Introduction
Beach chair position (BCP) surgeries are associated with significant cerebral desaturation events (CDEs) in as many as 80% of patients [1,2]. Cerebral oxygenation is dependent on a combination of multiple factors such as cerebral blood flow (CBF), mean arterial blood pressure (MAP), partial pressure of oxygen, cardiac output, and hemoglobin levels. A reduction in MAP during anesthesia in BCP may decrease the CBF [3-5]. A strong association of the hypotensive response with decrease in regional cerebral oxygen saturation (rSO2) and jugular venous oxygen saturation (SjvO2) has been observed [6–8]. In such situations, pharmacological agents such as ephedrine and phenylephrine, which rapidly increase MAP, are frequently used to obtain indirect benefits on cerebral oxygenation. Alternatively, prophylactic measures have been successfully used to prevent CDEs, including non-pharmacological techniques such as preloading with crystalloids/colloids or the use of sequential compression devices (SCDs) [9–11]. Vasoactive agents administered prophylactically can theoretically achieve a rapid increase of MAP and consequently the increase of CBF, however, the decline observed in rSO2 suggests otherwise [12]. The association between the use of prophylactic compression stockings and reduced occurrence of CDEs is unclear, as similar incidences were also reported in patients with their use [13]. We could not find any analysis of pooled data in the available literature to support or refute this association.
Our study attempted to determine whether any particular pharmacological or non-pharmacological technique is useful for reducing CDEs during BCP surgeries. Confirming an association between the two would improve predictability, provide insight into the possible underlying pathophysiological mechanisms, and guide the anesthesiologist on the most efficacious method of preventing these undesirable events. Therefore, we performed a systematic review and meta-analysis to summarize the existing evidence on the ability of prophylactic measures to prevent CDEs in this clinical setting.
Materials and Methods
Registration and protocol
This meta-analysis was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses [14] and was registered with PROSPERO (https://www.crd.york.ac.uk/PROSPERO, no. CRD42020167285).
Eligibility criteria
We included prospective randomized clinical studies or randomized controlled trials (RCTs) with adult patients (> 18 years) who underwent elective shoulder surgeries in BCP. Reporting of monitored cerebral oxygen saturation-related data and at least one prophylactic method used to prevent CDEs were mandatory for inclusion. Publications in all languages were considered. The patients received one of the following anesthetic modalities: (1) planned general anesthesia (GA) or (2) regional anesthesia (RA), viz interscalene brachial plexus block or similar block in combination with GA. We excluded studies wherein patients underwent surgeries under RA alone, at < 45° BCP, or with American Society of Anesthesiologists physical status > 3.
Information sources
An electronic literature search, specifically restricted to randomized studies or RCTs of BCP, was conducted in MEDLINE, CINAHL (EBSCO host), Google Scholar, and the Cochrane Central Register of Controlled Trials. The bibliography of the retrieved manuscripts was searched for additional studies pertaining to data encompassing our primary outcome of interest. These included studies reporting incidence of CDEs, maximum and minimum average cerebral oxygen saturations, serial average cerebral saturation values overtime periods, critical CDEs, and the percentage change of cerebral saturations, with a caveat that both supine, pre-BCP and BCP data are available. Similar to cerebral saturation, SjvO2 was documented whenever data were available. Twenty-first-century literature, that is, literature published only after January 1, 2000, was scanned because anesthesia protocols have remained uniform during this period. Cohorts with matched controls, retrospective studies, reviews with inadequate information on primary outcomes of interest, abstracts, and letters to the editor were not included. The detailed search strategy is shown in Supplementary Material 1, which depicts the keyword-based search inclusion terms.
Study selection and data collection
A collection of studies was conducted by TPT and HK. The manuscripts meeting the inclusion criteria were assessed, and data were extracted following a standardized format by the same authors. The extracted items comprised study characteristics, risk of bias domains [15], participant disposition, and study outcomes. The PICO inclusion criteria comprised the following elements, focusing on patients, interventions, comparisons, and outcomes, and were used to identify components of clinical evidence. Patients who underwent shoulder surgery under anesthesia in BCP with cerebral oxygen saturation monitoring using any type of cerebral oximetry device were considered. They were categorized according to the type of surgery or anesthesia, number of patients, the position adopted for surgery, and monitoring for CDEs. Interventions referred to prophylactic measures used to prevent CDEs. These patients must have had at least one type of prophylactic method to prevent cerebral desaturation in the sitting position. With regard to the type of intervention, study authors could consider any type of pharmacological or non-pharmacological method deployed before the CDE. The comparison of variables was between ‘with and without’ prophylactic measures. This is an alternative to intervention–placebo, different drugs, measures, or therapy. Outcomes were classified as primary or secondary. The former included cerebral oxygen (de)saturation data with and without the use of prophylactic measures at various time intervals using rSO2 and SjvO2 cerebral oximetry values. The latter included the incidence of CDEs and hypotension episodes, associations with MAP, and the use of vasoactive agents with CDEs.
