Introduction
Management of bleeding is a primary concern during the perioperative period. Total knee arthroplasty (TKA) is accompanied by significant blood loss that often requires blood transfusions [1,2]. In particular, bilateral TKA results in increased blood loss [3,4]. During TKA, a tourniquet is used to reduce unnecessary bleeding and secure a clear operative field. Therefore, most bleeding occurs after tourniquet release rather than during the operation.
Hypotensive epidural anesthesia has been suggested as a technique for reducing perioperative blood loss and the need for blood transfusion in TKA and total hip arthroplasty [5,6]. Another study revealed that high blood pressure due to postoperative pain may influence postoperative blood loss in TKA [7]. In addition, there was a significance correlation between postoperative blood loss and morphine consumption [7]. Considering that pain scores and opioid consumption are higher in patients after bilateral TKA than unilateral TKA [8], the effect of postoperative pain on postoperative blood loss may be clearer in bilateral TKA. To date, no comprehensive data is available on the relationship between postoperative pain and blood loss in patients with patient-controlled epidural analgesia after sequential bilateral TKA.
The aim of this study was to investigate the relationship between early postoperative pain intensity and postoperative blood loss in patients after bilateral TKA.
Materials and Methods
This study was approved by the Hospital Ethics Committee and written informed consent was obtained from all patients before surgery. From February 2007 to November 2007, a prospective study was conducted on 91 patients who underwent elective sequential bilateral TKA for osteoarthritis. Patients were excluded from the study if any of the following criteria were present: current infectious disease, history of neurological disease, preoperative hemoglobin < 10 g/dl, coagulopathy, American Society of Anesthesiologists (ASA) class IV, past or current alcohol or narcotic abuse, and hypersensitivity to opioid or local anesthetics.
None of the patients were pre-medicated. Lactated Ringer's solution was injected intravenously via a 20-gauge IV catheter and an external jugular vein was accessed for blood transfusion with an 18-gauge IV catheter. Patients received approximately 300 ml of lactated Ringer's solution before spinal anesthesia. All patients received combined spinal-epidural (CSE) anesthesia administered by anesthesiologists familiar with the technique in regional anesthesia. CSE was performed with a CSE kit (Espocan┬«, B. Braun, Melsungen, Germany) at L2-3 or L3-4 with the patient in the left lateral decubitus position. After local infiltration with 2 ml of 1% lidocaine, an 18-gauge epidural needle was placed first in the epidural space using the loss of resistance technique with air. A 27-gauge spinal needle was then introduced through the epidural needle into the subarachnoid space, and free flow of cerebrospinal fluid (CSF) was observed. The spinal anesthetic solution was prepared as follows: 1 ml of 1% tetracaine was taken from a vial of powdered tetracaine (Pantocainsterile inj.┬«, Daihan Pharm., Seoul, Korea) dissolved in 2 ml of 0.9% NaCl. This was mixed with 1 ml of the patient's CSF and 0.1 ml of 0.1% epinephrine to make 2 ml of 0.5% isobaric tetracaine. Then, 2 ml of 0.5% isobaric tetracaine was injected at a rate of 0.1 ml/sec with upward orientation of the spinal needle bevel. The epidural catheter was inserted 4 cm upward from the spinal puncture level. If systolic arterial pressure decreased below 90 mmHg or to a level less than 75% from the baseline value, 4-8 mg of IV ephedrine was administered. The patients were kept in a neutral supine position until the sensory block peaked. Surgery was initiated when the level of sensory block was at the T10 dermatome, which was confirmed by a pin-prick test with a 22 G hypodermic needle on each side of the midthoracic line. The epidural infusion pump used 225 mg of 0.225% ropivacaine, 1.5 ┬Ąg/kg of sufentanil, 0.6 mg of naloxone, and 0.9% normal saline in a 100 ml solution. The patient-controlled analgesia device (Accufuser Plus┬«, P2015M, Woo Young Medical, Seoul, Korea) was designed to deliver a dose of 2 ml/hour, with an "on-demand" bolus of 0.5 ml every 15 minutes, and was withdrawn at 48 hours. The same surgeon performed all surgical procedures to maintain a uniform application of the surgical stimulus. The sequential arthroplasty was performed by one team under a single episode of anesthesia. A midline incision and parapatellar arthrotomy was made using standard surgical techniques. Following instrumented bone resection, the total knee components were fixed. The tourniquet and drain clamp were released after the skin wound was sutured. A SureTrans┬« autotransfusion system (Davol Inc, Cranston, RI, USA) was inserted near the medial aspect of the joint space and stayed in place for 24 hours after the surgery. Thromboembolic prophylaxis was ensured by enoxaparin 40 mg administered subcutaneously once a day beginning on postoperative day 1.
