Hemidiaphragmatic paralysis after costoclavicular approach versus other brachial plexus blocks in upper limb surgery: a meta-analysis
Article information

Abstract
Background
The costoclavicular brachial plexus block (CCB) is a recently established technique that uses the infraclavicular approach and is performed just below the clavicle. This meta-analysis aimed to determine whether CCB can reduce the incidence of hemidiaphragmatic paralysis (HDP), which is a major adverse event related to brachial plexus block (BPB), while yielding comparable block performance as other BPB techniques.
Methods
We searched electronic databases to identify relevant studies that compared the incidence of HDP between CCB and other BPB techniques. The primary outcome was the incidence of HDP following CCB and other BPB techniques. The secondary outcomes were pulmonary function test results, other adverse events, and block performance parameters such as onset and performance time.
Results
We included six randomized controlled trials that included 414 patients. Compared with the other BPB group, the CCB group had a significantly lower incidence of HDP (relative ratio: 0.21, 95% CI [0.12, 0.36], P < 0.001) and higher peak expiratory flow rate (mean difference: 0.68 L/s, 95% CI [0.13, 1.23], P = 0.015). There were no significant between-group differences with respect to other adverse events and block performance parameters.
Conclusions
Compared with other BPB techniques, CCB involves a lower incidence of HDP with comparable onset and performance time.
Introduction
Ultrasound (US)-guided brachial plexus block (BPB) targets the brachial plexus at various levels to provide anesthesia and analgesia for upper limb surgery. This usually involves lateral sagittal infraclavicular BPB (Fig. 1) that targets the brachial plexus at the cord level and deposits local anesthetics around the second segment of the axillary artery in the lateral infraclavicular fossa [1]. Costoclavicular BPB (CCB) is a recently introduced technique for infraclavicular blocks (Fig. 2). Three brachial plexus cords are located within the costoclavicular space laterally to the axillary vessels and are tightly clustered; moreover, there is a consistent relationship among the cords [2,3]. During CCB administration, the brachial plexus is targeted immediately caudally to the clavicle in the costoclavicular space, which is located more superficially than the space targeted in other BPB techniques [4,5]. Recently, Karmakar et al. [4] described a costoclavicular approach that used a single injection and a relatively small anesthetic volume that allowed rapid onset and reliable analgesia. Accordingly, CCB has emerged as an attractive alternative approach given the aforementioned anatomical advantages and reliable blockade.

Probe position and US view of lateral sagittal approach. The US probe is placed medially to the coracoid process in the sagittal plane in the infraclavicular area, and three cords are targeted using the in-plane technique. AA: axillary artery, LC: lateral cord, MC: medial cord, PC: posterior cord, US: ultrasound.
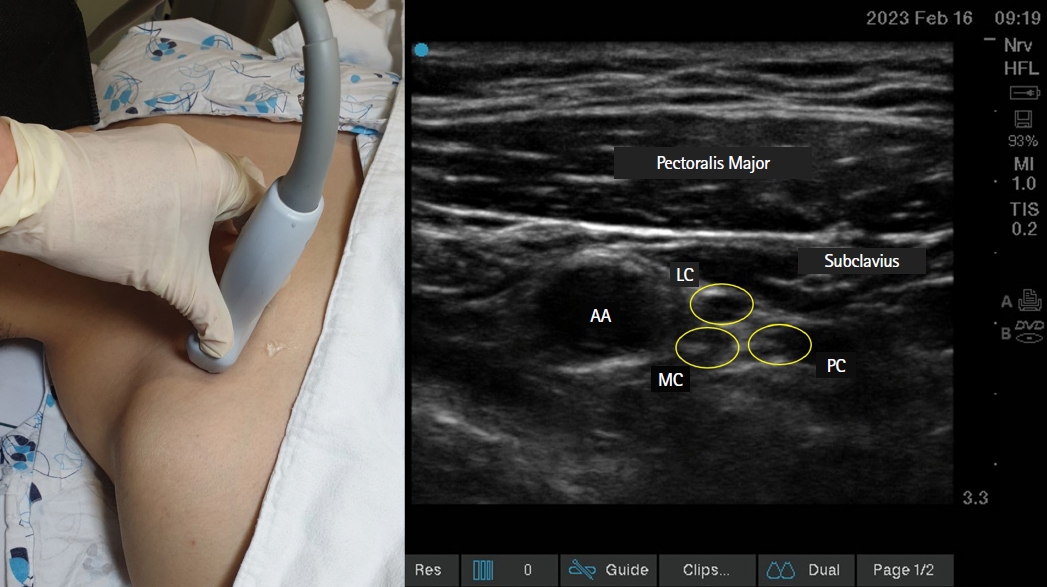
Probe position and US view of the costoclavicular approach. The US probe is placed parallel to the clavicle in the midclavicular area and tilted toward the cephalad; and three cords are targeted using the in-plane technique. AA: axillary artery, LC: lateral cord, MC: medial cord, PC: posterior cord, US: ultrasound.
