Introduction
Fascial plane blocks are techniques used to manage pain, both in the perioperative period and in the treatment of chronic pain. In recent years, different types of fascial blocks have been described and there has been an increase in their clinical applications. The main advantages offered by these techniques include the ease of performing them, the analgesic efficacy, and the low risk of complications. One of the newest techniques that have been described recently is the erector spinae plane (ESP) block. It was first described by Forero et al. [1] in 2016 for the treatment of chronic thoracic neuropathic pain and postoperative pain in thoracic surgery. Since then, many articles have been published describing the application of the technique for a wide variety of clinical scenarios. The objective of this review is to analyze the articles about ESP block that have been published to date. Through the study of these articles, we intend to describe its procedural technique, indications, effectiveness, and possible complications in the different scenarios reported.
Anatomy
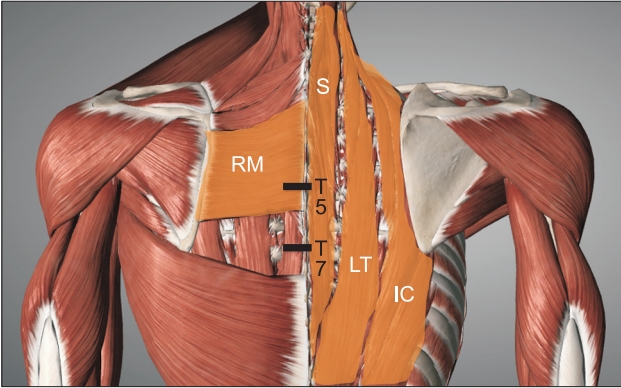
The erector spinae muscle (ESM) is a complex formed by the spinalis, longissimus thoracis, and iliocostalis muscles that run vertically in the back (Fig. 1). The ESP block is performed by depositing the local anesthetic (LA) in the fascial plane, deeper than the ESM at the tip of the transverse process of the vertebra. Hence, LA is distributed in the cranio-caudal fascial plane one dermatome a median of each 3.4 ml of injected volume [2]. Additionally, it diffuses anteriorly to the paravertebral and epidural spaces, and laterally to the intercostal space at several levels [3–5]. The LA exerts its effect on the ventral and dorsal ramus of the spinal nerve. The ventral ramus (intercostal nerve) is divided into the anterior and lateral branches. Its terminal branches provide the sensory innervation of the entire anterolateral wall. The dorsal ramus is divided into 2 terminal branches and it gives the sensory innervation to the posterior wall. Furthermore, the diffusion of LA to the paravertebral space through the costotransverse foramina and the intertransverse complex (intertransverse and costotransverse ligaments: levators, rotators, and intercostal muscles) provides both visceral and somatic analgesia. This diffusion into the epidural space and the neural foramina has been reported in anatomical studies that examined 2 to 5 vertebral levels that were centered near the injection site. However, this diffusion was not observed consistently in all cadaver studies.
Technique
The position of the patient for the realization of the block includes: sitting, lying on the side, or lying prone. The technique can be performed with the patient awake or under the effects of general anesthesia. In pediatric patients, it is advisable to perform the procedure after the induction of anesthesia. However, there is no consensus about the best method for adult patients. The awake technique provides the advantage of being able to assess the efficacy and level of analgesia by means of a skin sensitivity test. However, the poor correlation between analgesia and skin sensitivity has been reported [6].