Preoperative data including age, sex, height, weight, hemoglobin level, and the presence of pre-existing medical conditions such as diabetes mellitus and hypertension, were recorded. Mean arterial pressures were checked preoperatively, intraoperatively, and at 6, 12, and 24 hours postoperatively. To exclude the effect of residual spinal anesthesia, pain was evaluated at 6, 12, and 24 hours postoperatively using an 11-point verbal numerical rating scale (VNRS). Patients were instructed preoperatively to express their pain on the 0-10 VNRS, where a score of 0 represents no pain at all and a score of 10 represents the worst pain imaginable. The amount of intraoperative blood loss was obtained by weighing sponges and measuring blood recovered in suction canisters. Postoperative blood loss was obtained by measuring the volume of blood drained in SureTrans® at 6, 12, and 24 hours postoperatively. Since approximately 70% of the total drained blood is usually collected within 6 hours postoperatively [9], we divided the groups according to the VNRS at 6 hours postoperatively to determine the effect of postoperative pain on postoperative blood loss. The patients were divided into three groups, which were mild pain (n = 34, VNRS score 0-4), moderate pain (n = 24, VNRS score 5-6), and severe pain (n = 33, VNRS score 7-10) [10].
Statistical analysis was performed using SPSS 13.0 (SPSS Inc., Chicago, IL, USA) or SAS software 9.2 (SAS Inc., Cary, NC, USA). The normality of distribution was assessed with a q-q plot and the Shapiro-Wilk test. All data were expressed as mean ┬▒ SD, median (interquartile range), or the number of patients according to the distribution of normality. Data was compared among the groups using one-way ANOVA, the Kruskal-Wallis test or chi-square test. If the Kruskal-Wallis test proved significant, a Mann-Whitney U test with Bonferroni correction was used to evaluate differences among the groups. Factors influencing postoperative blood loss were analyzed using linear mixed models. A P value of less than 0.05 was considered statistically significant.
Results
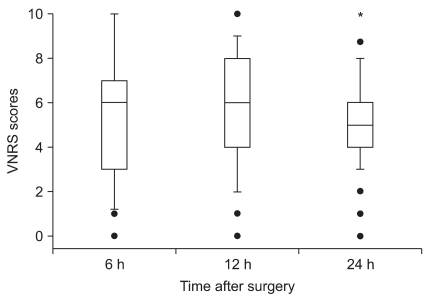
CSE anesthesia was successfully accomplished in all patients. Patient characteristics were similar among the three groups (Table 1). VNRS scores for pain of all patients during the postoperative period are shown in Fig. 1. The median VNRS score was lower at 24 hours than at 12 hours postoperatively (5 [IQR 4-6] versus 6 [IQR 4-8], respectively; Bonferroni-corrected P = 0.003).
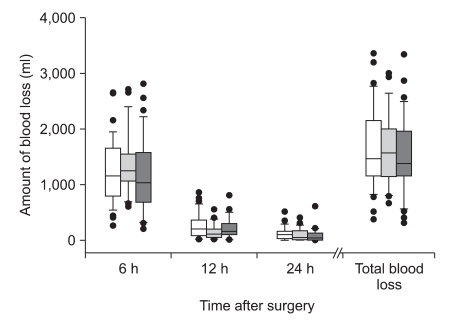
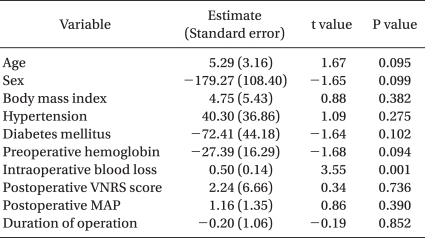
Mean arterial pressures at 6, 12, and 24 hours postoperatively were not different among the three groups (Table 2). Amount of blood loss at 6, 12, and 24 hours postoperatively and total blood loss also did not significantly differ among the three groups (Fig. 2). The number of units of packed red blood cells transfused was the same for all three groups [median 0 unit (range 0-2)]. After linear mixed model analysis, the amount of intraoperative blood loss was a statistically significant factor for the amount of postoperative blood loss (P = 0.001) (Table 3).