Data synthesis and analysis of outcomes
Data relevant to the outcomes of interest were extracted from each study in this meta-analysis. The rSO2 or SjvO2 data included continuous data documented as pooled averages or sequential data at various intervals for a study. Data were collected as a single or combined value in the form of mean and standard deviation (SD) or median and interquartile range (IQR), respectively. If multiple datasets were available, they were converted into pooled statistical averages. The other dichotomous data included the number of patients experiencing CDEs.
The data were tabulated before induction (baseline) and post-induction (relating to pre-BCP and BCP categories after stabilization of vital signs). The BCP rSO2 or SjvO2 data were pooled for the time periods mentioned in the respective publications. If the recorded data timings were non-specific, they were approximated to a specific time by a mutual discussion with the authors. Publications with unreported or inconclusive data that could not be obtained after attempts to contact the authors were excluded from this review.
To analyze cerebral saturation data, four categories of rSO2 or SjvO2 values were considered from the study (i.e., prophylactic measures used) and control (i.e., no prophylactic measures used) groups. The absolute values, which are mentioned as percentages, for both groups with respect to time (i.e., early or entire period of BCP) or for the type of outcome studied (i.e., rSO2/SjvO2) were recorded. These data were synthesized as pooled data that included (1) the early BCP period (rSO2/SjvO2 values, for immediate, the first 15 min of BCP), (2) the entire BCP period (all-time overall rSO2/SjvO2 values, until the reported time period or the end of surgery) referring to the pooled average values of those at all time points during BCP, (3) the lowest observed at BCP rSO2/SjvO2 values. When the right and left cerebral hemispheres were monitored separately (with either single or two different methods), the lowest value was included (4) the baseline values, which refer to the supine, pre-BCP rSO2 values after induction of anesthesia.
The data presented in tables, text, and images were used as the primary sources for extraction. Graph digitizing software (Engauge Digitizer version 10.10, @Mark Mitchell) was used to efficiently extract and estimate raw numerical data whenever textual numerical data were unavailable. When range and IQR were available, SD was estimated using the formulas SD = range / 4 and SD = IQR / 1.35, as described by the Cochrane Handbook for Systematic Reviews of Interventions [16]. Data are reported as 95% CI. The median value was used to estimate the mean if the value was not reported. Whenever the standard error of the mean (SEM) was reported, SD was obtained as SD = SEM × √N [16]. To account for drop-out cases over time or termination of BCP before the time specified in the meta-analysis, patient numbers were approximated to the nearest values for pooled data estimation. If the exact time point was not specified in the manuscript, then the approximated time point was considered by the authors’ judgment.
Individual definitions for CDEs and hypotension were accepted as described by each study. Dichotomous data such as the occurrence of CDEs and hypotension were converted into incidence (n/N) for early and overall time periods. All analyses were performed assuming no incidences of CDEs in the supine position under anesthesia. CDE occurrence was counted whenever the event was reported at least once, based on the original study authors’ definitions. Complications were analyzed on an ‘intention to treat’ basis since in some subgroups, patients were repositioned back to supine following BCP-induced hemodynamic disturbances or CDEs [17].
With regard to MAP, data evaluation and synthesis were similar to those applied for CDEs or rSO2/SjvO2 values. The incidence of hypotension was counted whenever the events were reported at least once either individually or sequentially for each patient.
Pre-defined sources of heterogeneity
To explore the potential causes of heterogeneity that could influence the primary outcomes, we pre-identified certain aspects of individual study groups. These included (1) anesthetic technique (GA vs. combined GA and RA); (2) induction agent (propofol vs. thiopentone); (3) maintenance anesthetic agent (propofol vs. inhalational agents); (4) prophylactic measures (vasoactive agents vs. preloading vs. SCD vs. targeted mild hypercarbia techniques vs. compression stockings vs. others), and (5) maintenance vasopressors (phenylephrine vs. ephedrine vs. others).
Meta-analysis was conducted using Review Manager (RevMan 5.4.1, Cochrane Collaboration, Denmark, 2014). A random-effects model was used for all analyses. Heterogeneity was measured and expressed as I2. For continuous variables (rSO2/SjvO2), mean differences (MDs) were compared using the inverse-variance (I-V) method. For dichotomous variables (incidence of CDEs and hypotension), odds ratio (OR) or risk ratio (RR) was computed using the Mantel-Haenszel (M-H) or I-V method. Natural log transformation was adopted [18], as the outcomes for incidences were expected to be non-normally distributed.
