, administered 30 minutes prior to rocuronium, also did not alter the effective dose of rocuronium. Considering the mechanism and the result of Soltesz et al. [10], it presumes to take some time to induce the facilitator effects of steroid on neuromuscular transmission. Therefore, as demonstrated in this study, acute exposure did not cause resistance to the neuromuscular blockade even at high doses of dexamethasone and hydrocortisone. There is no previously published study about the effects of hydrocortisone on the rocuronium-induced neuromuscular blockade, but the effects of hydrocortisone on pancuronium and succinylcholine were evaluated by Durant et al. [18]. In contrast to previous studies of the effects of steroids, they found no evidence of a facilitator action of hydrocortisone following acute or chronic exposure in cats. Moreover, acute high doses (7 and 15 mg/kg) of hydrocortisone actually enhanced the neuromuscular effects of pancuronium. They indicated that postjunctional receptors remain to be clarified [18]. However, we were unable to demonstrate this effect with rocuronium even with high doses of hydrocortisone. We presume that the effect of steroids on neuromuscular blockade is complex and varies according to the type of neuromuscular blocking agent. In the current study, there was no evidence of facilitator or depressive actions of dexamethasone and hydrocortisone on the effects of rocuronium.
Sugammadex is highly selective for steroidal neuromuscular blocking agents; therefore, there is a low possibility of association with other drugs [20]. Nevertheless, structural similarities between steroids and steroidal neuromuscular blocking agents suggest that interactions are possible [11]. Rezonja et al. [14] explored the influence of dexamethasone on sugammadex reversal of rocuronium-induced neuromuscular blockade in an in vitro model. They found that dexamethasone resulted in dose-dependent inhibition of sugammadex reversal of a rocuronium-induced neuromuscular blockade. To evaluate the effects of dexamethasone, 1 nM, 100 nM, and 10 ╬╝M of dexamethasone (corresponding to normal, elevated, and high clinical concentrations, respectively) were administered; the results revealed a peak effect of dexamethasone on sugammadex at a concentration of 10 ╬╝M (5.16 ╬╝g/ml). However, in the current clinical study, the authors did not observe an inhibitory effect of dexamethasone on sugammadex reversal: 0.15 mg/kg of dexamethasone was administered to anesthetized patients and no delay observed in the reversal of a rocuronium-induced neuromuscular blockade by sugammadex [17]. Buonanno et al. [15] also investigated the clinical relevance of this interaction and found that a prophylactic dose (8 mg) of dexamethasone to prevent postoperative nausea and vomiting did not interfere with reversal of rocuronium-induced neuromuscular blockade by sugammadex. Another clinical study found that 0.5 mg/kg of dexamethasone did not affect the reversal time of sugammadex in children undergoing adenoidectomy and/or tonsillectomy [16]. Rezonja et al. [17] assumed that the plasma dexamethasone concentrations determined in clinical studies were lower than those used for in vitro studies because of low-dose dexamethasone administration and plasma protein binding. Therefore, these results should be confirmed at various concentrations that are closer to clinical concentrations used in anesthetic practice. The therapeutic plasma concentration of dexamethasone used for prophylaxis of postoperative nausea and vomiting [1] or sore throat [2] during general anesthesia is close to 0.5 ╬╝g/ml [21]. In high-dose therapy (0.6ŌĆō1 mg/kg) [22,23] for neoplastic or cardiac surgery, the plasma concentration is approximately 5 ╬╝g/ml [24]. Therefore, we explored the effects of 0 ╬╝g/ml, 0.5 ╬╝g/ml (0.97 ╬╝M), and 5 ╬╝g/ml (9.69 ╬╝M) of dexamethasone. Additionally, we included a very high experimental concentration of 50 ╬╝g/ml to evaluate the range of dexamethasone concentrations that may interfere with sugammadex reversal. Only 50 ╬╝g/ml of dexamethasone caused inhibition. The sugammadex reversal effect was not significantly affected at 0.5 or 5 ╬╝g/ml of dexamethasone, which represents a clinical concentration. This is in agreement with the results of previous clinical studies [15ŌĆō17]. However, our results do not agree with those of previous in vitro studies [13,14]. In the present study, similar doses (5 ╬╝g/ml vs. 5.16 ╬╝g/ml) of dexamethasone did not significantly suppress sugammadex reversal. This difference might be related to different evaluation methods and different interpretations of the results. In previous in vitro studies, the authors counted the contracting units of skeletal muscle and concluded that micromolar concentrations of dexamethasone significantly suppressed the action of sugammadex because the ratio of the number of contracting units of skeletal muscle was lower than the ratio at which a rocuronium-induced neuromuscular blockade would be completely reversed by sugammadex [13,14]. Instead, we used the recovery of TOF ratio, T1, and recovery index to evaluate the recovery property of neuromuscular blockade. Possibly the TOF ratio did not fully reflect whether rocuronium-induced neuromuscular blockade is completely reversed by sugammadex. However, TOF ratio has become acknowledged as a sensitive and useful measure of adequacy of neuromuscular recovery clinically. Previous clinical studies [15ŌĆō17] also used TOF ratio as primary endpoint and reported same results as our study. However, the acceleromyography used in clinical studies may overestimate TOF ratio unacceptably [25]. We used mechanomyographic TOF ratio in this study, and we could exclude overestimation as identified by Fig. 3. Therefore, our results have important implications that could more convince the reliability of previous clinical studies. And importantly, there was no statistical significance in the results of previous in vitro studies [13,14]. Overall, our findings support the results of previous clinical studies [15ŌĆō17]: clinically relevant inhibition of sugammadex reversal on rocuronium-induced neuromuscular blockade is unlikely at typical clinical doses of dexamethasone.