In addition to the rapid onset of reliable sensory-motor blockade of the major terminal nerves of the brachial plexus, CCB is related to a lower incidence of hemidiaphragmatic paralysis (HDP) compared with other BPB techniques [6–8]. HDP, which is a common complication following BPB, is caused by the inadvertent spread of the local anesthetic to the phrenic nerve [9]. The occurrence of HDP is related to the applied BPB technique, injected local anesthetic volume, and distance between the block site and the C3–C5 nerve root or phrenic nerve [10]. The incidence of HDP is highest for interscalene (up to 100%) and supraclavicular BPB (up to 70%), followed by lateral sagittal infraclavicular BPB (up to 24%). Although HDP is well tolerated by healthy patients, it may cause substantial morbidity in patients with marginal pulmonary function [11–13]. Among the four BPB approaches, axillary BPB has a low possibility for phrenic nerve block [14]; however, it may require an additional approach for musculocutaneous block [15]. Contrastingly, CCB can yield a high-quality anesthesia and analgesia without additional needle re-insertion that reduces the performance time [15].
We hypothesized that CCB involves a lower incidence of HDP compared with other BPB techniques. Accordingly, we aimed to compare the incidence of HDP and other adverse events, pulmonary function test results, and block performance between CCB and other BPB techniques among patients undergoing upper limb surgery.
Materials and Methods
We conducted a systematic review and meta-analysis following the Preferred Items for Systematic Reviews and Meta-analysis statement guidelines [16]. The study protocol was registered in the International Prospective Register of Systematic Reviews on October 6, 2022 (CRD42022364910).
Literature search
We searched PubMed, EMBASE, Cochrane Central Register of Controlled Trials, Cumulated Index to Nursing and Allied Health Literature, Scopus, and Web of Sciences for studies that compared the incidence of HDP between CCB and other BPB techniques. The search terms included ‘costoclavicular’ and ‘brachial plexus block’. Supplementary Table 1 shows the search strategies and results for each database. The database query was performed on September 29, 2022, without restrictions in terms of language, year, journal, or region.
Study selection
We selected studies based on the following PICOS (population, intervention, comparison, outcomes, and study design) criteria: (P) patients who underwent upper limb surgery under BPB, (I) CCB, (C) other BPB techniques, (O) occurrence of HDP, (S) human studies including randomized controlled trials (RCTs) or retrospective cohort studies. We excluded case reports, conference abstracts, non-peer-reviewed studies, and studies without data regarding HDP. The titles and abstracts of identified articles were screened by two independent authors (C.-H.K. and H.-J.S.). Subsequently, the authors screened the full texts of eligible articles and selected studies that met the inclusion criteria. Disagreements were resolved through discussions with a third author (J.-H.R.).
Data extraction
The two authors (C.-H.K. and H.-J.S.) independently extracted the following data from the included studies: the first author, published year, study design, sample size, BPB type, assessment tool for HDP, and characteristics of the local anesthetics (drug concentration, type, and volume). Values reported as median and range (for example, interquartile range or minimum to maximum) were converted to the mean and standard deviation following Luo’s and Wan’s formula [17,18]. The primary outcome was the incidence of HDP. The secondary outcomes were postoperative pulmonary function test results, other adverse events (Horner’s syndrome, hoarseness, paresthesia, vascular puncture, dyspnea, desaturation, and pneumothorax), onset time, performance time, and needle passage time. Disagreements were settled through discussions with the third author (J.-H.R.).