Meta-regression analysis
Because of overlapping of use (i.e., more than one) of different prophylactic measures, a meta-regression analysis was planned to estimate the effectiveness of the individual prophylactic measures. Pre-BCP (supine, after anesthesia induction) and BCP (all-time overall, absolute [%], and pooled) cerebral saturation values were considered for meta-regression. Meta-regression data inputs were different from the data of conventional meta-analysis, where the former included the MDs from baseline to all-time overall fall of rSO2 values. Meta-regression was performed using JASP software (Version 0.9.2, BibTeX, University of Amsterdam, the Netherlands). The effect size (estimate) and standard error (SE) were used for meta-regression. A priori defined prophylactic measures were used across the study groups. We included all prophylactic measures that were identified among study groups, such as compression stockings, SCDs, targeted mild hypercarbia, crystalloid loading, hydroxyethyl starch (HES), regional ischemic preconditioning technique (RIPC), and vasoactive agents for meta-regressions. Meta-regressions were also performed for ‘the number of patients experiencing CDEs’, in which baseline supine, pre-BCP CDEs were assumed as ‘zero’ for the analysis. All meta-regressions were performed using the restricted maximum likelihood method and random effects. An omnibus test of the model coefficients and tests for heterogeneity were used for the model. Simultaneous to Egger's regression tests for funnel plot asymmetry evaluations, a visual inspection of the funnel plot was carried out to rule out publication bias. The influence of such studies on the model was also assessed. The parameter covariance was assessed for the combined effects of prophylactic measures. Statistical significance was set at P < 0.05 (2-tailed).
Grading of Recommendations Assessment, Development and Evaluation
The certainty of the evidence was summarized using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) [19] approach for individual outcomes. The strength of recommendations reduces the potential to facilitate critical appraisal and improves the communication of judgments. GRADEpro GDT (GRADEpro Guideline Development Tool [Software], McMaster University, 2020 [developed by Evidence Prime, Inc.]) was used to facilitate the development of evidence summaries and recommendations.
Results
Literature identification and study characteristics
From 2,297 studies that were initially screened, 56 potentially relevant manuscripts were selected based on abstracts (Supplementary Material 2). Of these, 12 trials provided the data for analysis (Supplementary Material 3) [7,13,20-29] including Jadad scores. Data from 786 patients were included in the analysis.
Cerebral oxygenation monitoring was performed using INVOS™ 5100 B/C (Medtronic, Ireland) cerebral oximetry monitoring devices [7,13,20-27,29] (near-infrared reflectance spectroscopy) in all included studies in this review, except in a single study [28] in which the FORE-SIGHT™ device (Edwards Lifesciences, USA) was used. All the studies reported baseline data with respect to rSO2 including pre- and post-induction values, except for a single study [24] in which only the mean (SD) maximum fall of cerebral saturation values was reported. The physiologic principles to prevent CDEs followed in each included study, however, were dissimilar. Because rSO2 values can be affected by a variety of factors, the mechanisms used by the authors in the prevention of falls in rSO2 varied. Vascular tone, cardiac output, and cerebrovascular-mediated mechanisms were considered by the authors to preserve cerebral oxygenation. To simplify, we classified the included heterogeneous studies based on whether the study authors used pharmacological (PPMs) or non-pharmacological prophylactic measures (NPPMs). For the prevention of MAP-dependent cerebral desaturations, PPMs were used in four RCTs (vasoactive agents; vasopressin [20,21,25], n = 3 and phenylephrine [7], n = 1) and NPPMs in eight (preloading with colloid [HES 130/0.4 [22], n = 1]; SCD use on legs [26], n = 1; compression stockings [13,24], n = 2; targeted mild hypercarbia [27,28], n = 2; or reduced BCP angle for surgery [23] [low BCP angle, ≤ 60º, n = 1] or RIPC [29], n = 1]). However, overlapping prophylactic measures were observed among the study groups. Eight study groups [13,20,21,24] used compression stockings and five used SCDs [23,24,26] as a prophylactic measure. Crystalloid loading [7,21,22,29] and HES preloading [22,26,27] were used in 10 and 5 study groups, respectively. Vasoactive agent prophylaxis [7,20,21,25] was used in seven, whereas targeted mild hypercarbia [27,28] was used in two study groups. Similarly, low BCP angle [13,23,24] during surgery was used in five study groups. However, the RIPC technique was used in only a single study [29] group.
CDE was uniformly defined as > 20% decrease from baseline values and critical desaturation as < 55% (absolute value, Supplementary Material 3). Four studies [20,21,25,27] mentioned a duration of cerebral desaturation of > 15 s, whereas others had no duration stated. One study [29] additionally defined CDE as a fall in absolute values < 40% from baseline if it occurred for at least 1 min. Deliberate hypotension was accepted in one study [23]. All studies considered pharmacological agents for treating BCP-induced hypotension or treating CDEs via blood pressure elevation. The rest of the data related to treatment and prophylactic measures are depicted in Supplementary Material 3.
