Introduction
Rotational thromboelastometry-guided (ROTEM-guided) bleeding management is an essential part of patient blood management (PBM) which is an important concept in improving patient safety [1].
The treatment of bleeding is to stop the bleeding and to avoid the need for massive transfusion that is associated with high morbidity and mortality [2–5]. Prophylactic and/or inappropriate plasma and platelet transfusion does not prevent bleeding and transfusion and is associated with worse outcomes including mortality [6–11]. Two-thirds of transfusion-related mortality is based on transfusion-related acute lung injury (TRALI), transfusion-associated circulatory overload (TACO), and transfusion-related immunomodulation (TRIM) with hospital-acquired infections [12].
Ratio-based transfusion concepts do not correct coagulopathy and do not reduce mortality in patients with severe hemorrhage [13–17]. Ratio-based concepts do not stop bleeding. It just gains time to identify the reason for bleeding (coagulopathic and/or surgical) and to perform adequate hemostatic interventions to stop bleeding. Accordingly, some centers are using a hybrid approach starting with a ratio-based transfusion concept until coagulation data are available and enable a more effective targeted hemostatic therapy [18].
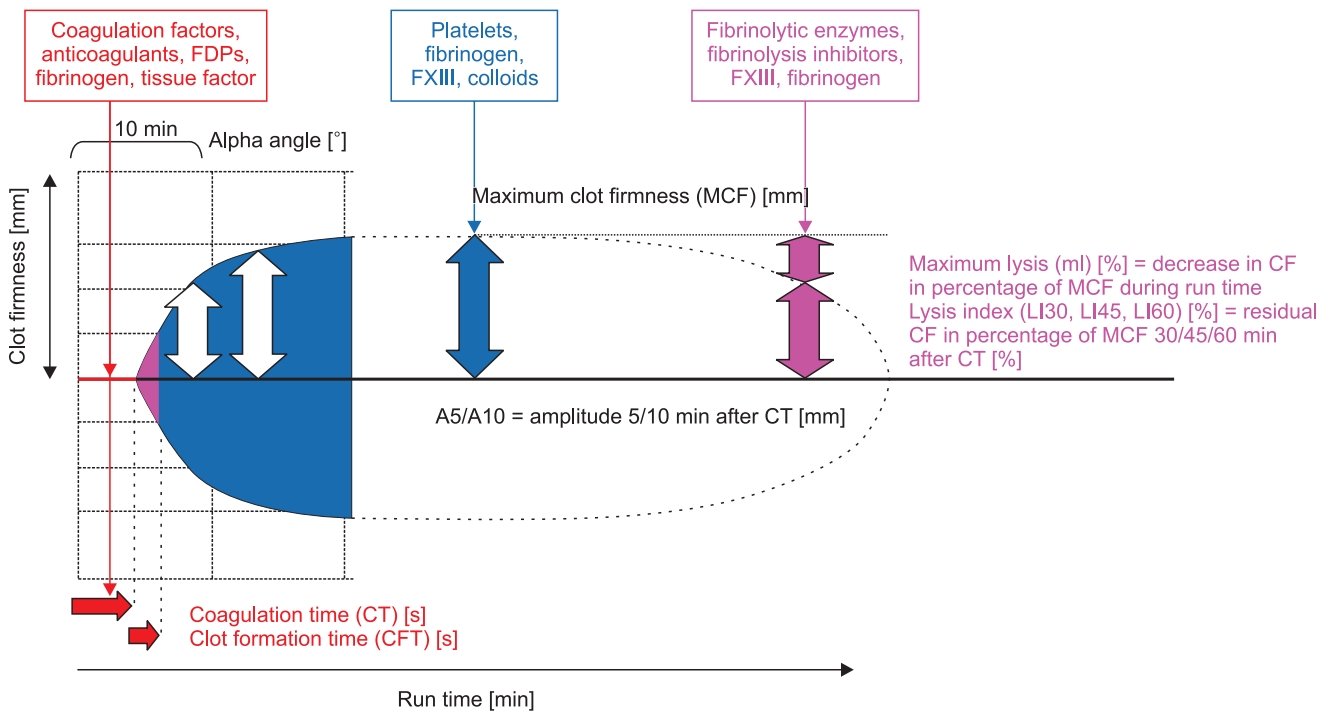
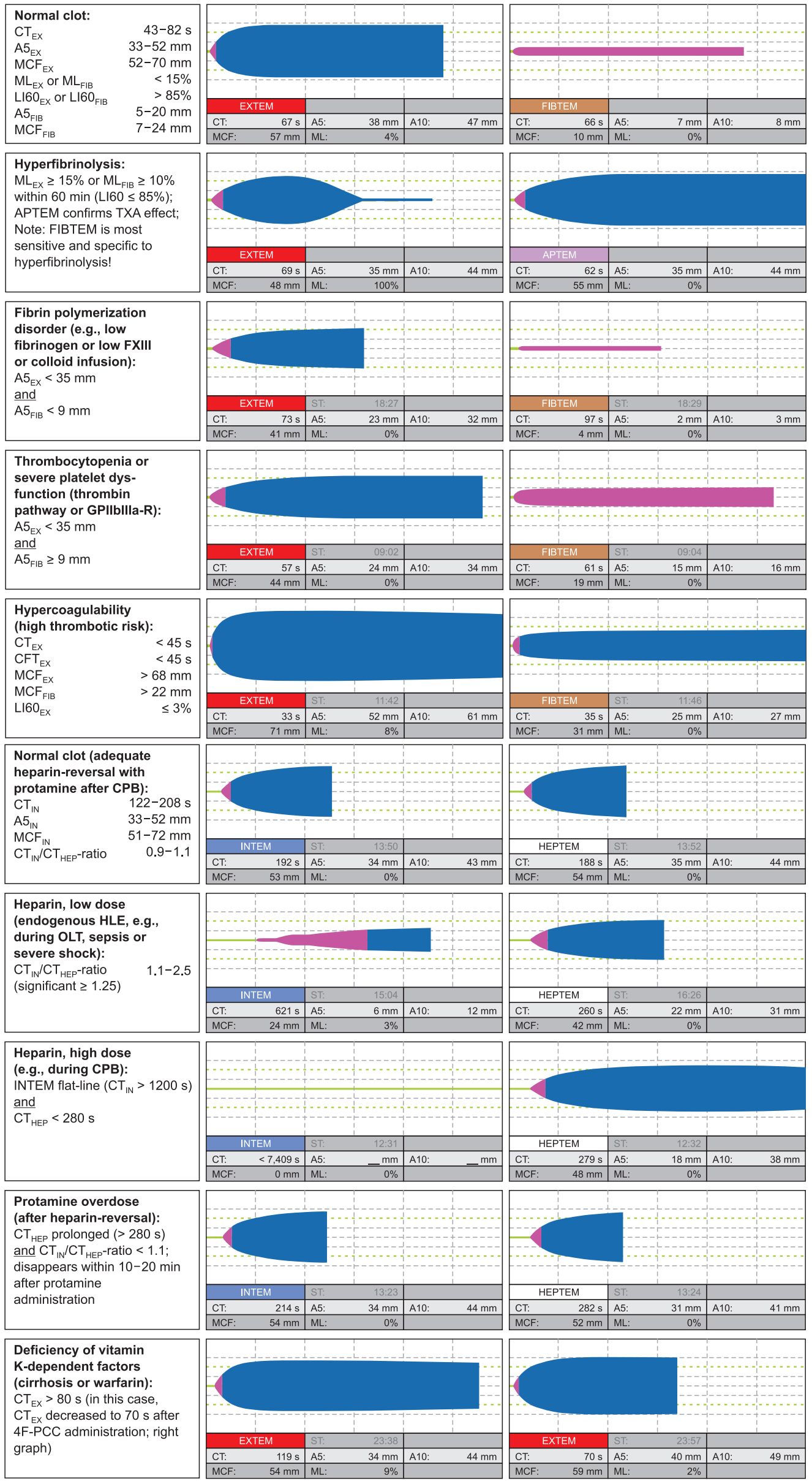
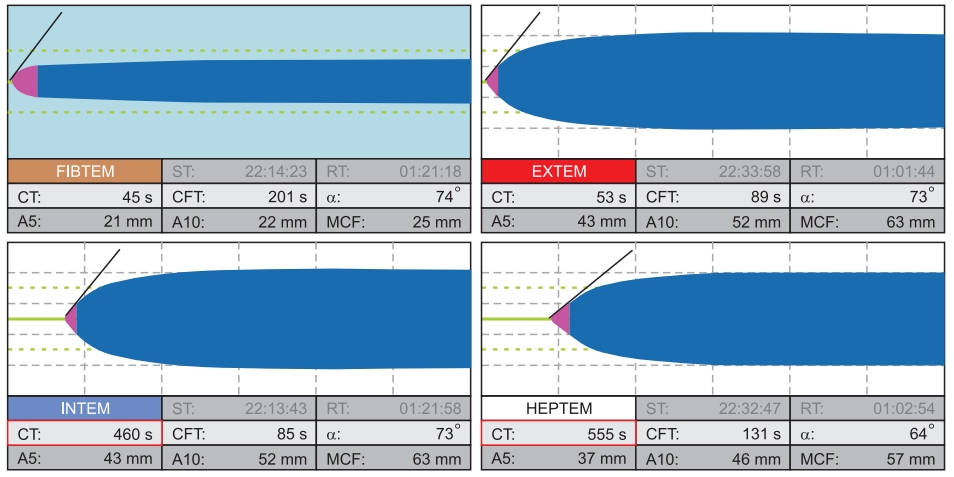
Time is life in severe bleeding! Here, the turnaround time of standard laboratory coagulation tests (SLCT) is too long (30–90 min) to guide clinical decisions [19–21]. In contrast, point-ofcare (POC) ROTEM provides test results within 10–15 min, as shown in Fig. 1. Here, early amplitudes of clot firmness at 5 and 10 min after the time to initiate clotting (coagulation time, CT), e.g., amplitude of clot firmness 5 min