Another supposed cause of the different results is the doses of rocuronium and sugammadex. Previous in vitro studies [13,14] used 10 ╬╝M of rocuronium and sugammadex. In the present study, we used 13.0 ┬▒ 2.04 ╬╝g/ml of rocuronium, 21.2 ┬▒ 3.3 ╬╝M, and equimolar sugammadex in 5 ╬╝g/ml (9.69 ╬╝M) concentrations of dexamethasone group. In a pharmacokinetic study, the peak sugammadex concentration was 197 ╬╝g/ml following a 16 mg/kg sugammadex infusion [26]. The dose of sugammadex in previous clinical studies [15ŌĆō17] was 2 mg/kg or 200 mg, which is roughly around 20 ╬╝M. Considering the encapsulating mechanism and higher dose of sugammadex, the inhibitory effects of dexamethasone may have been masked in our experiment and in previous clinical studies. Additionally, the different results could be explained by the use of different preparations, co-culturing of human skeletal muscle cells with rat spinal cord explants vs. a phrenic nerve-hemidiaphragm rat model.
We also evaluated the effect of hydrocortisone in 1, 10, and 100 ╬╝g/ml. The dose of hydrocortisone used for corticosteroid supplementation is 20ŌĆō100 mg in a usual and up to 200ŌĆō300 mg in a high-dose therapy [4,27]. The plasma concentration is close to 1 ╬╝g/ml in a usual dose and is approximately 10 ╬╝g/ml in a high-dose therapy [28ŌĆō30]. And 100 ╬╝g/ml of hydrocortisone was included as a high experimental concentration. Hydrocortisone demonstrated a similar result as that of dexamethasone. The reversal effect on rocuronium-induced neuromuscular blockade of sugammadex was not significantly affected at clinical concentrations of hydrocortisone. Hydrocortisone has a higher binding affinity for sugammadex than dexamethasone. The binding affinity of dexamethasone for sugammadex was less than 1.00 ├Ś 103 M, whereas the binding affinity of hydrocortisone for sugammadex was 5.48 ├Ś 104 M [20]. Additionally, significantly more molecules may be present in hydrocortisone groups than dexamethasone groups: 10 ╬╝g/ml hydrocortisone is 27.6 ╬╝M. Therefore, hydrocortisone could be assumed to have more strong effect on sugammadex. However, there were no inhibitory effects on sugammadex reversal in clinical concentrations of hydrocortisone as dexamethasone. And this is the first study to evaluate the effect of hydrocortisone on sugammadex reversal.
This study has several limitations. First, this experimental model does not have the same pharmacokinetic and pharmacodynamic characteristics as in vivo clinical conditions. The concentrations of dexamethasone in this study do not represent the exact concentrations of dexamethasone in plasma or at the neuromuscular junction in humans; however, the concentrations of free dexamethasone in this study are expected to be higher than in vivo in the absence of protein binding. Nevertheless, this study yielded results comparable to those of clinical studies, supporting the conclusion that clinical doses of dexamethasone used in anesthesia practice do not inhibit the reversal of sugammadex [15ŌĆō17]. Second, we observed recovery of neuromuscular blockade for 30 minutes and analyzed the data at 30 minutes after sugammadex administration instead of waiting for a full recovery. In many specimens, the TOF ratio at 30 minutes after sugammadex administration did not reach a sufficient recovery value (TOF ratio > 0.9). It seems that 30 minutes were not enough for a full recovery. We conducted this experiment just for 30 minutes because, in our pilot study, 30 minutes were sufficient to evaluate recovery, and we thought that an analysis of the data at the same time point is important to detect inhibition of recovery. Additionally, statistical analysis can be used to compensate for any differences. Finally, we should have strictly limited the number of animals involved; therefore, there were limited size of samples and substantially large standard deviations.
In conclusion, no concentration of dexamethasone or hydrocortisone altered the effective dose of rocuronium, indicating that they provided no resistance to the rocuronium neuromuscular blockade. Although inhibitory at high (not clinical) concentrations, clinical concentrations of steroids had no inhibitory effect on sugammadex to reverse rocuronium-induced neuromuscular blockade. Therefore, we can expect proper effects of rocuronium and sugammadex on neuromuscular blockade when the steroids, dexamethasone, or hydrocortisone are used during general anesthesia.