Although the peripheral nervous system is commonly involved in cancer patients, it is rarely affected in leukemia [1ŌĆō4]. Leukemic infiltration of the peripheral nerves (neuroleukemiosis) presents with non-specific symptoms depending on the nerve affected. Special diagnostic tools should be considered in patients presenting with this non-specific constellation of symptoms. Current diagnostic modalities include magnetic resonance imaging (MRI), positron emission tomography/computerized tomography, electromyography/nerve conduction studies, and studies of cerebrospinal fluid and bone marrow. However, these modalities are expensive, invasive, and time-consuming.
This case report was approved by the Institutional Review Board of The Catholic University of Korea, Yeouido St. MaryŌĆÖs Hospital (SC20ZESE0024).
Case Report
A 70-year-old man in his sixth year of remission from acute myeloid leukemia was referred to the pain clinic in July 2017 from the department of neurology for shooting and radiating pain in the left posterior compartment of the leg and sole of the foot that was progressively worsening. The pain intensity was 7/10 according to a numerical rating scale, and the nature of the pain was spontaneous, lancinating, and was accompanied by a sensation of extreme cold. Examination revealed mild calf muscle atrophy of the left leg and decreased power (grade 3/5) on plantar flexion and inversion of the left ankle. The left deep tendon ankle reflex was absent.
The electromyography/nerve conduction studies showed reduced response of the left posterior tibial nerve. A lumbar spine magnetic resonance imaging (MRI) showed diffuse lumbar disc degeneration and mild bulging of the L2-3 disc with left foraminal extension, which were insufficient to explain the patientŌĆÖs symptoms. On infrared thermography, hypothermia in the left leg was observed (Fig. 1). Laboratory findings, including complete blood cell count, C-reactive protein, erythrocyte sedimentation rate, etc. were all normal. Symptomatic pain management with non-steroidal anti-inflammatory drugs, high doses of gabapentin, tricyclic antidepressants, and serotonin-norepinephrine reuptake inhibitors were ineffective. Opioid (oxycodone hydrochloride) was effective only at high doses (80 mg/day). Additional lumbar epidural block and piriformis injection based on the patientŌĆÖs symptoms before the electromyography/nerve conduction studies were done, but the patientŌĆÖs pain was not alleviated.
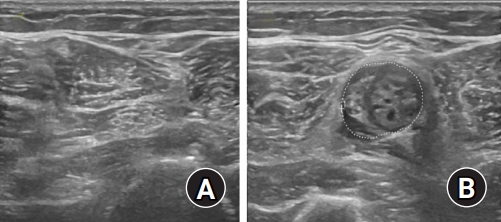
Based on the electromyography/nerve conduction results, we planned for sciatic nerve block. Before the block, we examined both sciatic nerves using ultrasound and found an enlarged hypoechoic and edematous mass on the left sciatic nerve at mid-thigh level (Fig. 2). The sciatic nerve block was conducted using guided ultrasound in the sub-gluteal region. Mepivacaine (10 ml, 0.5%) was injected on the thin triangular shaped nerve inside the fascial plane between the gluteus maximus and quadratus femoris muscles. After the sciatic nerve block, the pain was temporarily relieved.
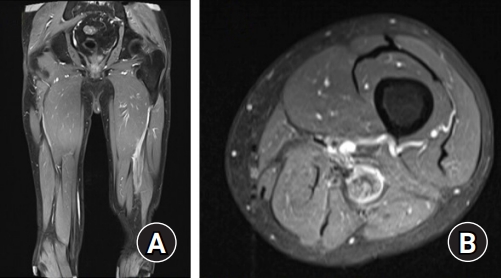
MRI of the left thigh showed diffuse swelling and internal enhancement of the left sciatic nerve, with peri-lesional fluid collection at mid- to distal-thigh level (Fig. 3). Cerebral spinal fluid and bone marrow studies were conducted to exclude the possibility of relapse of leukemia in peripheral nerves, and no abnormal findings were observed in the test. However, neuroleukemiosis was confirmed by histology of biopsy obtained under general anesthesia in October 2017. Based on the biopsy findings, the patient was started on chemotherapy (cytarabine). The neuropathic pain and motor weakness persisted. After two months from time of referral, he died of pneumonia.