after CT (A5; actually not yet available in the US) and amplitude of clot firmness 10 min after CT (A10; early clot firmness parameter also available in the US), correlate very well with maximum clot firmness (MCF), plasma fibrinogen concentration, and platelet count and are essential for a short turnaround time of ROTEM analysis (Table 1 and Fig. 2) [21–26]. POC ROTEM testing does not only enable a shorter turnaround time compared to SLCTs, but these assays (such as FIBTEM) are also superior to SLCTs (such as plasma fibrinogen concentration) to predict bleeding and transfusion in several clinical settings [27–31].
ROTEM-guided bleeding management algorithms have been shown to be effective in reducing transfusion requirements, health care costs, and complication rates. Several randomized clinical trials (RCTs), meta-analyses, and health technology assessments provided evidence that using ROTEM-guided algorithms in bleeding patients resulted in improved patient’s safety and outcomes including perioperative morbidity and mortality [32–36].
Accordingly, ROTEM-guided algorithms implement the concept of personalized or precision medicine in perioperative bleeding management (‘theranostic’ approach). However, the implementation of ROTEM in the PBM concept requires adequate technical and interpretation training, education and logistics, as well as interdisciplinary communication and collaboration.
Basic Concepts of POC ROTEM-guided Bleeding Management Algorithms
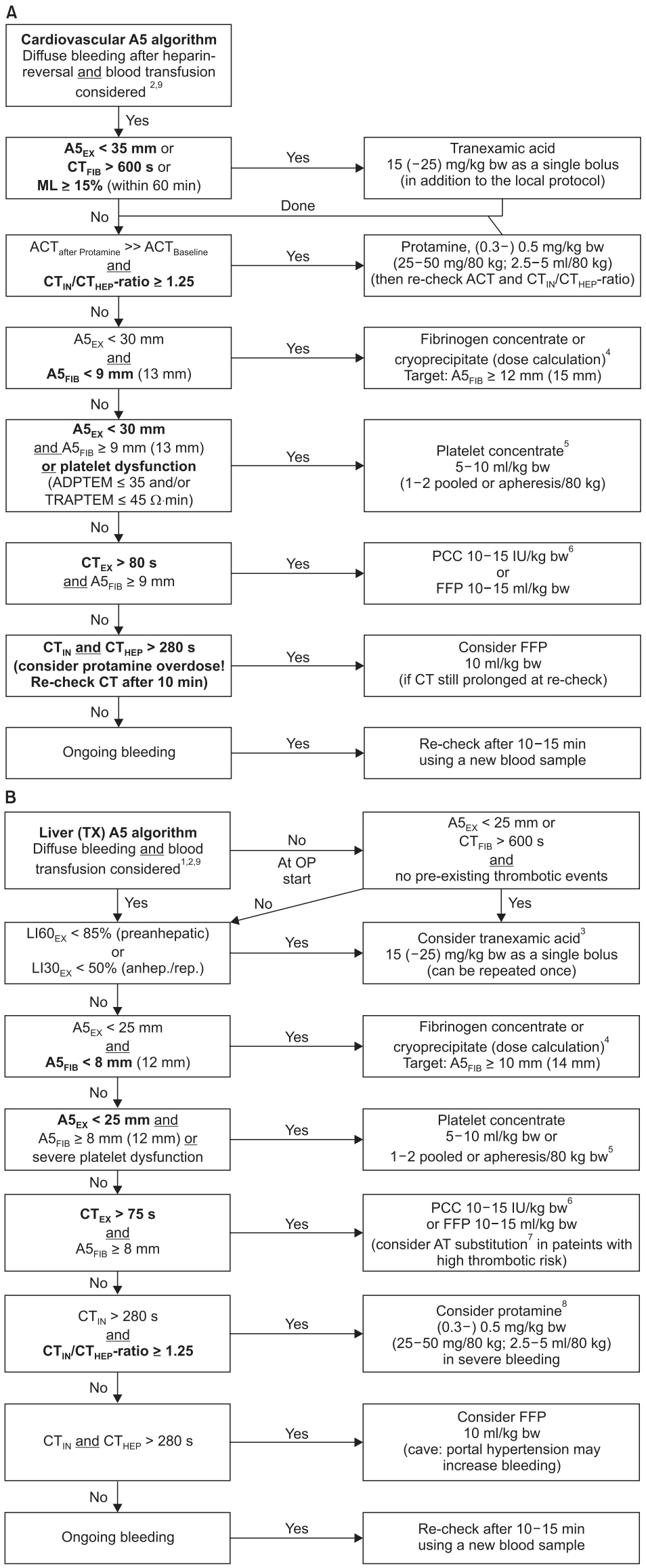
All presented ROTEM-guided algorithms are based on a similar structure. The aims of algorithms include administering the right hemostatic intervention(s), in the right dose (fibrinogen and platelet dose calculation, Table 2), at the right time (‘Treat first what kills first!’), and in the right sequence, as shown in Figs. 3 and 4.