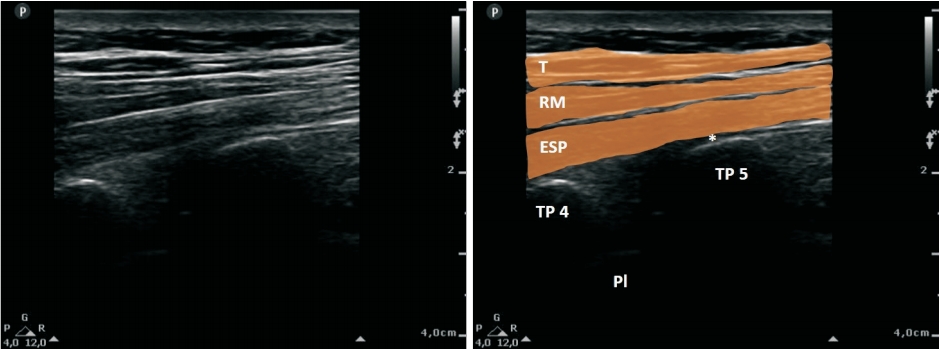
Although cases of blind puncture or under fluoroscopy have been described [7], the technique is usually guided by ultrasound. Usually, a high-frequency linear ultrasound transducer is used to block the thoracic level, and a convex transducer is used to block the lumbar level. The probe is placed in a transverse orientation to identify the spinous process. Once the level is identified, the probe is moved 3 cm laterally until the transverse process is identified. The probe should be rotated 90 degrees on the transverse process by placing it in a parasagittal plane. Three muscles must be identified as superficial to the hyperechoic transverse process shadow, and they include the trapezius, rhomboid major, and erector spinae (Fig. 2). These three muscles are visualized at the level of the fifth thoracic vertebra (standard level for a thoracic block); however, the rhomboid major muscle disappears at the level of the seventh thoracic vertebra (in lower blocks). The needle is inserted in the plane. The procedure can be performed in the cranio-caudal or opposite direction depending on the conditions and the region to be treated. Moreover, the block can be administered by a single shot or with a catheter insertion for continuous infusion; with the target as the transverse process. A hydrodissection should also be carried out with saline solution, and the local anesthetic must be deposited in the fascial plane, deeper than ESM at the tip of the transverse process of the vertebra (Fig. 3).
Materials and Methods
This is a narrative review. We performed a literature search for articles related to the ESP block in Medline, PubMed, Cochrane Library, and Google Scholar. The search period was from January 1, 2016, to December 1, 2018. The inclusion criteria were the articles related to ESP block that were identified in the search; these articles included letters to the editor, commentaries, case reports, case series, cadaver studies, observational studies, reviews, and clinical trials in adult and pediatric patients. The exclusion criteria included non-English language articles, duplicates articles, animal studies, irrelevant articles or articles that were not related to the ESP block. The search terms used included: “Erector Spinae Plane Block,” “ESP block,” and “Erector Spinae block.”
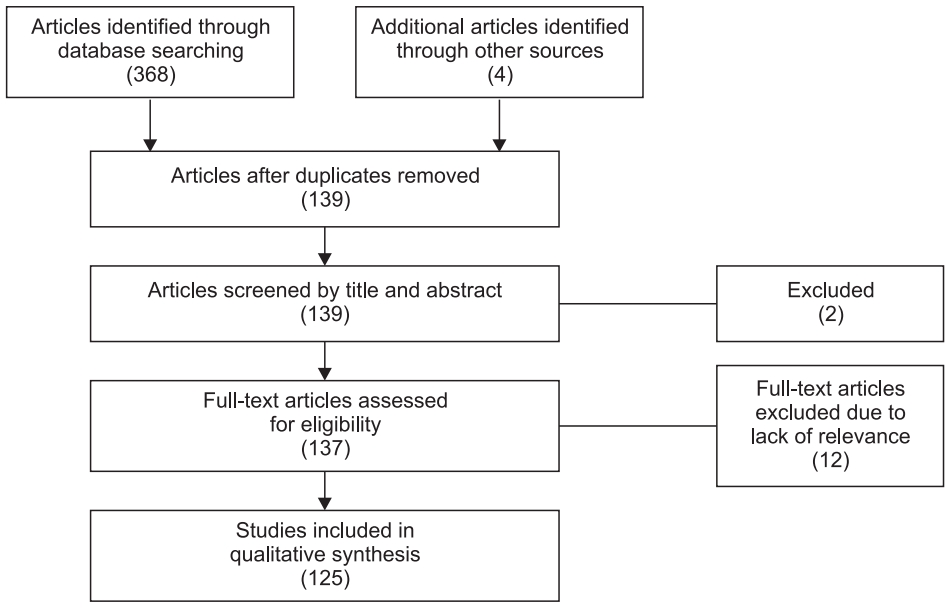
Initially, we identified 368 articles, out of which 233 articles were excluded because they were duplicates; however, 4 additional articles were identified from a different source and included in the review. Of the 139 remaining articles, 2 were excluded after reading the abstracts [126,127] which revealed that they were not related to ESP blocks. One was a review of adjuvant nerve blocks, and the other was an anatomical study of a different type of block. We eventually completed the reading of 137 articles, out of which 12 were excluded [128–139] for their irrelevance for this review. Finally, 125 studies were included in this review (Fig. 4). The data extracted in the case reports includes the following: type of pain and painful region, intervention performed, number of subjects treated, level of realization of blockage, use of catheter or single shot, unilateral or bilateral, local anesthetic used, average numerical rating scale (NRS) for pain, and presence of complications and other relevant observations. The average NRS included in the table was calculated by calculating the mean of the first NRS value reported in each case (in the cases where the pain was described in the first 12 hours post-block). The most relevant findings from clinical trials and observational studies are described in the results.