Quality assessment
Two authors (C.-H.K. and H.-J.S.) independently evaluated the risk of bias (RoB) and level of evidence. The recent version of the Cochrane RoB tool (RoB 2) that evaluates randomization bias, bias due to deviation from the intended intervention, missing outcomes bias, measurement bias, and selective reporting bias was used for RCTs [19], with RoB being graded as low, moderate, or high risk. For non-randomized studies, the quality was assessed using the Newcastle-Ottawa scale (NOS) that comprises three domains: selection, comparability, and outcome [20]. The level of evidence was scored based on the RoB, inconsistency, indirectness, imprecision, and publication bias in accordance with the Grading of Recommendations, Assessment, Development, and Evaluation [21].
Statistical analysis
Statistical analyses were performed using the ‘meta’ and ‘metafor’ packages of R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria) [22–24]. The pooled effect size was estimated by calculating the risk ratio (RR) or mean difference (MD) based on data obtained from RCTs. Among-study heterogeneity was presented as the inconsistency index (I2), with an I2 value > 50% indicating significant heterogeneity. Based on the heterogeneity, we used the fixed-effect model (I2 < 50%) or random-effect model (I2 > 50%). In case of a small number of included studies (e.g., < 10), the Hartung-Knapp-Sidik-Jonkman method was used in the random-effect analysis to minimize the error rate [25]. In sensitivity analysis, each study was omitted one by one, followed by re-estimation of the effect size. Publication bias was evaluated using the symmetrical funnel plot and Egger’s linear regression test. We planned to perform subgroup analysis according to the other BPBs (supraclavicular, infraclavicular, interscalene, or axillary) control group. Statistical significance was set at P < 0.05.
Results
Study selection
Among 300 initially identified articles, 174 duplicate articles were excluded. Subsequently, the titles of the remaining 126 articles were screened and 56 articles were selected. After abstract screening, 19 papers were selected. Finally, full-text screening of the 19 papers yielded six RCTs that included 414 patients [6–8,26–28] and one retrospective study that included 236 patients [29] (Fig. 3). Among the 414 patients in the RCTs, 203 and 211 patients underwent CCB and other BPB techniques, respectively. The other BPB techniques included supraclavicular block (n = 3) [6,7,29], interscalene block (n = 1) [27], lateral sagittal block (n = 1) [26], superior trunk block (n = 1) [28], and paracoracoid block (n = 1) [8]. Table 1 shows detailed information regarding the seven included studies.
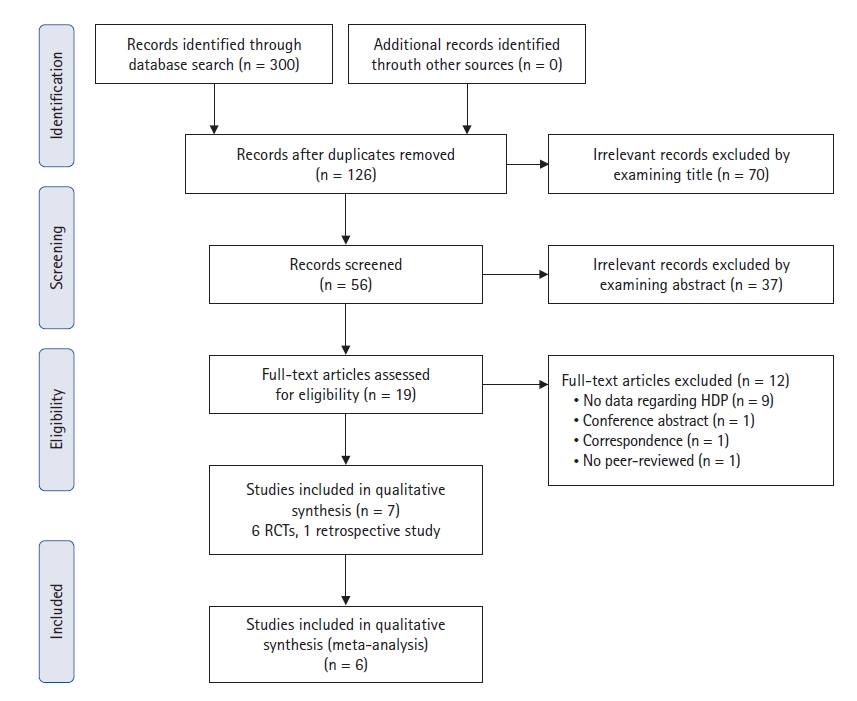
PRISMA flow of the literature search and study selection. A total of 300 articles were identified through electronic databases. Among them, 174 duplicate articles were removed. After screening the titles of the 126 remaining articles, 56 articles were considered relevant. Subsequent screening of the abstracts of the 56 articles yielded 19 relevant studies. Finally, full-text screening of these 19 studies yielded six RCTs and one retrospective study. RCT: randomized controlled trial.