The first step is always the presence or absence of clinically relevant bleeding and the potential need for blood transfusion. The second (and maybe third) step deals with important setting-specific issues such as fibrinolysis management and anticoagulation reversal (cardiovascular surgery). The next two steps take care for clot firmness management (fibrinogen and platelet transfusion).
A fibrinogen deficiency is most often associated with a prolonged CT in EXTEM assay (CTEX). Therefore, only if the FIBTEM clot amplitude in the early 5 and 10 min tracing (A5FIB or A10FIB, respectively) is adequate, CTEX values can be interpreted adequately. In other words, ROTEM results should be interpreted in a reasonable sequence (A5FIB prior to CTEX) as given by the algorithms, not according to their availability (CTEX prior to A5FIB). This avoids potential misinterpretation of ROTEM results. The other reason is that fibrinogen concentration drops down first in severe bleeding before thrombin generation is affected (except in bleeding due to anticoagulants or hemophilia). Furthermore, an increase in thrombin generation seems to be associated with a higher risk of thromboembolic complications compared to a substitution of substrates—in particular, fibrinogen. Therefore, clot firmness management, e.g., a reduced A5FIB and A5 in EXTEM assay (A5EX), should precede thrombin generation management, e.g., a prolonged CTEX and CT in INTEM assay (CTIN).
ROTEM reference ranges have been established for several populations of healthy individuals (geographically, US and non-US), neonates, infants, children, adolescents, and adults, as well as for pregnant women (1st–3rd trimester and peri-partum) [37–42]. However, the reference ranges describing the 95% prediction interval for a specific population of healthy individuals can be used for orientation only and are not designed to predict bleeding or transfusion requirements.
Cut-off or trigger values (e.g., used in ROTEM algorithms) to guide clinical decision-making are determined in setting-specific observational studies by receiver operating characteristics (ROC) curve analysis or multivariate regression analysis [27–31,43–45].
Target values for ROTEM-guided algorithms have been validated by setting-specific interventional trials to assess whether a therapeutic intervention results in the achievement of hemostasis, reduction in transfusion requirements, and/or improvement in patient outcomes [32,45,46].
The following rules have to be considered when using ROTEM-guided bleeding management algorithms.
• Avoid any inappropriate blood transfusion or hemostatic intervention.
• ROTEM is not designed to answer the question ‘Will this patient bleed?’ but ‘Why does this patient bleed?’
• The first decision in every ROTEM-guided bleeding management algorithm presented in Figs. 3 and 4 is the clinical question whether diffuse (coagulopathic/microvascular) bleeding is present and blood transfusion has to be considered. If the answer to this clinical question is ‘No,’ the ROTEM algorithm ends at this point.
• Accordingly, don’t treat pathologic laboratory results (‘numbers’) in the absence of bleeding (low positive predictive value of SLCTs [14%–24%], viscoelastic [15%–24%], and platelet function testing [27%–50%]) in order to avoid any overtreatment that might result in thromboembolic events and increased health care costs [31,47,48].
• Use the high negative predictive value of viscoelastic (90%–97%) and platelet function testing (80%–95%) in ROTEM algorithms (that excludes reasons for bleeding). Accordingly, ‘Not-to-do (restrictive) POC ROTEM algorithms’ consider only hemostatic interventions with a high potential to stop the bleeding but avoid thromboembolic events (‘therapeutic window’ concept) [31,47,48].
• If both, POC viscoelastic (ROTEM delta or ROTEM sigma) and platelet function testing (ROTEM platelet) are normal, surgical bleeding has to be considered and treated adequately.
• However, the limitations of every diagnostic device and assay have to be considered (e.g., effect of antiplatelet drugs and von Willebrand disease for viscoelastic testing) [49].
Thromboelastometry and Whole Blood Impedance Aggregometry Devices and Reagents
The ROTEM system includes the semi-automated ROTEM delta system that works with a computer-driven automated pipette and provides four independent channels for viscoelastic testing and, in combination with the ROTEM platelet module, two additional channels for whole blood impedance aggregometry for POC platelet function analysis. Accordingly, the ROTEM platelet module covers the blind spot of thromboelastometry. The ROTEM sigma device is a cartridge-based fully-automated thromboelastometry system, and its cartridge includes four assays (actually EXTEM C, FIBTEM C, INTEM C, and APTEM C [type 1 or complete cartridge] or EXTEM C, FIBTEM C, INTEM C, and HEPTEM C [type 2 or complete + hep cartridge]). Here, no pipetting is needed and the closed blood sampling vial can be connected to the cartridge. In particular, the ROTEM sigma can easily be handled at the point-of-care by the medical staff without pipetting skills.
Three different types of reagents are used in the ROTEM system. First, there are the so-called liquid reagents (LR) for the ROTEM delta system (Table 1) that require several pipetting steps by combining 1–2 different liquid reagents for each assay. Here, the extrinsically activated assays EXTEM, FIBTEM, and APTEM contain the heparin inhibitor polybrene that inactivates up to 5 IU/ml unfractionated heparin. This enables the use and interpretation of these assays even under high heparin concentrations, such as on cardiopulmonary bypass (CPB) [50–52]. The ‘beads’ reagents used in the ROTEM sigma cartridges perform in the same way and the results are stored in the database under the terms EXTEM C, FIBTEM C, and APTEM C. Furthermore, the so-called single use reagents (SUR) are available for ROTEM delta and ROTEM platelet (Table 1). However, the ROTEM delta SURs have an important limitation:
Notably, the SURs for the assays EXTEM S, FIBTEM S, and APTEM S do not contain a heparin inhibitor. Therefore, SURs must not be used in patients treated with unfractionated heparin (UFH) (e.g., in cardiovascular surgery or in patients with therapeutic anticoagulation with UFH) as well as in patients in whom a significant endogenous liberation of heparinoids can be expected (e.g., after graft reperfusion in liver transplantation or in patients with severe shock). UFH can result in prolonged CT and clot formation time (CFT) as well as in reduced clot firmness (A-values and MCF) by using SURs in these settings. A heparin effect can be verified by the test combination INTEM (S) and HEPTEM (S).
ROTEM-guided Algorithms in Different Clinical Settings
In cardiovascular surgery
Most patients undergoing cardiac surgery already might get antifibrinolytic drugs prophylactically according to a local protocol. In this case, ROTEM-guided management of fibrinolysis is of minor importance.