Results
The 125 articles finally included in this review included: 6 randomized controlled trials [104–109], 1 consecutive controlled before-and-after study [110], 2 observational studies [111,112], 3 review articles [2,113,121], 5 anatomical studies [3–5,124,125], 98 case reports [1,7–103], and 10 opinion articles [6,114–120,122–126]. The case reports are described in Table 1 [1,7–103]. All case reports included a total of 211 patients in 98 articles. Of these case reports, 12 and 87 articles respectively described the technique as a treatment for chronic pain and acute pain. However, both scenarios described cases where the block was utilized for therapy at the cervical level, upper limbs, thoracic level, abdominal level, and lower limbs. The single-shot technique was most frequently used, while the most commonly used local anesthetics were bupivacaine and ropivacaine. The mean NRS for analgesia measurement reported in all cases was ≤ 3, and the only complications described were incomplete analgesia, pneumothorax, and motor blockade.
Only six prospective trials were identified in this review. Tulgar et al. [104] evaluated the ESP block for postoperative analgesia in laparoscopic cholecystectomy. They compared 30 patients in two groups (ESP group and a control group). Their results included consumption of tramadol, as well as a score on the NRS scale lower in the ESP group during the first 3 h. Gürkan et al. [105] evaluated the ESP block for postoperative analgesia in breast surgery. They compared 50 patients in two groups (ESP group and control group). Total morphine consumption in block group decreased by 65% at 24 h compared to the control group (5.76 ± 3.80 mg vs. 16.60 ± 6.92 mg), but there was no statistically significant difference between the groups in terms of NRS scores. Oksuz et al. [106] also compared the bilateral ESP block with tumescent anesthesia for postoperative analgesia in 43 patients undergoing reduction mammoplasty. The NRS scores and the requirement for additional analgesia were statistically significantly lower in the ESP group. Altiparmak et al. [107] compared the effects of modified pectoral nerve (PECS) block and ESP block after radical mastectomy surgery. They concluded that PECS block reduced postoperative tramadol consumption (132.78 ± 22.44 mg vs. 196.00 ± 27.03 mg) and NRS scores after the postoperative 1 h, 2 h, 12 h, and 24 h more effectively than the ESP block. Nagaraja et al. [108] compared the continuous thoracic epidural with bilateral ESP block in cardiac surgery among 50 patients. The NRS scores were statistically significantly lower in the ESP group at 24 h, 36 h, and 48 h. Incentive spirometry, ventilator, and intensive care unit duration were comparable between the groups. Krishna et al. [109] evaluated the ESP block for postoperative analgesia in cardiac surgery. They compared 106 patients in two groups (ESP group and control group) and concluded that ESP block provided significantly better pain relief at rest (NRS were significantly lesser at all measured time points) and for a longer duration than the control group (8.98 ± 0.14 hours vs. 4.60 ± 0.12 hours).
One consecutive, patient-matched, controlled before-and-after study was included in this review. Macaire et al. [110] compared 67 patients undergoing cardiac surgery in 2 groups: a historical group of 20 patients who received intravenous morphine (0.5 mg/h) and nefopam (100 mg/24 h) with a group of 47 patients who received continuous bilateral ESP block. The ESP group was associated with less pain and lower opioid consumption (40 [25–45] mg in the control group vs. 0 [0–0] mg in the ESP group [P < 0.001]). In addition, the mobilization of the patients and the removal of the thoracic tube was performed earlier in the ESP group.