Discussion
Neuroleukemiosis is a very rare complication of leukemia. Until now, only 15 cases have been reported (Table 1) [1ŌĆō12]. Including the case described in this report, the mean age of patients was 40.2 years, and four patients were aged < 20 years. Among the 15 cases, 10 (66.7%) were men. All cases involved Ōēź one extremity, and four (including the current one) involved only one extremity. In most of the cases (73.3%), neuropathy appeared during the remission period. A sensory deficit was observed in all patients and most (93.3%) had motor weakness. Autonomic deficit was reported in only two cases. The most underlying leukemia was acute myeloid leukemia. In most cases (73.3%), the symptoms developed during the remission period, had led to misdiagnosis or delayed diagnosis. Because nerve conduction, cerebrospinal fluid, and bone marrow studies showed inconsistent findings, confirmation of neuroleukemiosis was through biopsy or autopsy. In this current case, we could not decide on a nerve biopsy as it could have worsened the motor weakness because the sciatic nerve is a mixed nerve.
The blood-nerve barrier consists of tight junctions, which separates the peripheral nerve from the circulating blood. Neuroleukemosis is thought to be caused by infiltration of leukemic cells into the nerves after disability of the blood-nerve barrier by unknown factors [13]. Intractable neuropathic pain, numbness, and weakness can be the first signs of neuroleukemiosis. With only neuropathic symptoms present, it is easy to misdiagnose a leukemic mass infiltrating the peripheral nervous system, especially if the blood smear and bone marrow biopsy are negative for leukemia [12]. Differential diagnosis for neuroleukemiosis include Guillain-Barre syndrome, neurotoxicity from chemotherapy and abscess [5]. Nerve biopsy is the gold standard method, but nerve conduction study and radiological investigations, especially MRI and positron emission tomography are helpful in localizing the lesion [13]. Most treatments combine systemic chemotherapy and radiation therapy. When selecting the chemotherapy regimen, agents that can penetrate the blood-nerve barrier should be used [13]. In addition, peripheral nerve blockers may be performed to relieve the patientŌĆÖs pain. The presence of neuroleukemiosis portends poor outcome [13].
Ultrasound is a simple device that is often used to guide nerve block. An ultrasound examination has an advantage over other diagnostic tools for peripheral nerve diseases in that it is both accurate and quick [14]. An abnormal finding can be found by fully examining the nerves from proximal to distal using ultrasound, and comparing them with the opposite nerve structure. The main pathologic findings upon ultrasound of the peripheral nerve are enlarged nerve, increased hypo- or hyper echogenicity, enlarged fascicles, increased thickness of the epineurium, and increased endoneural/perineural blood flow [15]. Although ultrasound findings alone are not sufficient to confirm, the above-mentioned abnormal findings can be found by comparing left/right, digital/proximal regions. Compared with electromyography/nerve conduction studies, ultrasound was found to be a simpler diagnostic and screening tool for peripheral nerve sheath tumors such as neurofibromatosis, also enables targeted MRI analysis.
Because neuroleukemiosis is a rare complication of leukemia, its diagnosis can be overlooked and therefore delayed, affecting prognosis. Ultrasound examination is a simple, inexpensive, non-invasive, and quick diagnostic modality for diseases causing peripheral neuropathy, including neuroleukemiosis.
For our patient, a diagnosis of neuroleukemiosis was delayed for six months because of the non-specific symptoms manifested during remission period of acute myeloid leukemia. Moreover, results from the complete blood cell count, cerebrospinal fluid, and bone marrow studies were normal. Initially, we suspected that the patientŌĆÖs pain resulted from radiculopathy originating in the spine. However, upon ultrasound we observed an enlarged hypoechoic and edematous segmental mass on the sciatic nerve with normal adjacent muscle. No fluid collection was detected around the nerves since the pathological process occurred inside the nerve membrane owing to the invasion of the nerve membrane. Radiculopathy that originates from the lumbar spine usually shows no signs of peripheral nerve edema. If trauma was the cause, damage to muscles around the nerve should be observed, but in this case, only nerve lesions were observed. These findings were different from radiculopathy caused by disc herniation and trauma; hence, we quickly ruled out these etiologies.
In this case, we described a patient with unexplained new-onset neuropathy due to leukemic infiltration of the peripheral nerve during remission period. Ultrasound is helpful when patients with neuroleukemiosis have difficulty using MRI or photoitron emission tomography as a cost issue, or when it is difficult to perform a biopsy immediately.