Primary outcomes
Absolute values of rSO2 for an early period
Pooled absolute rSO2 (comparisons with controls, Figs. 1A and 1B) values (in %) were obtained for the first 15 min of BCP. These were recorded from 10 studies; three used vasopressin as a PPM [20,21,25] and seven used NPPM techniques [13,22,23,26-29] to prevent CDEs. PPMs were associated with lower absolute rSO2 values than those without (controls). PPMs thus produced unfavorable results (vs. controls; MD: –13.58%, 95% CI [–16.03, –11.4], I2 = 0%, P = 0.97) in contrast to NPPMs (vs. controls; MD: 2.76%, 95% CI [0.62, 4.89], I2 = 56%, P = 0.03). Among NPPMs, the SCD and RIPC measures had statistically significantly higher rSO2 values than in those without their use.
Absolute values of rSO2 for all-time period
Pooled absolute rSO2 (comparisons with controls, Figs. 2A and 2B) values (in %) were obtained for all-time periods of BCP. These were recorded from 10 studies, four of which used PPMs (vasopressin [20,21,25] or phenylephrine [7] infusions) to regulate MAP. Preloading with HES [22], reduction of BCP angle [23], SCDs [26], and RIPC [29] were used in one study each, and targeted mild hypercarbia [27,28] was used in two RCTs. PPMs were associated with lower absolute all-time overall rSO2 values (vs. controls: MD, -12.23%; 95% CI, -14.59 to -9.87; I2 = 0%, P = 0.82) in contrast to NPPMs (vs. controls; MD: –12.23%, 95% CI [–14.59, –9.87], I2 = 0%, P = 0.82) in contrast to NPPMs (vs. controls; MD: 2.92%, 95% CI [0.34, 5.49], I2 = 76%, P = 0.0009). Among NPPMs, the use of SCDs, targeted mild hypercarbia, and RIPC measures had statistically significantly higher rSO2 values than those without their use.
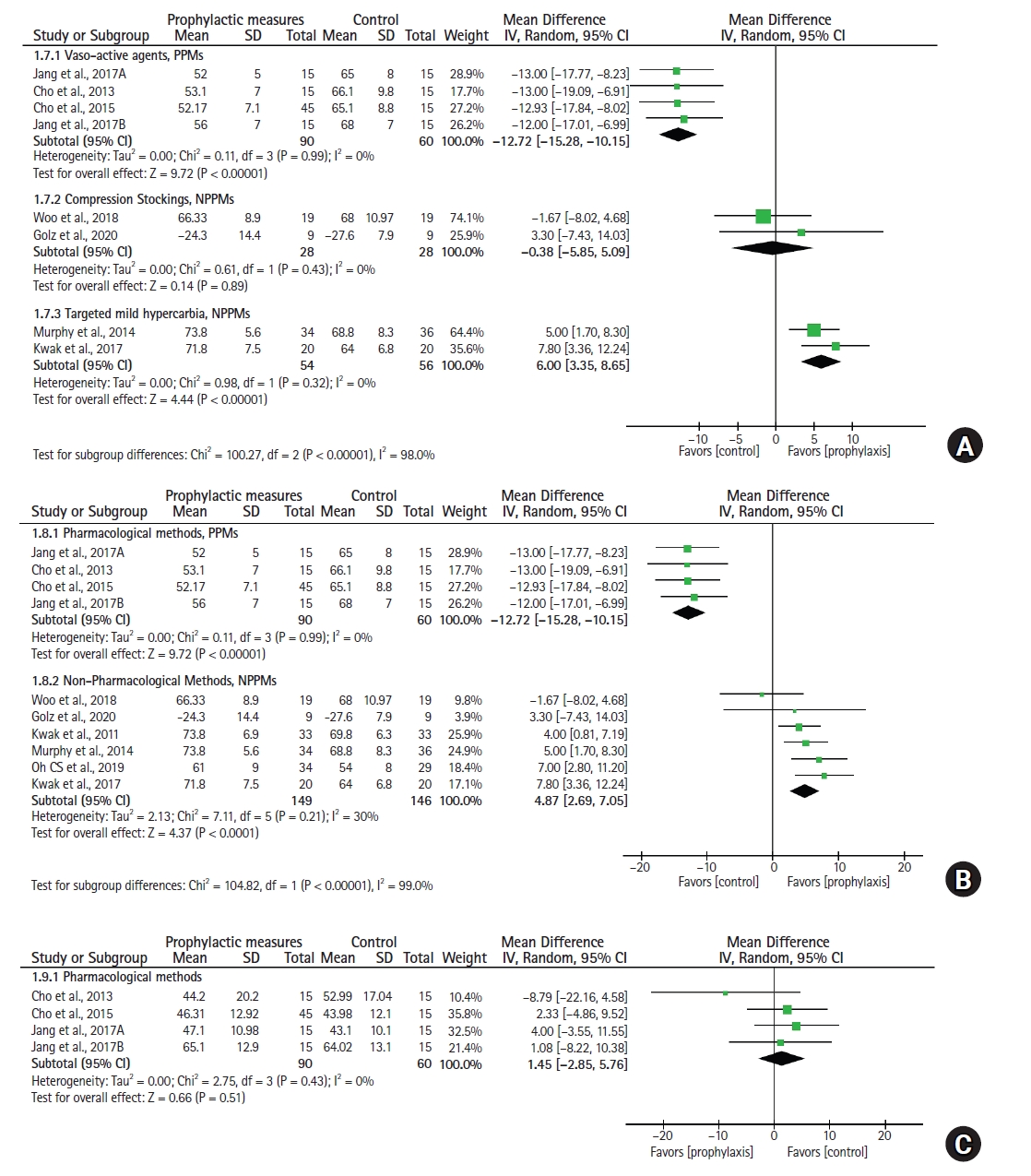
Lowest achieved absolute rSO2 values
The lowest achieved rSO2 (comparisons with controls, Fig. 3A and 3B) was recorded (in %) from nine studies. Three of these used PPMs (vasopressin [20,21,25] infusions), and NPPMs were used in others (preloading with HES [22], reduction of BCP angle [23], SCDs [26], and RIPC [29] techniques in one study each; targeted mild hypercarbia [27,28] in two). PPMs had lower rSO2 for ‘lowest achieved’ absolute values during BCP compared to their controls (MD: –12.72%, 95% CI [–15.28, –10.15], I2 = 0%, P = 0.99). However, the use of NPPMs was associated with higher values than in the control group patients for the same studied parameter (vs. controls; MD: 4.87%, 95% CI [2.69, 7.05], I2 = 30%, P = 0.21). More specifically, use of targeted mild hypercarbia, SCDs, and RIPC techniques had favorable effects on rSO2 compared to those without their use.