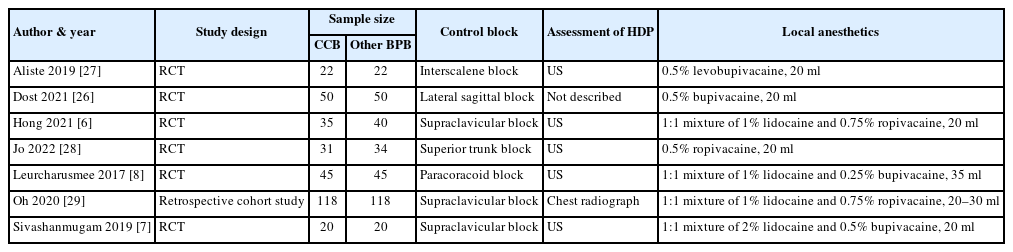
Baseline Characteristics of the Included Trials
Incidence of HDP
The incidence of HDP was significantly lower in the CCB group than in the other BPB group (5.9% vs. 31.3%, six studies; RR: 0.21, 95% CI [0.12, 0.36], P < 0.001, I2 = 47%; fixed-effect model) (Fig. 4) [6–8,26–28]. The re-estimated RR in the sensitivity analysis retained statistical significance (Supplementary Fig. 1) that indicated that no study skewed the pooled effect size. A funnel plot demonstrated symmetrical distribution (Supplementary Fig. 2); additionally, Egger’s linear regression test did not reveal significant publication bias (P = 0.628). In the subgroup analysis, the results differed according to the model applied (fixed-effect vs. random-effect model) (Supplementary Fig. 3). Given the heterogeneity, we used the fixed-effect model effect size for the supraclavicular subgroup (I2 = 0%) and the random-effect model effect size for the interscalene subgroup (I2 = 73%). Accordingly, the protective effect of CCB was only significant when compared with the supraclavicular approach (two studies; RR: 0.20, 95% CI [0.08, 0.47], P < 0.001, I2 = 0%; fixed-effect model) (Supplementary Fig. 3) [6,7].
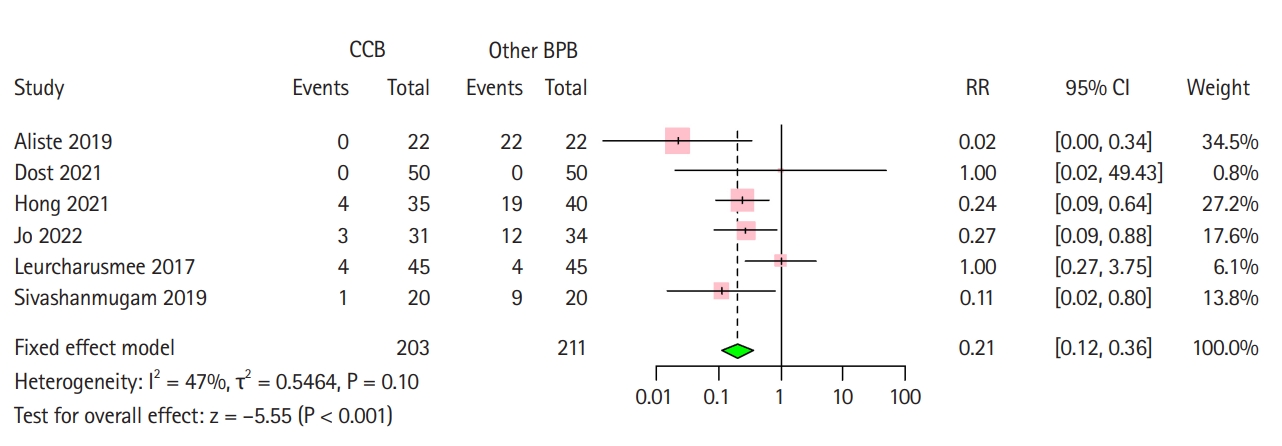
Forest plot for the incidence of HDP between the CCB and other BPB groups. CCB: costoclavicular brachial plexus block, BPB: brachial plexus block, RR: risk ratio, HDP: hemidiaphragmatic paralysis.