In complex cardiac surgery, heparin-neutralization in liquid reagents (ROTEM delta) and cartridges (ROTEM sigma) allows for ROTEM analysis in blood samples with high heparin concentrations at the end of CPB, e.g., at aortic declamping [32,46,52–55]. This enables the timely ordering of blood products such as cryoprecipitate and platelet concentrates—in particular, if factor concentrates such as fibrinogen concentrate are not available. During cardiac surgery, the time window to perform hemostatic interventions is limited to 30–45 min between heparin-reversal by protamine and chest closure/transport of the patient to the intensive care unit (ICU). Therefore, a short turnaround time of POC testing and a short ‘time-to-treat’ are most important in this setting.
Detection of a residual heparin effect or a protamine overdose is essential in cardiovascular surgery before other hemostatic interventions are considered (step 3 of the algorithm in Fig. 3A). Notably, a prolonged activated clotting time (ACT) is not specific for a residual heparin effect. In centers using a 1 : 1 ratio between the primary heparin dose and the protamine dose administered for heparin reversal, a protamine overdose might even be more often the reason for an elusive ACT prolongation. Ichikawa et al. [56] reported a very weak correlation between ACT (r = 0.12) as well as activated partial thromboplastin time (APTT) (r = 0.36) and the heparin concentration determined by the anti-Xa activity. In contrast, the CTIN/CTHEP-ratio correlated well (r = 0.72) with the anti-Xa activity. Furthermore, Ichikawa et al. demonstrated that an anti-Xa activity below 0.2 U/ml corresponding to a CTIN/CTHEP-ratio below 1.25 was not associated with increased postoperative mediastinal blood loss. In contrast, protamine overdose is not only associated with an elusively prolonged ACT (inhibition of factor V activation), CTIN/CTHEP-ratio ≤ 1, but also with a significant and long-acting inhibition of platelet function including the adenosine diphosphate (ADP)- and thrombin receptor-activating peptide (TRAP)-pathway [57–60]. RCTs confirmed that a protamine overdose is associated with a significant increase in blood loss, transfusion requirements, and need for re-surgery after cardiac surgery [61,62]. Therefore, a 1 : 1 ratio between primary heparin dose and protamine dose cannot be recommended. Here, a heparin to protamine ratio of 1 : 0.6–0.8 seems to be more effective [56,61,62]. Additional protamine administration is definitively not beneficial in patients with a prolonged ACT due to a protamine overdose.
Furthermore, a low FIBTEM amplitude has to be considered as a reason for a prolonged ACT, CTIN, CTHEP, and CTEX— in particular, in children undergoing cardiac surgery, since fibrinogen levels are diluted quickly in this patient population, as described ahead [63]. Fibrinogen is a key factor for bleeding after cardiovascular surgery since it is diluted and consumed quickly during and after CPB. Karkouti et al. [64] demonstrated that a post-CPB fibrinogen level below 2 g/L—that corresponds to an A5FIB < 9 mm (A10FIB < 10 mm) [21]—is associated with a significantly increased probability of transfusion of ≥ 5 U red blood cells (RBCs). This is in line with the results reported by other authors [52,65] and the reason to set the cut-off value for fibrinogen/cryoprecipitate substitution to A5FIB < 9 mm in the cardiovascular algorithm. Ranucci et al. [66–69] demonstrated that fibrinogen substitution in cardiac surgery is very effective to stop bleeding in patients with hypofibrinogenemia but that a substitution higher than an A5FIB of 16 mm (corresponding to a plasma fibrinogen concentration of about 3 g/L) does not show any further improvement. Therefore, the first target in our cardiovascular algorithm is an A5FIB ≥ 12 mm (fibrinogen concentration ≥ 2.5 g/L) and the second target (if bleeding continues in complex cardiovascular surgery) is an A5FIB ≥ 15 mm (fibrinogen concentration ≥ 3 g/L). An A5FIB ≥ 12 mm (fibrinogen concentration ≥ 2.5 g/L) may compensate for thrombocytopenia (< 100/nl) or platelet dysfunction after CPB [53,70]. The dose calculation for fibrinogen concentrate or cryoprecipitate are based on the targeted increase in FIBTEM amplitude and presented in Table 2 [46,53,66,71,72].
Notably, neither fibrinogen nor prothrombin complex concentrate (PCC) or recombinant activated factor VII (rFVIIa) are magic bullets in bleeding management and should only be given if indicated by the clinical situation and ROTEM results and in an adequate dose as a part of a bleeding management algorithm.
Thrombocytopenia as well as platelet dysfunction are frequent after cardiac surgery with CPB and have to be considered as a reason for intra- and post-operative bleeding. The expected increase in A5FIB (A10FIB, MCF) after platelet transfusion (one pooled or apheresis platelet concentrates in an adult patient) is about 8–10 mm (only about 5 mm in cirrhotic patients) (Fig. 3B) [73–75]. This can be used for dosing in our algorithm.
Since viscoelastic testing is not sensitive to the effects of antiplatelet drugs, CPB, and protamine on platelet function, POC whole blood impedance aggregometry (ROTEM platelet) is an ideal complement to thromboelastometry in cardiovascular surgery [32,46,53,76,77]. Pre-operative platelet function testing can be used to detect a residual platelet function defect in patients treated with antiplatelet drugs or other drugs that might impair platelet function in order to reduce the waiting time until surgery after cessation of ADP-receptor antagonists [78–82]. However, the intra- and post-operative changes in platelet function seem to be more significant and important for peri-operative bleeding management in patients undergoing cardiac surgery with CPB [47,60,82–85]. Accordingly, platelet function testing results achieved after protamine administration demonstrated the best correlation with postoperative chest tube drainage and postoperative transfusion requirements that were dependent on the degree of platelet inhibition and the number of pathways inhibited [47]. The corresponding cut-off values for ROTEM platelet ADPTEM and TRAPTEM after protamine administration have been implemented in our cardiovascular algorithm (Fig. 3A). Notably, several studies and one meta-analysis demonstrated that the incorporation of POC platelet function testing into transfusion management algorithms is associated with a reduction in blood loss and transfusion requirements in cardiac surgery patients [32,46,54,55,86].
The last part of the algorithm deals with impaired thrombin generation. Here, a deficiency of coagulation factors of the extrinsic pathway is detected by a CTEX > 80 s in the cardiovascular algorithm if A5FIB is normal (≥ 9 mm). Blasi et al. [87] reported that a CTEX ≥ 84 s predicted the International Normalized ratio (INR) > 1.5 in 93% of the cases, whereas a CTEX below this value predicted a safe INR value of < 1.5 in 100% of cases in patients taking acenocoumarol after elective heart valve replacement (ROC AUC = 0.998). These results have been confirmed by Schmidt et al. [88] in patients treated with warfarin. In contrast, the false-negative rate for detecting warfarin coagulopathy with kaolin- and rapid-TEG was clinically unacceptable (45.5% and 40.9%, respectively) [89]. The aim is to increase the activity of the vitamin K-dependent factors to about 40–60% that is enough to generate sufficient thrombin but avoids any overtreatment with the risk of thrombosis [48,52,71,90]. Several studies demonstrated that the approach of ROTEM-guided therapy with factor concentrates (fibrinogen and four-factor PCC)—in particular, in the cardiovascular setting—was associated with a significant risk reduction for thromboembolic events (OR [95% CI]: 0.44 [0.28–0.70]; P = 0.0006) [32–34,46,91,92]. In contrast to PCC, plasma transfusion is associated with a high incidence of TACO and right ventricular failure [7,11,93–95].