Prophylactic measures and SjvO2
The SjvO2 values (comparisons with controls, Fig. 1C, 2C, and 3C) were recorded for only the PPM subgroup in three studies [20,21,25] (150 patients). Arginine vasopressin (AVP) was used in all studies, and both rSO2 and SjvO2 were monitored. The early, all-time overall and lowest achieved SjvO2 values were considered for analysis. With the use of prophylactic AVP infusions, the study group had comparable values to those of the control group patients, indicating the absence of beneficial effects of AVP in BCP. Furthermore, in contrast to rSO2, the negative effects of AVP were not observed for the BCP SjvO2 values.
Meta-regression results for ‘baseline to all-time overall rSO2 differences’
Meta-regression analysis included 11 studies [7,13,20–23,25–29]. One study [24] did not report baseline values; therefore, the study was not considered for meta-regression analysis. Meta-regressions revealed a statistically significant highest estimate (estimate: 7.8, SE: 1.534, 95% CI [4.8, 10.8], P < 0.001) for vasoactive agent prophylaxis use (PPMs, higher positive coefficients represent a greater fall of rSO2 in BCP compared to supine) compared to NPPMs (Table 1A). The use of SCDs, crystalloid loading, targeted mild hypercarbia, HES, and RIPC had beneficial effects (visual analysis of coefficients, Table 1A). The use of compression stockings and maintenance of a low BCP angle during surgery failed to demonstrate these benefits. In contrast, targeted mild hypercarbia, HES, and RIPC techniques had statistically significant coefficients (Omnibus P < 0.001, test for heterogeneity P = 0.646, Egger’s P = 0.514, Table 2; for publication bias [30], Supplementary Material 4A). Among all NPPMs, the targeted mild hypercarbia technique had the lowest estimates (estimate: –5.5, SE: 1.408, 95% CI [–8.2, –2.7], P < 0.001), indicating its superior beneficial effects over others (Wald test, P < 0.001).
Secondary outcomes
Number of patients developing CDEs
Ten studies reporting patients with CDEs [7,13,20–24,27–29] were included, and two [7,29] of these declared only patients with critical CDEs. Meta-analysis (Fig. 4A) revealed that use of PPMs showed a significantly higher risk of developing CDEs than that of the control groups (vs. controls; RR: 4.01, 95% CI [1.82, 8.81], I2 = 0%, P = 0.75). In contrast, there was no difference observed between NPPMs and their respective controls (vs. controls; RR: 0.44, 95% CI [0.18, 1.10], I2 = 75%, P = 0.001).