Secondary outcomes
Table 2 summarizes the pooled effect sizes for the secondary outcomes. Patients in three studies underwent postoperative pulmonary function tests [6,7,28], with all three studies reporting the peak expiratory flow rate (PEFR). The CCB group showed significantly higher PEFR values than the other BPB group (MD: 0.68 L/s, 95% CI [0.13, 1.23], P = 0.015, I2: 0%; fixed-effect model) (Supplementary Fig. 4) [6,7,28]. There were no significant between-group differences in the incidence of other complications (3.0% vs. 5.2%, six studies; RR: 0.62, 95% CI [0.27, 1.43], P = 0.263, I2 = 0%; fixed-effect model) (Supplementary Fig. 5) [6–8,26–28]. Additionally, there were no significant between-group differences in the onset time (three studies; MD: 1.92 min, 95% CI [–9.50, 13.33], P = 0.545, I2 = 90%; random-effect model) (Supplementary Fig. 6) [8,26,27], performance time (three studies; MD: 0 min, 95% CI [–2.40, 2.40], P = 0.999, I2 = 90%; random-effect model) (Supplementary Fig. 7) [8,26,27], and needle passage time (three studies; MD: −0.28 min, 95% CI [–3.09, 2.54], P = 0.714, I2 = 98%; random-effect model) (Supplementary Fig. 8) [8,26,27].
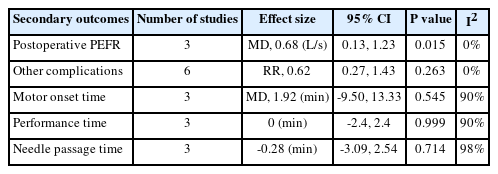
Summary of the Secondary Outcomes
Quality assessment
Supplementary Fig. 9 shows the quality assessment of the included studies. Among the included RCTs, one and five studies showed moderate and low RoB, respectively. The moderate RoB resulted from unbalanced participant loss between the groups (four and one in the CCB and other BPB groups, respectively) due to unexpected open conversion. The researcher who administered the BPB could not be blinded; however, all the included studies used a blinded observer to objectively assess the outcomes. This suggested that the block performer’s awareness of the group allocation did not influence the evaluation of outcomes. The NOS score for the cohort study was 8 out of 9 that indicated good quality. There was a moderate evidence level regarding the incidence of HDP, other complications, and postoperative PEFR. Contrastingly, there was a low evidence level regarding the onset time, performance time, and needle passage time that involved a risk of inconsistency and imprecision (Supplementary Table 2).
Discussion
We observed that CCB involved a lower incidence of HDP than other BPB techniques (lateral sagittal, supraclavicular, superior trunk, and interscalene blocks). Compared with the other BPB group, the CCB group showed more preserved PEFR that is an indicator of the physiologic impact of diaphragmatic weakness [30]. There was no between-group difference in the incidence of block-related complications as well as the onset and performance time.