An A10 (US) version of the cardiovascular algorithm has been published in the Critical Care Handbook of the Massachusetts General Hospital [96].
In liver transplantation and visceral surgery
The liver transplantation and visceral surgery ROTEM algorithm (Fig. 3B) has a similar structure compared to the cardiovascular algorithm (Fig. 3A). Both start with the clinical detection of diffuse bleeding and the consideration of blood transfusion, followed by management of fibrinolysis, clot firmness, and thrombin generation. However, fibrinolysis management and the detection of endogenous heparin-like effects are more important in this setting [97]. SCLT in cirrhotic patients are most often characterized by thrombocytopenia and an increased INR. However, these pathologic SCLT results are not associated with increased bleeding because in this patient population a re-balance of hemostasis has to be considered. Since this re-balance take place on a low level, it can be disturbed easily and can result in bleeding as well as in thrombosis [97]. Notably, liberal transfusion of blood products—in particular, plasma— is associated with nosocomial infections, citrate intoxication, TRALI, TACO, and portal hypertension that again promotes bleeding and is associated with increased hospital mortality [98,99]. Accordingly, a restrictive transfusion strategy is associated with decreased mortality in patients with cirrhosis and upper gastrointestinal bleeding [100]. It should be avoided to treat numbers of the SCLT results. Unnecessary plasma and platelet transfusion can lead to citrate intoxication, portal hypertension, and organ failure through TACO and TRALI.
Sixty to 80% of patients undergoing liver transplantation reveal fibrinolysis—most often after reperfusion of the liver graft. However, most of them are self-limiting within 30–180 min without any need for additional treatment [101–103]. Fibrinolysis during the resection phase (pre-anhepatic phase) is associated with increased 30-day (26% vs. 0%; P = 0.000) and 6-month mortality (32% vs. 4%; P = 0.003), and fibrinolysis after reperfusion is associated with thrombosis in the portal vein and hepatic arteria (42% vs. 8%; P = 0.002) [103]. Accordingly, administration of antifibrinolytic drugs should be considered carefully—in particular, if fibrinolysis occurs after reperfusion—and no increase in blood transfusions during liver transplantation has been reported after the withdrawal of aprotinin [101–104]. Low clot firmness in EXTEM (A5EX < 25 mm) and a flat-line in FIBTEM (CTFIB > 600 s) are good predictors for fibrinolysis and can be used for risk analysis at the beginning of surgery [105,106]. Notably, FIBTEM is the most sensitive assay for fibrinolysis because in this assay diagnosis of fibrinolysis is not affected by the occurrence of platelet-mediated clot retraction [107,108].
Several observational studies reported cut-off values for EXTEM and FIBTEM clot firmness amplitudes (A5, A10, MCF) to predict bleeding and to guide fibrinogen substitution and platelet transfusion during and after liver transplantation [31,43,44,109]. With a cut-off value of 25 mm for A5EX (35 mm for A10EX and 45 mm for MCFEX) and a cut-off value of 8 mm for A5FIB (9 mm for A10FIB and 10 mm for MCFFIB), lower levels of clot firmness seem to be adequate in liver transplantation compared to the cardiovascular, trauma, and obstetric setting. Notably, FIBTEM is superior to predict bleeding in liver transplantation compared to plasma fibrinogen concentration since it does not only assess the quantity of fibrinogen but also fibrin polymerization that is affected by dysfibrinogens, factor XIII activity, and colloids [110–113]. Implementation of FIBTEM-guided fibrinogen substitution in bleeding management algorithms during liver transplantation significantly reduced transfusion requirements for red blood cells, plasma, and platelets [31,92,97,101,114–118]. In contrast, preemptive administration of fibrinogen concentrate did not influence transfusion requirements in an RCT in liver transplantation [119].
ROTEM-guided platelet transfusion during liver transplantation or in patients with cirrhosis who had to undergo invasive procedures could reduce platelet transfusion by 64 to 75% compared to transfusion trigger of platelet count < 50 × 109/L without any additional bleeding events [92,97,120–122]. This is of particular importance since platelet transfusion during liver transplantation is associated with reduced 1-year survival (74 vs. 92%; P < 0.001) [123].
INR can be used to characterize the severity of liver disease (e.g., in MELD score) but not to assess thrombin generation and bleeding risk in patients with cirrhosis [97,124–127]. Here, CTEX with a cut-off of 75 s is superior to predict bleeding in this patient population and CTEX-guidance can reduce fresh frozen plasma (FFP) transfusion and PCC administration significantly [31,97,124–129]. This helps to avoid overtreatment and thromboembolic events [92,97,125–130]. FFP is not effective in increasing thrombin generation in patients with cirrhosis but is associated with a high risk of TACO and portal hypertension [92,97,116,126,130]. In contrast to modern four-factor PCCs that contains significant amounts of protein C and S, rFVIIa does not contain any anticoagulants and has been shown to be associated with an increased incidence of thromboembolic events—in particular, arterial thrombosis—in liver transplantation and other clinical settings and should therefore be avoided [131,132].
Endogenous heparinization or a heparin-like effect (HLE) is well described in patients during liver transplantation [97,101,105,133,134]. A mild (CTIN/CTHEP-ratio ≥ 1.25) to severe (CTIN/CTHEP-ratio ≥ 2.0) HLE can be detected in about 50% after liver graft reperfusion (CTIN, 270–3312 s). The CTIN/CTHEP-ratio is more sensitive to identify HLE than APTT. Severe HLE was associated with increased transfusion requirements, and HLE during the anhepatic phase was associated with increased 3-month mortality [135]. HLE after reperfusion is most often self-limiting after hemodynamic stabilization [97,101]. If not, HLE can be reversed by small amounts of protamine [97,101,136].
Since the SURs for the assays EXTEM S, FIBTEM S, and APTEM S do not contain a heparin inhibitor, SURs must not be used in patients undergoing liver transplantation. A HLE can result in misinterpretation of ROTEM results due to prolonged CT and CFT as well as in reduced clot firmness amplitudes (A-values and MCF) by using SURs in this setting [97].
ROTEM results can also be used to assess the risk for thrombosis, and the ‘therapeutic window’ concept of ROTEM-guided bleeding management can be used to avoid thromboembolic complications [31,49,97,116,118,126,137]. Hincker et al. [137] reported that pre-operative APTT, INR, and platelet count were not able to predict post-operative thromboembolic events after major non-cardiac surgery. In contrast, INTEM and EXTEM A10 (A10EX cut-off, 61.5 mm; ROC AUC, 0.751) were the best predictors of thromboembolic complications. FIBTEM was not predictive for thromboembolic events in this study. In contrast, several studies in patients with cirrhosis and/or undergoing liver transplantation demonstrated a predictive value of increased MCFFIB (cut-off between 18 and 25 mm; risk ratio [RR] up to 4.8) for portal vein and hepatic artery thrombosis. In particular, this applies to patients with hereditary or acquired thrombophilia (e.g., anti-thrombin, protein C or protein S deficiency, factor V Leiden mutation, lupus anticoagulant, antiphospholipid antibodies) and patients with hepatocellular or cholangiocellular carcinoma [138–141]. Again, this emphasizes the need for a correct dose-adjustment and that overtreatment—also with fibrinogen—should strictly be avoided.