Incidence of hypotension
Ten studies [7,13,20–22,25–29] reported episodes of hypotension. Both methods (PPMs and NPPMs) effectively reduced the incidence of hypotension (for PPMs vs. controls; OR: 0.13, 95% CI [0.06, 0.28], I2 = 0%, P = 0.42, and for NPPMs vs. controls; OR: 0.27, 95% CI [0.10, 0.74], I2 = 54%, P = 0.07) (Fig. 4B).
Vasopressor consumption
Phenylephrine was used in five studies [20,21,23,24,29], and ephedrine in nine [13,20,21,24–29] (combined use in five studies [21,23,24,27,29]), as vasopressors for the treatment of BCP-induced hypotension. The diversity in pattern and dose of individual vasopressor use precluded any analysis of their effect on altering the CDEs.
A few studies compared cerebral desaturations with respect to time-person observations, such as time from induction or time from upright positioning to the onset of CDE, and average cumulative CDE durations. However, the data were inadequate for additional analyses. Serious adverse neurological outcomes (as reported by all studies) and postoperative cognitive dysfunction (as reported by three studies [20,21,25]) were not observed. One study [28] reported nausea and vomiting with low incidence in the study group (nausea/vomiting, 3/0 vs. 12/1, P < 0.05).
Meta-regression results for ‘number of patients experiencing CDEs’
Meta-regression analysis of the number of patients experiencing CDEs (Table 1B) included 10 studies [7,13,20-24,27-29]. Two studies [25,26] did not report the incidence with respect to the number of patients; therefore, they were not considered in the meta-regression analysis. Meta-regressions revealed statistically significant highest estimate (estimate: 5.73, SE: 7.632, 95% CI [–9.2, 20.7], P = 0.452) for vasoactive agent prophylaxis use (PPMs, positive coefficient represents a higher number of patients experiencing CDEs) compared to that for NPPMs. Among all NPPMs, the targeted mild hypercarbia techniques had the lowest estimates observed, indicating its maximal effects over others (estimate: –12.31, SE: 10.14, 95% CI [–32.2, 7.6], P = 0.225). However, to statistically confirm the observations, poor model fit and high heterogeneity were limitations. We observed no statistically significant P values for any of the prophylactic measures used (Omnibus test for model coefficient P = 0.459; fit measure log-likelihood = -50.15, AIC = 120.3; Table 1B; for publication bias [30], see Supplementary Material 4B).
Subgroup analysis of PPMs, targeted mild hypercarbia, and compression stockings
Two studies [27,28] included 110 patients for the targeted mild hypercarbia techniques. End-tidal CO2 values of 40-42 and 30-35 mmHg were used during BCP in the study and control patients, respectively. Subgroup analysis revealed targeted mild hypercarbia as an effective measure in preserving cerebral oxygenation ([vs. controls; MD: 4.93%, 95% CI [2.45, 7.41], I2 = 0%, P = 0.83, Fig. 2A] and [vs. controls; MD: 6.00%, 95% CI [3.35, 8.65], I2 = 0%, P = 0.32, Fig. 3A], for all-time overall and lowest achieved absolute rSO2, respectively). Similar to the above results, targeted mild hypercarbia successfully prevented the fall of rSO2 values from supine-baseline values to BCP (supine vs. BCP; MD: 1.56%, 95% CI [–0.71, 3.83], I2 = 6%, P = 0.30, n = 108). This is in contrast to control patients without targeted mild hypercarbia use, in whom a significant fall of rSO2 values from supine-baseline to BCP was observed (supine, pre-BCP vs. BCP; MD: 6.14%, 95% CI [3.08, 9.2], I2 = 36%, P = 0.21, n = 112). Furthermore, the number of patients not developing CDE was 13 times higher than for those not using targeted mild hypercarbia techniques at BCP (OR, nonevent: 13.18, 95% CI [3.84, 45.24], I2 = 0%, P = 0.94, n = 110). Use of compression stockings [13,24] (n = 104) failed to demonstrate benefits, as the odds ratio remained less than 1 (OR, non-event: 0.77, 95% CI [0.33, 1.77], I2 = 0%, P = 0.45). Furthermore, the lowest achieved rSO2 was not different from that of control patients when compression stockings were used as a prophylactic measure (vs. controls; MD: –0.38%, 95% CI [–5.85, 5.09], I2 = 0%, P = 0.43, n = 56).
