Introduction
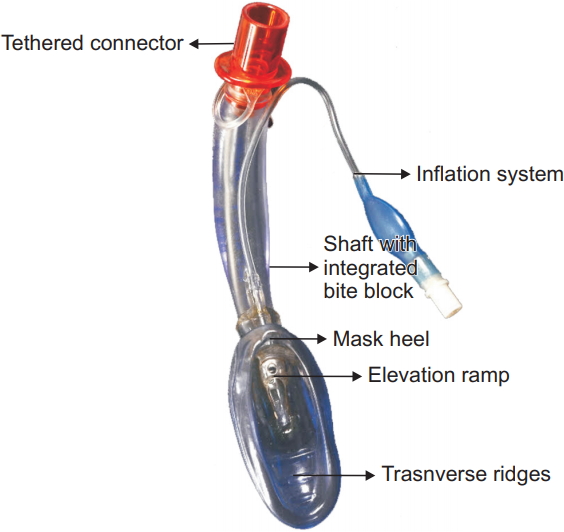
The Air-QŌōć laryngeal mask airway (LMA) (Cook gas LLC, USA; Fig. 1) is a second-generation supraglottic airway device (SAD) developed by Daniel J. Cook. It has been specifically engineered for use as a primary airway device as well as a conduit for tracheal intubation in anticipated or unanticipated difficult airways in children and adults [1].
Its other advantages include being user-friendly, available in sizes small enough to be used in the pediatric age group, and providing adequate airway control in both mechanically ventilated and spontaneously breathing children despite unfavorable pediatric airway anatomy [1,2].
The anatomical differences in pediatric airways could complicate the proper placement of SADs [3]. It is paramount to assess the techniques to improve positioning of Air-Q, because improper position can cause laryngeal obstruction and inadequate seal. The fiber-optic bronchoscope (FOB) helps in assessing the position of the Air-Q.
Since the introduction of Air-Q, there are numerous studies assessing it as a conduit for tracheal intubation in adults and children and comparing the efficacy of the device with other SADs [4ŌĆō10]. Previous studies documented that fiber-optic laryngeal view using the midline insertion technique for Air-Q was better than other SADs in children [1,6,11]. Based on their clinical experience with 100 patients, Jagannathan et al. [7] stated in their study that rotational technique was the best technique for Air-Q insertion.
The classic midline and rotational techniques have been compared for the insertion of Classic LMA, Softseal LMA, and Proseal LMA [3,12,13]; however, there are no studies comparing the laryngeal view of the midline and rotational insertion techniques of Air-Q. Therefore, our primary objective was to compare the FOB assessment of Air-Q position using these two insertion techniques. Based on a study conducted by Jagannathan et al. [7], we hypothesized that the FOB assessment of Air-Q position after insertion using the rotational technique would be better than the midline technique in the pediatric age group.
Our secondary objective was to compare the ease of Air-Q insertion with each technique with respect to the number of attempts for successful insertion and duration of insertion. Hemodynamic changes during insertion, oropharyngeal leak pressure (OPLP), and occurrence of complications such as trauma, laryngospasms, and hypoxemia were compared.
Materials and Methods
This randomized study was conducted in the Department of Anesthesia and Intensive Care, Postgraduate Graduate Institute of Medical Education and Research (PGIMER), Chandigarh, from August 2015 to November 2016, and was registered in the Clinical Trial Registry of India (CTRI/2018/09/015574). After gaining protocol approval from the Institutional Ethics Committee (INT/IEC/2015/724) and written informed parental consent, 80 pediatric patients of American Society of Anesthesiologists (ASA) physical status I /II of either sex were enrolled. These patients were aged between 5ŌĆō12 years, weighing 10ŌĆō30 kg, and were scheduled for elective surgery in supine position (cataract surgeries, inguinal hernia, or urethroplasty) under general anesthesia. Operative time for all the surgeries was less than 45 minutes and anesthetic duration was less than one hour.
Children with history of upper respiratory tract infection (cough, fever, rhinorrhea) within three weeks or on the day of surgery, respiratory tract pathology (oropharynx or larynx), anticipated difficult airway, increased risk of aspiration, gastro-esophageal reflux disease, non-fasting status, hiatus hernia, lung diseases, and cardiorespiratory or cerebrovascular diseases were excluded.