Discussion
TKA is a procedure that is being performed at an increasing rate as the result of an increasing mean age of the population. Although the majority of patients with arthritis of the knee undergo unilateral TKA, patients often present with symptomatic arthritis of both knees. Even though concomitant bilateral TKA is associated with a higher rate of complications [3,11,12], there are many advantages to performing sequential bilateral arthroplasty under one episode of anesthesia. In particular, the preference of patients for a concomitant bilateral TKA and their satisfaction following the procedure are high due to a shorter hospitalization time, a faster return to function in their daily lives, and a reduction of medical costs compared with staged TKA [4,13,14].
This study shows that postoperative pain intensity does not affect postoperative blood loss after bilateral TKA. This result differs from that of a previous study which demonstrated that elevated postoperative pain significantly correlated with increased postoperative blood loss after TKA, and the mean arterial pressure at 6 hours after surgery was also a factor influencing the number of transfused units of blood [7]. However, in our study, postoperative VNRS scores and mean arterial pressures were not a factor for postoperative blood loss (Table 3). Even though the amounts of blood lost during the operation were not high (median 200 ml [IQR 150-300]) due to the use of a tourniquet, only the amount of intraoperative blood loss was a factor influencing postoperative blood loss. Therefore, in contrast to the previous study [7], postoperative pain intensity did not act as a factor on postoperative blood loss. The possible reason for different results between this study and the previous study [7] may be due to differences in the type of surgery (unilateral versus bilateral) and the methods of postoperative analgesia (intravenous (IV) patient-controlled analgesia (PCA) versus IV PCA + continuous femoral nerve block versus IV PCA + continuous posterior lumbar plexus block versus epidural PCA). Therefore, according to the study design, the main factor for postoperative blood loss could be changed. In this study, instead of postoperative pain and mean arterial pressure, intraoperative surgical factors may be more important for postoperative blood loss. There are many factors influencing intraoperative blood loss, such as patient factors, surgeon factors, method of thromboprophylaxis, and the timing of tourniquet release [15-17]. We did not analyze the factors contributing to intraoperative blood loss, and this could be a limitation of this study. Considering that intraoperative blood loss is an important factor effecting postoperative blood loss, the use of antifibrinolytic or hemostatic agents proven to be effective in reducing postoperative blood loss [18-20] may be useful in case of heavy bleeding during the surgery.
Deliberate hypotension is a technique for reducing perioperative blood loss by significantly lowering arterial pressure, and has been studied extensively in major orthopedic procedures [21,22]. Hypotensive epidural anesthesia with a mean arterial pressure of 45 to 50 mmHg has been shown to significantly reduce blood loss and the need for blood transfusion in TKA [6]. In the current study, intraoperative mean arterial pressure was maintained at about 90 mmHg in the three groups. Therefore, the amount of intraoperative blood loss was similar among the three groups. In addition, despite the differences in pain intensity, postoperative mean arterial pressures were not different among the groups. If there was a difference in the mean arterial pressure postoperatively, there would likely be a difference in the amount of blood loss.
In this study, the average total blood loss was approximately 1,500 ml during the first 24 hours after the operation. It has been reported that most blood loss occurs in the first few hours, with 50% occurring within the first 3 hours and 70% within the first 6 hours [6,9]. In accordance with previous results, about 79% of the total blood drainage was collected within 6 hours postoperatively and there were no differences among the groups.
In addition to management of postoperative blood loss, postoperative pain is a major concern after TKA. After knee surgery, pain intensity is reportedly quite high [7,23-25]. Despite the use of epidural analgesia, the median VNRS score was 6 (IQR 3-7) at 6 hours, 6 (IQR 4-8) at 12 hours, and 5 (IQR 4-6) at 24 hours after surgery in our study. Therefore, in addition to continuous epidural analgesia, multimodal approaches to pain control, such as peripheral nerve block and/or additional analgesics, may be needed in the early postoperative period [7,23,25].
In conclusion, the intensity of early postoperative pain is not a component for postoperative blood loss in sequential bilateral TKA. The amount of intraoperative blood loss correlates with the amount of postoperative blood loss.