Risk of bias and heterogeneity
The risk of bias summary and graph are presented in Figs. 5A and 5B, respectively. Selection bias (biased allocation to interventions) due to inadequate generation of a randomized sequence was noted in one study [23], and selection bias due to inadequate concealment of allocations prior to the assignment occurred in a few studies [20,21,23]. Blinding is difficult [13,23,28] in BCP surgeries, although most studies were double-blinded. Therefore, performance bias and detection bias due to knowledge of the allocated interventions by participants and personnel during the study were observed in a few studies [13,28]. Further, we observed selective reporting (reporting bias) in a few [7,24], with incomplete outcome data such as reporting only ‘critical’ desaturations and mentioning ‘maximum fall’ of rSO2 from baseline values. The observed low heterogeneity for PPMs precluded further analysis, as opposed to that of NPPMs. As described earlier, the latter group included the use of different prophylactic techniques. Therefore, the results of subgroup analyses of NPPMs are uncertain because of the uneven covariate distribution among groups. Furthermore, an insufficient number of studies per group was observed. Therefore, all these factors necessitated additional meta-regression analysis. To explore the potential causes of heterogeneity that could influence primary outcome results, anesthetic factors such as the type of anesthesia and induction or maintenance agents were not considered separately, primarily due to inadequate data.
GRADE evidence
The relevant summary results are presented in Table 2 with GRADE evidence. The certainty of the evidence is summarized as ‘moderate’ for the outcome of ‘early, all-time overall, and lowest achieved rSO2/SjvO2 values’ since the risk of bias was ‘serious’ in nature. The certainty of the evidence is similar for the targeted mild hypercarbia technique. For the rest of the studied outcomes, the certainty of the evidence is described as ‘low’ since ‘inconsistency’ and ‘imprecision’ were ‘serious’.
Discussion
In our meta-analysis, we evaluated the efficacy of different prophylactic measures employed to prevent cerebral desaturation during shoulder surgeries performed in BCP. We observed that not all prophylactic measures were successful, and the methods did differ in efficacy. Our current study provides concrete evidence that PPMs cannot effectively prevent cerebral desaturation. The benefits of a few NPPM techniques, such as targeted mild hypercarbia, for maintaining cerebral oxygenation during BCP are also evident. However, a few trials have confirmed the protective effects of HES preloading, and studies of SCDs or RIPC are scarce. Our meta-analysis unequivocally confirmed the negative effect of vasoactive agents on rSO2 values (but not on SjvO2), highlighting their failure in protecting patients from CDEs despite their ability to prevent hypotension.
A pervasive issue in the pharmacologic prophylaxis portion of this meta-analysis is the extracranial contribution (contamination) [31] to cerebral oximetry, which must be acknowledged. This can be explained to a large extent as a ‘paradoxical effect’ of vasopressors on oximetry values when given to support blood pressure. Our analysis demonstrated that prophylactic vasoactive agents can decrease rSO2 values. However, to confirm whether this decrease truly reflects cerebral desaturation, additional analysis was needed. SjvO2-metry is a more accurate assessment of the balance between oxygen supply and demand in the brain, albeit globally. Therefore, we simultaneously analyzed the effects of PPM on both rSO2 and SjvO2. The discrepancy between rSO2 and SjvO2 necessarily describes the effects of PPMs on regional oximetry values. The other finding of this study is the inefficacy of vasoactive agent prophylaxis in preventing fall of cerebral oxygen saturation. Despite the higher SjvO2 recorded over rSO2, AVP failed to demonstrate any beneficial effect, in that its use did not prevent the fall in SjvO2 during BCP. In contrast to rSO2, the SjvO2 values of the PPM subgroup were similar to those of the control groups, in both the supine, pre-BCP and BCP periods. A single phenylephrine study was included in the PPM subgroup. However, in the absence of SjvO2 monitoring in the same study, we were unable to describe the extracranial effects of phenylephrine on rSO2 monitoring. The association of AVP, CDEs, and postoperative cognitive dysfunction have also been reported in the past [32]. While some NPPMs were superior to vasoactive agent prophylaxis with respect to CDE incidence, their role in preventing cognitive dysfunction was not evaluated in our study. Reports on the effect of AVP on cerebral oxygenation in animal models have been conflicting [12,33]. Beyond auto-regulation values of MAP, AVP improves CBF via nitric oxide-mediated cerebral vasodilatation [34], and this was the rationale for its use in some of our included studies.
In this review, the effectiveness of individual prophylactic measures (especially NPPMs) was analyzed through a separate analysis. Drawing conclusions on NPPMs was not possible, as we have lumped together with a disparate and diverse group. Importantly, since no study authors used a single measure to prevent cerebral desaturation, analyzing a single method (such as NPPMs) could be misleading. Therefore, the more appropriate method of meta-regression analysis was performed. Our analysis confirmed the beneficial effects of a few NPPMs, such as targeted mild hypercarbia, HES, and RIPC. Targeted mild hypercarbia during these procedures must be performed with caution and must not be performed to the exclusion of blood pressure support. Hypercarbia impairs cerebral autoregulation and puts the patient at a higher risk for cerebral hypoperfusion, should hypotension occur at the same time. Additional subgroup analysis established stronger evidence for targeted mild hypercarbia use. Few prospective studies [35] investigating the effects of targeted mild hypercarbia on rSO2 during major surgery have confirmed similar effects.