Eighty pediatric patients were randomly and equally assigned to the classic midline technique group and rotational technique group (n = 40, each) using a computer generated random number table. The random numbers assigned were concealed in opaque, sealed envelopes.
After confirming fasting status of patients according to the Standard Nil Per Os guidelines [14], standard ASA monitoring for heart rate (HR), saturation of peripheral oxygen (SpO2), non-invasive blood pressure, and end tidal carbon-dioxide was attached in the operating room. The patients were induced with 100% oxygen and sevoflurane (6ŌĆō8%), following which intravenous cannula was inserted and 2 ╬╝g/kg of fentanyl was administered. With end tidal sevoflurane concentration of 2.5% before device insertion, the depth of anesthesia was confirmed by the absence of motor response to jaw thrust [15].
The appropriate size of the Air-Q, based on the weight of the patient, was inserted using the allocated technique. In the classic midline technique group, the Air-Q was inserted using the manufacturerŌĆÖs recommendations. By stabilizing the patientŌĆÖs neck and head with the non-dominant hand, the patientŌĆÖs mouth was opened. The lubricated Air-Q mask was placed at the base of the tongue with a slight forward angle, and the Air-Q was placed in position by gently applying downward and inward pressure. Correct placement was determined by resistance to further advancement of the device.
In the rotational technique group, the Air-Q was inserted with its lumen facing backwards. Once the resistance in the posterior pharyngeal wall was felt, the device was rotated through 180 degrees and then passed downwards into position.
After insertion, the cuff of the Air-Q was inflated as per the recommendations (0.5 ml and 1 ml for sizes 1.5 and 2, respectively) to maintain cuff pressure in the range of 20ŌĆō30 cmH2O, and the breathing circuit of anesthesia machine was attached to the proximal end of the Air-Q. Adequate bag movements and chest rise confirmed airway patency, and capnography was monitored for adequate ventilation [16].
If any airway obstruction or inadequate ventilation with significant leak was observed, the Air-Q was reinserted using the same technique. When the second attempt failed, the other technique was used to insert the device. The anesthesiologist was blinded to the technique used and assessed the laryngeal view using FOB (size 3.5 mm OD; Pentax, Japan). The position of the tip of the FOB at the distal outlet of the Air-Q was used to determine the score of the laryngeal view. Grade scoring was based on the standard established scoring system by Jagannathan et al. [10] for FOB grading of laryngeal view through Air-Q:
Grade 1: Only vocal cords seen
Grade 2: Vocal cords and posterior surface of epiglottis seen
Grade 3: Vocal cords and tip of anterior surface of epiglottis seen (< 50% of obstruction to vocal cords by epiglottis)
Grade 4: Epiglottis down-folded and its anterior surface seen (> 50% of obstruction to vocal cords by epiglottis)
Grade 5: Epiglottis down-folded and vocal cords cannot be seen directly
If the FOB grades were 1 and 2, the Air-Q position was considered optimal, while FOB grades 3 to 5 indicated a sub-optimal position. At the end of the surgery, the Air-Q was removed under deep plane of anesthesia. Patients were monitored for time taken for successful insertion of the device, number of attempts and any complications after removal of device including laryngospasm, hypoxemia (SpO2 below 92%) and trauma (blood on the device after removal).
Statistical analysis
As since there were no previous studies comparing the two techniques of Air-Q insertion using FOB assessment in pediatric patients, the sample size was calculated on the basis of the results obtained by the Classic LMA study [3]. Sample size calculation was performed based on the assumption that the incidence of better FOB grades 1 and 2 would improve from 62% with the classic midline technique to 92% with the rotational technique. With an alpha error of 0.05 and a power of 90%, 37 patients in each group would be required. To account for attrition/dropouts, 80 patients were enrolled.
Discrete categorical data was represented in the form of either a number or a percentage (%); continuous data assumed to be normally distributed was represented as mean and standard deviation or as median and interquartile range, as per the requirement. The normality of quantitative data was checked using the Kolmogorov-Smirnov tests of normality. Statistical analysis was performed using the paired t-test for continuous variables and Wilcoxon signed rank test for categorical data. P value < 0.05 was considered statistically significant. All the statistical tests were two-sided and performed at a significance level of ╬▒ = 0.05. Analysis was conducted using International Business Machines Statistical Package for the Social Sciences (IBM SPSS) Statistics (version 22.0).