BPB is a valuable regional anesthesia technique for patients undergoing upper extremity surgery. HDP is a common complication of BPB, with its incidence following interscalene BPB reaching 100% [31]. In our study, the incidence of HDP was 5.9% and 31.3% in the CCB and other BPB groups, respectively. Moreover, the included retrospective study, which was excluded from the meta-analysis, showed that CCB has a greater protective effect against HDP than supraclavicular BPB (2.5% vs. 35.8%) [29], which is consistent with our meta-analysis findings. As aforementioned, the distance between the phrenic nerve or C3‒C5 roots and the block site significantly influences the occurrence of HDP [6]. This could explain the lower incidence of HDP and better PEFR in the costoclavicular approach that involves a relatively distal area from the phrenic nerve or C3‒C5 roots compared with the interscalene, superior trunk, and supraclavicular approaches. In subgroup analysis, CCB was superior only to the supraclavicular approach. Notably, there was no significant difference between the CCB and interscalene approach that could be attributed to the small sample size of the subgroup of the interscalene approach. Regarding safety, the costoclavicular approach might be a valuable alternative for patients with impaired lung function.
The incidence rates of block-related complications were 3.0% and 5.2% in the CCB and other BPB groups, respectively. All included RCTs applied US-guided BPB techniques that may have contributed to the low incidence of complications across the BPB techniques. This further demonstrates the safety benefits of the costoclavicular approach.
There were no between-group differences in the onset and performance time; however, this result should be carefully interpreted given the small number of included RCTs and the heterogeneity within the control group (one interscalene and two lateral sagittal approaches). Moreover, it is crucial to consider the familiarity of the operator with the nerve block method [32]. Although nerve blocks were performed by experienced and skillful physicians, we could not adjust for biases resulting from differences in the technique level across operators. Another important factor that influences the technical aspect is the nerve depth. The three brachial plexus cords run deeper in the conventional lateral sagittal approach than in the costoclavicular approach for infraclavicular BPB that impedes needle visibility given the steep angle between the needle and US probe [5]. Contrastingly, the cervical roots and clustered cords in the interscalene groove and costoclavicular space, respectively, are within a relatively shallow depth compared with those in other approaches [33]. However, we could not perform subgroup analysis according to the approach type since only two and one RCT applied lateral sagittal BPB and interscalene BPB, respectively.
This study had some limitations. First, we included a relatively small number of studies. Therefore, large-scale and well-planned studies are warranted to confirm our results. Second, the control group comprised various BPB techniques that could have contributed to the heterogeneity. Third, none of the studies compared the incidence of HDP between the CCB and axillary approach that is a safe technique in terms of phenic nerve block [14].
In conclusion, among patients undergoing upper limb surgery, compared with other BPB techniques, CCB involves a lower incidence of HDP as well as comparable performance time, onset time, and block-related complications. Further large-scale and well-designed RCTs are warranted to strengthen the evidence and confirm our results.
Notes
Funding
None.
Conflicts of Interest
Jung-Hee Ryu has been an editor for the Korean Journal of Anesthesiology since 2018. However, she was not involved in the review process of this article, including peer reviewer selection, evaluation, or decision-making. There were no other potential conflicts of interest relevant to this article.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
Chang-Hoon Koo (Data curation; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft)
Insung Hwang (Data curation; Investigation; Methodology; Writing – original draft)
Hyun-Jung Shin (Data curation; Formal analysis; Methodology; Supervision; Validation; Writing – review & editing)
Jung-Hee Ryu (Conceptualization; Data curation; Formal analysis; Investigation; Supervision; Validation; Writing – review & editing)
Supplementary Materials
Search strategy for each database.
Level of evidence for each outcomes.
Forest plots for sensitivity analysis of incidence of hemidiaphragmatic paresis. Sensitivity analyses confirmed that RR remained stable, implying that any single study did not skew the significance. RR: risk ratio.
Funnel plots for the incidence of hemidiaphragmatic paresis.
Forest plots for subgroup analysis of hemidiaphragmatic paralysis according to the control group technique (Interscalene vs. infraclavicular vs. supraclavicular). According to the heterogeneity, we decided to random effect model.
Forest plot for postoperative peak expiratory flow rate.
Forest plot for other complications.
Forest plot for motor onset time.
Forest plot for performance time.
Forest plot for needle passage time.
Quality assessment. Green circle, low risk; Yellow circle, some concerns.