One of the interpretations of this meta-analysis is that NPPMs in combination can be effectively deployed during BCP surgery to enhance rSO2; this conclusion could be relevant to clinicians in maintaining cerebral oxygenation. For example, targeted mild hypercarbia of 40-42 mmHg during controlled ventilation, appropriate preloading (HES), and concomitant use of SCDs can significantly reduce CDEs. The routine use of RIPC as a prophylactic measure has not yet been recommended. While a previous prospective cohort study [9] demonstrated the efficacy of compression stockings in reducing the incidence of CDEs, our meta-regression results failed to confirm this. Confounding factors such as MAP, hemoglobin level, cardiac output, angle of BCP maintained, and partial pressures of oxygen and carbon dioxide, which can influence rSO2 values, were kept constant in the RCTs included. We believe that the study authors excluded patients with cardiopulmonary disease or anemia because of possible negative effects on rSO2 values.
While PPMs were inferior to a few NPPMs in the prevention of CDEs (coefficient evaluation), both exhibited similar effects with respect to lowering the incidence of hypotension (vs. controls). Thus, PPMs were unable to achieve the ultimate therapeutic benefit, despite maintaining MAP. The association of episodic decrease in MAP with the incidence of cerebral desaturation and its direct correlation with cerebral oximetry values remain unconfirmed [36,37]. Several studies have demonstrated no direct correlation between blood pressure and cerebral (de)saturation values (Supplementary Material 5) [13,38-43]. However, cardiac output has been claimed as a factor that correlates well with rSO2 values in BCP-neurosurgical patients [40]. Targeting MAP alone may not be the ideal approach to prevent CDEs in BCP surgeries.
Over 80% of the patients in this meta-analysis were treated with ephedrine for BCP-related hypotension. Phenylephrine and ephedrine are commonly used for this indication. While treating hypotension in a non-BCP setting, the former was shown to decrease cerebral oxygen saturation even with correction of arterial blood pressure [44]. According to cardiac output rather than arterial blood pressure, it has been concluded that treating hypotension using vasoconstrictors to avoid cerebral hypoxia actually accomplished the opposite result [44,45]. In contemporary practice, approximately 70% of BCP-related hypotension episodes are still treated with phenylephrine. It would be prudent to choose a different vasopressor and to use the more physiological NPPMs. Additionally, while targeting cardiac output to maintain cerebral oxygenation, the use of NPPMs with ephedrine (as a vasopressor of choice to treat hypotension) could possibly be a desirable combination. Currently, the use of cerebral oximetry in patients with BCP is limited in availability. Under these circumstances, especially in susceptible patients, this combination is gaining significance.
Our study had some limitations. Higher heterogeneity values represent different NPPM methods applied over cohorts. The type of anesthesia, maintenance anesthetics, Fraction of inspired oxygen concentration, and other co-variables could have partially influenced the outcomes. The definition of ‘event’ could vary according to the authors’ perception, and this could have a bearing on the incidence reporting. The range of rSO2 values may be significantly larger when measured with INVOS™ devices compared to FORE-SIGHT™, but the exact underlying reasons for these differences remain unknown [46]. The use of phenylephrine to treat hypotension episodes in subgroups of NPPMs could have possibly influenced the CDEs in a few studies, which is an inherent contradiction in the analysis. The difference in the timing of the application of NPPMs poses significant analytical challenges. Moreover, none of the included NPPMs reported SjvO2 data. The use of pooled data and presuming the baseline data of rSO2 values to be uniform for all patients may be another limitation. Non-availability of raw patient data and non-reporting of time-person observations for groups or lowest achieved cerebral desaturation data for many trials precluded conducting individual patient meta-analysis or correlations.
In conclusion, the evidence favors the prophylactic use of targeted mild hypercarbia techniques to effectively reduce BCP-CDEs and best preserve cerebral oxygenation. Evidence does not favor the use of prophylactic vasoactive agents for the prevention of cerebral desaturations, irrespective of whether their use interferes with cerebral oximetry readings. One may use a combination of a few NPPMs as prophylactic measures; however, an RCT investigating the effect of combined use of all NPPMs could conclusively demonstrate the benefits. At the same time, comparisons of prophylactic as well as therapeutic effects of different vasoactive agents (such as phenylephrine vs. ephedrine) for BCP-CDEs could set the direction for future research in this field.