Two observational studies were identified in this review. Tulgar et al. [111] reported their results of comparing the single or bi-level application of ESP block in 12 patients undergoing thoracotomy. They observed that the NRS scores in the first 12 h were higher in the single level group than in the bi-level group. While the average fentanyl use in patients in the single level group was 37.5 mg in the first postoperative hour, no patient in the bi-level group required fentanyl. Additionally, tramadol use was lesser in patients undergoing bi-level ESP block. Ueshima et al. [112] compared 41 patients undergoing lumbar spinal surgery in a retrospective study. They observed that the NRS scores and the amount of fentanyl administered were lower in the ESP block group than in the control group at all measured time points, with no significant difference in the incidence of complications between the two groups. The 9 studies described are summarized in Table 2.
Discussion
Regional anesthesia and pain management have experienced advances in recent years with the advent of fascial plane blockages. One of the newest techniques described in the literature has been the ESP block. In the past two years, the publications referring to ESP block have increased significantly [113,114].
Furthermore, most published articles are case reports; hence, from the study of these reports, it can be concluded that the ESP block is an effective analgesic technique in a variety of clinical scenarios. It can be utilized successfully in the treatment of acute and chronic pain. Likewise, it has also been effective for analgesia at the cervical, thoracic, and abdominal levels. Likewise, studies indicate that it can provide adequate analgesia in the upper or lower limbs if it is performed at the high thoracic and lumbar levels, respectively. The procedure has mostly been described for postoperative analgesia at the thoracic level. Additionally, it has a low rate of reported complications. However, given the majority of case reports reported in this review, the evidence of the description is low and there is a risk of publication bias (since it is possible that the studies with unsuccessful blockade were not published). Another limitation of our review is the lack of prospective studies. Prospective randomized controlled trials that compared the technique with a control group revealed that the ESP technique reduces both the pain scale score and the need for additional analgesia. However, other studies that compared the ESP block with another technique were not unanimous in their favor of it. The difference in analgesic effectiveness, which differs according to the scenario and comparative technique, means that more prospective studies are needed to help improve the evidence of its use.
Most authors affirm that ESP block is a technique that has great advantages over conventional techniques performed close to the neuroaxis. First, it is an easy technique to perform as the visualization of the target by ultrasound is very simple and it is not difficult to direct the needle towards it. Second, the technique has a low risk of complications. Important structures (such as main vessels, pleura, or medulla) whose injury can cause serious complications, are far from the target of blockage. Although several authors have postulated that the ESP block is the same technique as the retrolaminar block [117,118] or an “accidental paravertebral block” [119,120], both clinical and anatomical studies (in vivo and cadaveric) seem to indicate that it is a different technique [3,121,124,125]. Moreover, it is performed differently, the objective is different in all cases and the diffusion of LA differs between them.
Given that this procedure is easy to perform and is relatively safe, several authors have expressed the opinion that it could be part of the multimodal analgesia of the enhanced recovery after surgery programs [110]. Additionally, catheter insertion has been described as an easy procedure to perform; hence, the possibility of performing the technique for prolonged analgesia is available. However, being such a novel blockade technique, the lack of more well-designed prospective studies makes recommending its use in these programs has not yet occurred.
Therefore, we can conclude that ESP block seems to be an effective analgesic technique at many levels. This offers us the opportunity to utilize it in many clinical situations. Although it is not the technique of first choice in most situations, it is a suitable alternative, especially in scenarios in which the technique of first choice constitutes an important risk or is directly contraindicated. Moreover, ESP block has been described as an effective alternative when paravertebral or epidural block are contraindicated due to rejection by the patient [33,45,56,83], thrombocytopenia [39,41], antiplatelet [52] or anticoagulant treatments [53], or coagulopathy [58]. Other authors have shown its effectiveness as a second line therapy after the unsuccessful insertion of an epidural catheter [41] or its failure [49,51]. Additionally, it has been reported to successfully induce anesthesia in patients with a high risk of adverse effects from general anesthesia [30,31,85,86,99]. However, more randomized controlled trials are necessary to establish the best indications of ESP block as an analgesic technique, in chronic, acute, and postoperative pain.