Results
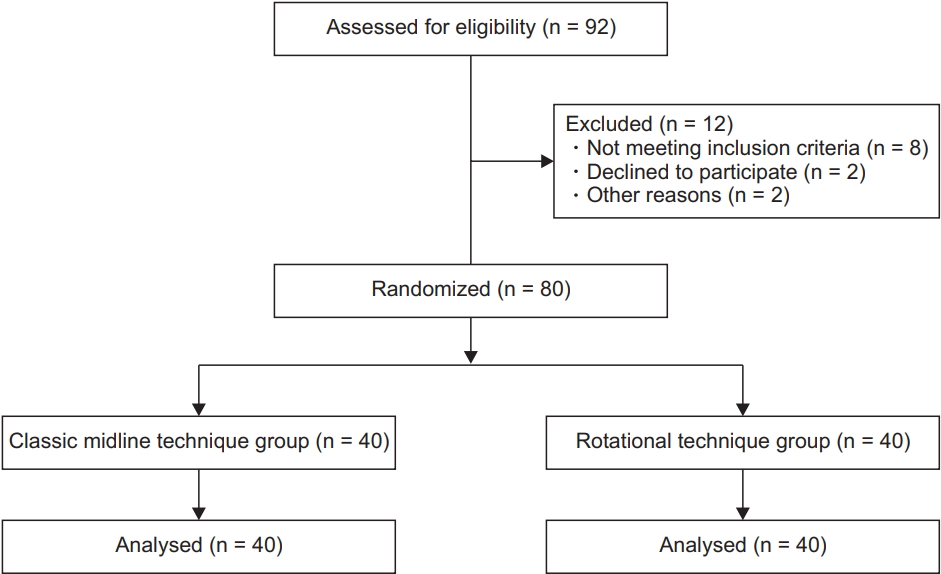
The demographic data of age, sex, and weight of patients as well as the sizes of Air-Q used were comparable in both the groups (Table 1). The Consort flow diagram of enrolled patients is shown in Fig. 2.
Ideal position (FOB grade 1) and optimal position (FOB grade 1 and 2) of Air-Q were better observed in rotational technique group than in classic midline technique group with a statistically significant difference. The time taken to successfully insert the Air-Q was significantly lesser in the rotational technique group (7.2 ┬▒ 1.5 s) than in the classic midline technique group (10.2 ┬▒ 2.1 s) (P < 0.001) (Table 2). The Air-Q could not be successfully inserted in two patients of the classic midline technique group, and an alternate technique was used. These two patients were excluded in the analysis of the time taken to insert the Air-Q device.
Successful insertion of Air-Q in the first attempt was comparable between both groups. The overall success rate of Air-Q insertion (successful insertion in two attempts) was statistically similar for both the techniques: 100% with the rotational technique and 95% with the classic midline technique (Table 2).
Ease of Air-Q insertion was better with rotational technique than classic midline technique but was not statistically significant. In 15% of the classic midline technique patients and 5% of the rotational technique patients, Air-Q insertion was moderately difficult but was not statistically significant (P = 0.105) (Table 2).
The mean OPLP of Air-Q was statistically similar in both the groups (Table 2).
Similar complications after removal of the device were observed in both groups. Two (5%) patients in the classic midline technique group showed laryngospasm, but no such complication was observed in the rotational technique group. Blood on the device was seen in two patients in the classic midline technique group and in one patient in the rotational technique group (Table 3).
The HR and mean arterial pressure (MAP) were noted during pre-induction, post-insertion, post-induction, 5 min after insertion, 10 min after insertion, and 15 min after insertion, and analyzed using the two-way repeated measured analysis of variance (ANOVA) test within the groups.
The increase in mean HR post-insertion was significantly higher in the classic midline technique group. There was no significant difference in the subsequent readings of both groups. There was no statistically significant difference in the MAP of both the groups at all times.
Discussion
Our study suggested that insertion of Air-Q using the rotational technique showed better FOB grading than the classic midline technique. The time taken to insert the Air-Q was significantly lesser with the rotational technique than with the classic midline technique. To the best of our knowledge, this is the first study in the literature comparing these two techniques of Air-Q insertion in children. All other authors have used either the classic midline technique or the rotational technique of insertion of Air-Q in pediatric patients.
With respect to the rotational technique of Air-Q insertion, our results were comparable with those of Jagannathan et al. [7], in which the fiber-optic view was superior with the rotational technique of insertion in children with anticipated difficult airway.