An A10 (US) version of the liver algorithm has been published recently in an US textbook about bleeding management [97].
In trauma and orthopedic surgery
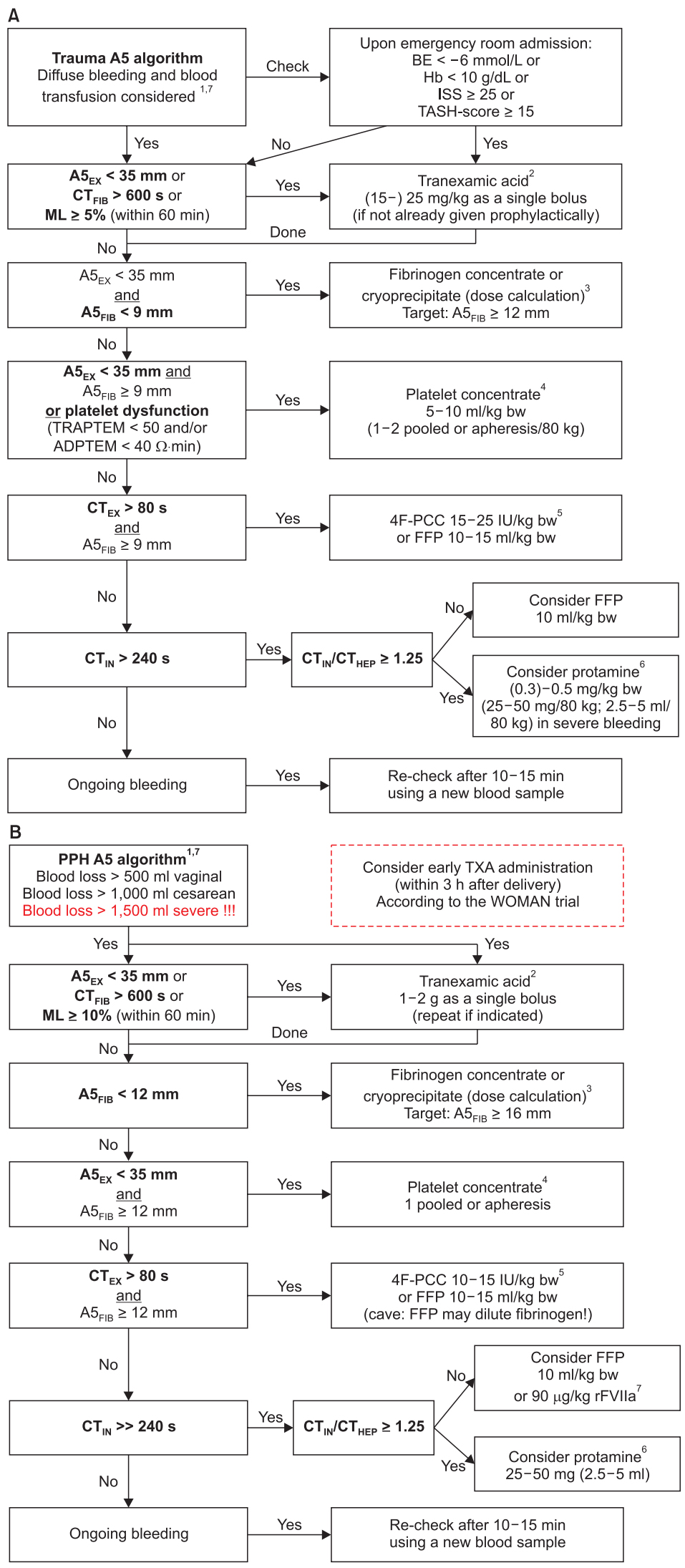
The trauma and orthopedic surgery ROTEM A5 algorithm is presented in Fig. 4A.
In trauma, a previous RCT (CRASH-2 trial) postulated that tranexamic acid (TXA) should be given to all trauma patients with significant hemorrhage within 3 h after injury, since TXA administration was associated with a RR for death of 0.91 (99% CI, 0.85–0.97) (14.5% vs. 16.0% all-cause mortality) in this study [142]. However, this study demonstrated an increase in mortality if TXA administration was started later than 3 h after injury (RR, 1.44; 95% CI, 1.12–1.84; 4.4% vs. 3.1% mortality due to bleeding) [143,144]. Accordingly, TXA should only be started later than 3 h after injury if signs of trauma-induced coagulopathy (A5EX < 35 mm or FIBTEM flat-line [CTFIB > 600 s]) or hyperfibrinolysis (EXTEM or FIBTEM maximum lysis [ML] ≥ 5% within 60 min) are present [105,145–147]. However, it is still under debate whether prophylactic or therapeutic administration of TXA should be performed in hospitals with access to viscoelastic testing [145–155]. Physiologic fibrinolysis and fibrinolysis shutdown are defined in ROTEM as an EXTEM LI60 82–97.9% and ≥ 98%, respectively [156].
Davenport et al. demonstrated that acute traumatic coagulopathy (ATC) is functionally characterized by a reduction in ROTEM clot firmness amplitude [20,36,158–160]. With a cutoff value of A5EX ≤ 35 mm, ROTEM can identify ATC at 5 min after CT and predict the need for massive transfusion (detection rate for A5EX ≤ 35 mm, 71% vs. 43% for INR > 1.2; P < 0.001). In patients with A5EX > 35 mm transfusion requirements were below 2 U RBC/12 h and 1 U FFP/12 h. For A5EX < 35 mm transfusion requirements for RBCs and FFP increase significantly. This allows for initiation and termination of massive transfusion protocols in hemorrhaging trauma patients [161,162].
In the same way Schöchl et al. [27] showed that FIBTEM (A5FIB and A10FIB) provided early prediction of massive transfusion (≥ 10 U RBCs within 24 h of admission). Here, an A10FIB < 8 mm (plasma fibrinogen level < 150 mg/dl) was associated with an increased incidence of massive transfusion. An A10FIB ≤ 4 mm (plasma fibrinogen level < 100 mg/dl) provided a ROC AUC of 0.83 for the prediction of massive transfusion. Furthermore, the crucial factor of fibrinogen for the hemostatic competence in trauma has been confirmed by Hagemo et al. [163], who detected a dramatic increase in 28-day mortality in trauma patients if admission fibrinogen concentration was below a critical value of 2.29 g/L (corresponding to an A10FIB of 12.5 mm and an A5FIB of 11.5 mm). These results have been confirmed by an international prospective validation study including 808 trauma patients [28]. An A5EX cut-off value of ≤ 37 mm had a detection rate of 66.3% for ATC. An A5EX threshold value of ≤ 40 mm predicted massive transfusion in 72.7%. An A5FIB cut-off value of ≤ 8 mm detected ATC in 67.5%, and an A5FIB cut-off value ≤ 9 mm predicted massive transfusion in 77.5%. Accordingly, an A5EX and A5FIB cut-off value of 35 mm and 9 mm have been selected for fibrinogen substitution and platelet transfusion in our trauma algorithm. The same cut-off values have been recommended by the consensus group on viscoelastic test-based transfusion guidelines for early trauma resuscitation and the German AWMF guidelines on the management of multiple traumas [164–166]. Similar cut-off values are used in the European multicenter RCT iTACTIC (implementing Treatment Algorithms for the Correction of Trauma-Induced Coagulopathy; ClinicalTrials.gov, ID: NCT02593877): A5FIB < 10 mm for fibrinogen substitution and (A5EX–A5FIB) < 30 mm for platelet transfusion [167]. This is also in line with the FIBTEM cut-off values published by Na et al. [29] to predict massive bleeding in total hip replacement arthroplasty.