The results obtained with the classic midline technique of Air-Q insertion in our study corroborated with that by Darlong et al. [9], wherein optimal FOB grading (grades 1 and 2) was seen in 84% children subjected to classic midline technique of Air-Q insertion. However, these findings do not corroborate with that by Whyte et al. [11], Sinha et al. [2], and Jagannathan et al. [1], where the optimal FOB grading was seen in 58%, 65%, and 68% of pediatric patients, respectively. This difference was apparent because these studies had a large number of children with no visible vocal cords, because they used size 1 of Air-Q along with sizes 1.5 and 2.
The time taken to insert the Air-Q using the classic midline technique in our study was similar to that reported by Jagannathan et al. [6] of 11.1 ┬▒ 1.5 s. On the other hand, it was different in the studies by Darlong et al. [9] and Sinha et al. [2], wherein the time taken to insert the device using the classic midline technique was 16.3 ┬▒ 1.5 and 13.3 ┬▒ 3 s, respectively. This difference in insertion time of the device was because of the difference in the definitions of insertion time. In these studies, insertion time was defined as the time from picking up the device to obtaining the square waveform of capnography, whereas our study defined it as the time from mouth opening to the confirmation of airway patency.
In our study, we observed that the success rate of device insertion in the first attempt and ease of insertion was 95% with the rotational technique and 80% with the classic midline technique, and the difference was not statistically significant. Our results of the first attempt success rate with rotational technique of Air-Q insertion were similar to that of Jagannathan et al. (100%) [7]. In other studies by Sinha et al. [2], Darlong et al. [9], and Jagannathan et al. [1], the first attempt success rate using the classic midline technique was in the range of 95ŌĆō100%, which did not correlate with results of our study for the same technique. This could be because of the use of neuromuscular blockade in those studies, which altered the tone of the airway musculature and improved the ease of insertion, and thus the first attempt success rate of insertion in children.
We found that the OPLP did not vary with the technique of insertion of Air-Q (22.6 ┬▒ 1.8 cmH2O and 23.3 ┬▒ 1.4 cmH2O for rotational technique and classic midline technique, respectively). In previous studies by Darlong et al. [9] and Whyte et al. [11] with the classic midline technique of Air-Q insertion in pediatric patients, the OPLP of Air-Q correlated with our study (20.2 ┬▒ 4.6 cmH2O and 23 cmH2O, respectively in neutral position). In contrast to our study, the OPLP in studies by Jagannathan et al. [1] and Sinha et al. [2] using the classic midline technique of Air-Q insertion was 19 ┬▒ 5.4 and 18.5 ┬▒ 1.8 cmH2O, respectively. This could be attributed to the different age groups and weight parameters.
In our study, we did not find any statistically significant difference in the complications associated with the rotational and classic midline techniques of Air-Q insertion. Although laryngospasm and blood on the device was seen in 5% of patients of the classic midline technique group and in 2.5% patients of the rotational technique group, our study was not powered to calculate the small differences in complications. Our results were similar to those of previous studies by Whyte et al. [11] and Darlong et al. [9], where blood on the devices was seen in 5% and 3.1 % of pediatric patients undergoing the classic midline technique of Air-Q insertion, respectively.
The ease of insertion, first attempt success rate of insertion, OPLP, and associated complications were similar for both the techniques of Air-Q insertion, suggesting the use of the rotational technique as an alternative to classic midline technique of Air-Q insertion in pediatric patients. However, because of better FOB grading and lesser time taken to insert the device with the rotational technique, it could be the technique of choice for optimal positioning of Air-Q and for intubating through Air-Q in pediatric patients.
There are certain limitations in this study. Since only healthy children with normal airway anatomy were studied, our results cannot be extrapolated to those with complicated airway anatomies. Only two sizes of Air-Q were studied (1.5 and 2), because size 0.5 was introduced recently. Further studies with sizes 1 and 0.5 of Air-Q are necessary. As our study was performed on children under spontaneous ventilation during surgery and were not administered with muscle relaxant, these results may not be applicable to those administered with neuromuscular blockade for positive pressure ventilation.
We conclude that the rotational technique of Air-Q insertion is associated with better FOB view and is faster when compared to the classic midline technique in pediatric patients. Complications such as blood on the device and laryngospasm had similar incidences in both the groups. Hence, the rotational technique of Air-Q insertion could be the technique of choice in children for optimal Air-Q positioning and for intubation through Air-Q.