Furthermore, ATC is characterized by an early platelet dysfunction mainly affecting the ADP and TRAP pathway in whole blood impedance aggregometry [168]. Chapman et al. [169] reported a cut-off value of 53 Ω∙min (ROC AUC, 0.97) for ROTEM platelet TRAPTEM and a cut-off value of 65 Ω∙min (ROC AUC, 0.88) for ROTEM platelet ADPTEM to predict massive transfusion (≥ 10 U RBCs) or death from hemorrhage within 6 h of injury. However, interventional studies are needed to assess whether early platelet dysfunction in trauma can only be used as a biomarker for severe trauma or to guide platelet transfusion in this setting [170].
Impaired thrombin generation with the need for plasma transfusion or four-factor PCC administration is considered in our trauma algorithm if CTEX > 80 s and A5FIB ≥ 9 mm according to the consensus group on viscoelastic test-based transfusion guidelines for early trauma resuscitation and the German AWMF guidelines on the management of multiple trauma [164–166]. This is also in line with the iTACTIC protocol [167]. In severe traumatic hemorrhage, fixed-ratio RBC and plasma transfusion is not effective to treat ATC and to reduce mortality [12–17,171]. Innerhofer et al. compared in their RCT the efficacy of ROTEM-guided administration of coagulation factor concentrates (fibrinogen, factor XIII, and four-factor PCC) versus plasma transfusion to treat ACT and to stop bleeding [172,173]. After two therapeutic loops, FFP failed in 52% to treat ATC and to stop bleeding and a rescue cross-over to ROTEM-guided administration of coagulation factor concentrates was needed. In contrast, ROTEM-guided administration of coagulation factor concentrates failed only in 4% and rescue cross-over to FFP transfusion was needed. Furthermore, massive transfusion rate (12% vs. 30%; P = 0.042), number of days on hemofiltration (11.0 vs. 27.0; P = 0.038), multiple organ failure rate (50% vs. 66%; P = 0.15), and venous thrombosis rate (8% vs. 18%; P = 0.22) were lower in the ROTEM-guided group. Accordingly, the European Trauma Guidelines suggest in their recommendation 33 that PCC or plasma be administered in the bleeding patient based on evidence of delayed coagulation initiation using viscoelastic monitoring provided that fibrinogen levels are normal [174].
Endogenous heparinization with a HLE detected by viscoelastic testing (CTIN/CTHEP -ratio) has been reported in 5% of patients with severe trauma and seems to be linked to endothelial glycocalyx degradation [175].
Finally, thrombosis is a big issue in trauma, orthopedics, and neurosurgery, and overtreatment should definitively be avoided by implementing the ‘therapeutic window’ concept of ROTEM-guided bleeding management. This also includes the timely start of thromboprophylaxis in the post-operative period [137,172,176–178].
An A10 (US) version of the trauma algorithm has been published recently in an US textbook about trauma induced coagulopathy [145].
In obstetrics surgery and postpartum hemorrhage
The obstetrics and postpartum hemorrhage (PPH) algorithm (Fig. 4B) is very similar to the trauma algorithm (Fig. 4A) but takes into account the shift in fibrinogen and FIBTEM reference ranges during pregnancy and the different A5FIB cut-off and target values determined for this setting in observational and interventional trials [41,42].
As mentioned earlier, the most often reason for PPH is uterine atony and placental complications (TONE and TISSUE from the 4Ts: TONE, TISSUE, TRAUMA, THROMBIN) and hemostatic interventions (plasma transfusion, platelet transfusion, coagulation factor concentrates) should only be done in case of coagulopathy [179]. Accordingly, the ISTH Scientific Subcommittees (SSC) on Women’s Health Issues in Thrombosis and Haemostasis and on disseminated intravascular coagulation (DIC) recommend that (1) ‘if POC or laboratory test of hemostasis are normal, then no FFP is required’ and (2) they ‘recommend against the use of fibrinogen concentrate in an unmonitored or pre-emptive manner’ [180]. However, every severe bleeding can result in coagulopathy, finally. Accordingly, the management of PPH is still challenging [181–183].
Notably, prepartum A5FIB and plasma fibrinogen values cannot predict PPH but FIBTEM at the beginning of PPH can predict progress of hemorrhage and transfusion requirements and can be used to guide hemostatic therapy in PPH [33,184–189]. Of course, prepartum SCLTs and ROTEM results can be helpful in patients with hereditary coagulation factor deficiencies [190]. However, hereditary issues should be known in most cases from medical history.
Hyperfibrinolysis most often occur in PPH with severe shock or in patients with amniotic fluid embolism—in the later it can be accompanied by DIC [191–194]. Nevertheless, it is recommended to give TXA early (within 3 h after labor) in patients with PPH based on the WOMAN trial (World Maternal Antifibrinolytic Trial) [144,195]. In the WOMAN trial, death from bleeding could be reduced by TXA (1.5% vs. 1.9%; P = 0.045; RR [95% CI], 0.81 [0.65–1.00]). However, all-cause mortality did not change significantly (2.3% vs. 2.6%, P = 0.16; RR [95% CI], 0.88 [0.74–1.05]) since an increase in sepsis (0.2% vs. 0.1%; P = 0.15; RR [95% CI], 1.87 [0.79–4.40]) and organ failure (0.3% vs. 0.2%; P = 0.29; RR [95% CI], 1.87 [0.75–2.53]) outweighed the reduction in mortality due to bleeding. As already reported in the CRASH-2 trial, the benefits of TXA were most prominent if administered within 3 h after delivery [144,195]. Therefore, TXA should be given as soon as possible after onset of PPH [144,195]. A continuous infusion of TXA was not anymore used in the WOMAN trial [195]. The incidence of hyperfibrinolysis in the Nigerian subpopulation and the pathomechanisms responsible for the beneficial effects of TXA in the WOMAN trial have been assessed using ROTEM and whole blood impedance aggregometry [196,197].
Quick changes in plasma fibrinogen concentration and fibrin polymerization (FIBTEM) are key issues in the development and progression of severe PPH [26,30,189,198]. Here, Collins et al. [30] showed that A5FIB (adjusted OR [95% CI], 0.85 [0.77–0.95]; P = 0.02) is superior to Clauss fibrinogen (adjusted OR [95% CI], 0.93 [0.49–1.19]; P = 0.813) to predict progression of PPH to a total blood loss of more than 2500 ml. Women progressing to 8 U blood products (RBCs + FFP + platelets) had a median (IQR) fibrinogen and A5FIB of 2.1 (1.8–3.4) g/L and 12 (7–17) mm, respectively, compared with 3.9 (3.2–4.5) g/L and 19 (17– 23) mm for those not progressing. Accordingly, the A5FIB cut-off value for our PPH algorithm was set to < 12 mm and the target to ≥ 16 mm (discriminating point in the study 17 mm). This is in line with the Liverpool algorithm published by Mallaiah et al. [185] and the recommendations from the ISTH SSC [180]. Mallaiah et al. [185,199] and Smith et al. [200,201] reported in their follow up a significant reduction in blood transfusion (P < 0.0001), large volume blood transfusion (> 5 U RBCs; 11.2% vs. 28.6%; P = 0.006), hysterectomy rate (5.6% vs. 14%; P = 0.089), TACO (0% vs. 9%; P < 0.001), and ICU admission (1.9% vs. 9%; P = 0.027). Very similar results have recently been published by Snegovskikh et al. [186]. Here again, the estimated blood loss, RBC, and FFP transfusion was significantly reduced (P < 0.001), as well as the hysterectomy rate (25.0% vs. 53.5%; P = 0.013), the ICU admission rate (3.6% vs. 43.1%; P < 0.001), and the length of hospitalization after delivery (4 vs. 5 days; P < 0.001). In contrast, preemptive treatment of PPH (estimated blood loss ≥ 1500 ml) with fibrinogen concentrate was not effective in an RCT since the mean fibrinogen concentration at randomization was 4.5 ± 1.2 g/L [202]. This is in agreement with the results of the OBS2 RCT that did not show any benefit in the subgroup administering fibrinogen concentrate if A5FIB was 13–15 mm. Only patients with an A5FIB ≤ 12 mm showed a reduction in blood loss after study drug (300 ml vs. 700 ml) and transfusion of allogeneic blood products (1.0 vs. 3.0 units) [203,204]. This again, confirmed the A5FIB cut-off and target values used in our PPH algorithm.
Impaired thrombin generation is rarely an issue in PPH but can occur due to ongoing bleeding and dilution (Fig. 5) or in case of acquired hemophilia (Fig. 6). The first issue can be treated with 4F-PCC or FFP and the second issue with rFVIIa or activated PCC administration.
Since precision individualized medicine is more and more accepted as best practice in traumatic hemorrhage and PPH, ROTEM-guided management of coagulopathy in trauma and PPH is recommended in several national and international guidelines, and some authors even postulated that coagulation POC testing should be mandatory in the trauma emergency room and on the labor ward [164–166,174,188,205–213].
Impact on Transfusion Requirements, Patient Outcomes, and Health Care Costs
Implementation of ROTEM-guided bleeding management algorithms as an essential part of PBM resulted in significant reduction in bleeding, transfusion requirements, complication rates, and hospital costs. Here, the highest evidence is available for cardiovascular surgery [32–35,45,46,54,55,66,69,214–218] but data supporting the efficacy and safety of ROTEM-guided bleeding management in other clinical settings are increasing [12,35–36,92,101,114–118,172,185,186,189,219–228]. Accordingly, Deppe et al. [34] reported in their meta-analysis including nine RCTs, eight cohort studies and 8332 patients an odds ratio (OR) of 0.63 (95% CI, 0.56–0.71; P < 0.0001) for patients receiving allogeneic blood products, 0.63 (95% CI, 0.50–0.78; P < 0.0001) for RBC transfusion, 0.31 (95% CI, 0.13–0.74; P < 0.0001) for plasma transfusion, 0.62 (95% CI, 0.42–0.92, P = 0.0292) for platelet transfusion, 0.56 (95% CI, 0.45–0.71; P < 0.00001) for re-exploration due to postoperative bleeding, 0.64 (95% CI, 0.31–1.30; P = 0.1345) for cerebrovascular events, 0.77 (95% CI, 0.61–0.98; P = 0.0278) for postoperative acute kidney injury (AKI), and 0.44 (95% CI, 0.28–0.70; P = 0.0005) for thromboembolic events. Furthermore, the Cochrane analysis published in 2016 [35] demonstrated a RR for mortality in trials using ROTEM of 0.44 (95% CI, 0.21–0.93; P = 0.03) and in studies using TEG of 0.72 (95% CI, 0.25–2.07; P = 0.54). Analyzing ROTEM- and TEG-guided studies together showed a RR for mortality of 0.52 (95% CI, 0.28–0.95; P = 0.03). The Cochrane analysis also confirmed the significant reduction in transfusion requirements and in AKI with the need for dialysis (RR, 0.46; 95% CI, 0.28–0.76; P = 0.003).
Two large multi-center cohort studies analyzing transfusion requirements and patient outcomes before and after implementing PBM—including ROTEM-guided bleeding management—recruited 129,719 and 605,046, respectively [229,230]. Here, Meybohm et al. [229] reported as their main outcome a relative reduction in mean RBC transfusion by 17% (1.05 ± 0.05 vs. 1.21 ± 0.05 units; P < 0.001) and in acute renal failure by 30% (1.67% vs. 2.39%; P < 0.001). Leahy et al. [230,231] demonstrated a reduction of RBCs, plasma, and platelets transfused per admission by 41% (P<0.001), representing cost-savings of AU$ 18,507,092 (US$ 18,078,258), corresponding to an estimated activity-based cost-savings of AU$ 80–100 million (US$ 78–97 million). Furthermore, they reported risk-adjusted reductions in hospital-acquired infections (OR, 0.79; 95% CI, 0.73–0.86; P<0.001), acute myocardial infarction/stroke (OR, 0.69; 95% CI, 0.58–0.82; P < 0.001), hospital mortality (OR, 0.72; 95% CI, 0.67–0.77; P<0.001), and length of hospital stay (incidence rate ratio, 0.85; 95% CI, 0.84–0.87; P<0.001). In summary, these large cohort studies including more than 700,000 patients confirmed that the implementation of a PBM program including ROTEM-guided bleeding management resulted in reduced blood product utilization, blood product-related cost savings, and improved patient outcomes.
In a meta-analysis assessing the efficacy of implementing a multimodal PBM program addressing each of the three PBM pillars including 17 studies comprising 235,779 surgical patients, transfusion rate was reduced by 39% (RR, 0.61; 95% CI, 055–0.68; P < 0.00001), hospital length of stay was reduced in mean by 0.45 days (95% CI, 0.25–0.65 days; P < 0.00001), total number of complications was reduced by 20% (RR, 0.80; 95% CI, 0.74–0.88; P < 0.00001), and mortality rate was reduced by 11% (RR, 0.89; 95% CI, 0.80–0.98; P = 0.02) [232].
Accordingly, European, American, and Australian perioperative bleeding management, trauma, and PBM guidelines recommend implementing PBM including POC-guided bleeding management algorithms [164,166,174,180,205–210,233]. The implementation of PBM is also supported by the Australian Government and the European Commission [234–237].
Cost-savings can be divided into transfusion-associated costs and cost-savings by reducing potentially preventable complications [33,238,239]. In a health-economic analysis including eight studies (five cohort studies, two RCTs, and one meta-analysis published between 2012 and 2017) and 755,733 patients, the mean calculated blood product acquisition cost-savings were US$ 977,703 per 1000 patients and mean calculated PPC-related cost-savings 1,786,729 per 1000 patients [240]. Here, the reported cost-savings have been highest in studies focusing on patients with a high bleeding risk [32,218] and lowest in cohort studies looking at the whole patient population of hospitals implementing PBM [229,230].