Postdural puncture headache (PDPH) is a benign condition and the most frequent complication of spinal anesthesia. Intracranial subdural hematoma is an extremely rare but lethal complication of spinal anesthesia. Although spinal anesthesia is a safe and common intervention, an increasing number of papers are reporting cases of intracranial hematoma after spinal anesthesia. Headache is generally the first symptom of subdural hematoma; however, headache after spinal anesthesia is almost always considered to be caused by PDPH. More than 50 cases, including those in the present report, on the development of subdural hematoma after spinal anesthesia have been published [1,2,3,4,5,6,7,8,9]. We herein present two cases of bilateral subdural hematoma after epidural anesthesia. This paper emphasizes the importance of close follow-up of patients with PDPH and consideration of the various differential diagnoses of headache after spinal anesthesia.
Case Reports
Case 1
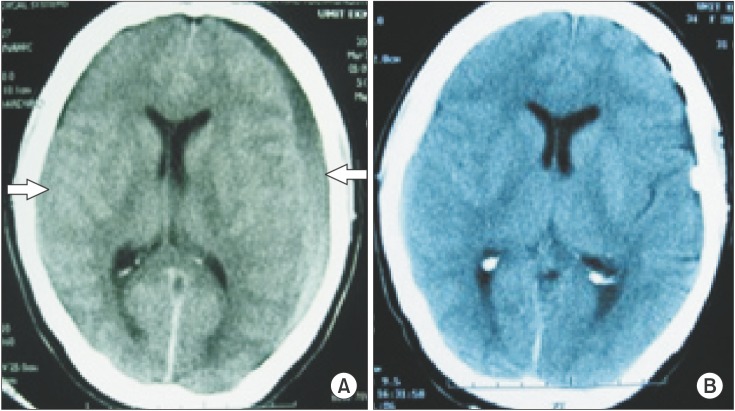
A 34-year-old female was admitted to the hospital with 10-day postpartum severe headache, vomiting, and facial asymmetry. Epidural anesthesia had been attempted at another hospital for caesarean section, but the intervention was unsuccessful. Therefore, general anesthesia was administered (primigravida at 39 weeks of gestation). The headache had started on the first postpartum day and became progressively incapacitating and unresponsive to medical treatment. The headache was not postural. The patient had no history of trauma or bleeding disorders. She was discharged with recommendations to undergo bed rest and analgesics. The facial asymmetry started 12 h before admission. No details of the anesthesia or labor were available. Neurological examination revealed right central facial paralysis and a bilateral positive Babinski sign. Emergent cranial computed tomography (CT) showed a bilateral frontoparietal acute-subacute subdural hematoma with a thickness of 12 mm on the left and 3 mm on the right side (Fig. 1A). The left side was drained through a burr hole under general anesthesia. The perioperative course was uneventful, and the patient was discharged 5 days postoperatively in a normal neurological state (Fig. 1B).
Case 2
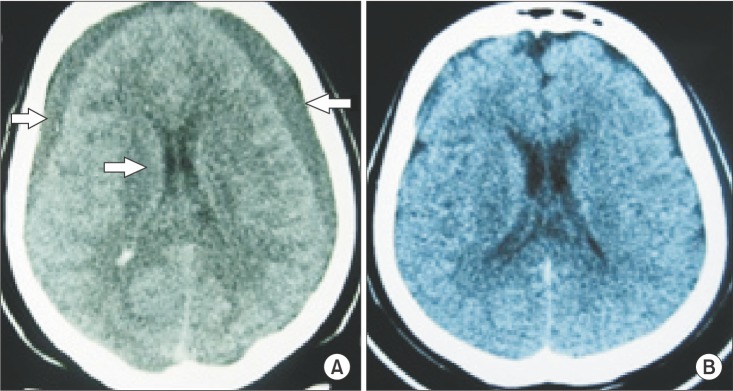
A 59-year-old female was admitted to the hospital with complaints of headache and vomiting. The patient had undergone hip prosthesis placement 20 days previously in another hospital. She had undergone general anesthesia after an unsuccessful attempt at epidural anesthesia. The headache had begun 10 days previously, and the patient had been vomiting for 3 days. She had no history of trauma or bleeding disorders, but enoxaparin was administered at 100 mg/day for 3 days postoperatively. Her fronto-occipital headache was not postural, and her neurological examination findings were normal. Cranial CT showed a 15-mm-thick bilateral frontoparietal chronic subdural hematoma compressing the brain (Fig. 2A). The patient underwent general anesthesia for surgical treatment on the same day. The hematomas were drained through bilateral burr holes. The perioperative course was uneventful. She was discharged 8 days postoperatively in a normal neurological state (Fig. 2B).
Discussion
The major etiologies of subdural hematoma are head trauma, coagulation disorders, certain medications, iatrogenic causes, dehydration, and lumbar puncture [2]. Subdural hematoma after spinal or epidural anesthesia is a very rare but lethal complication of spinal anesthesia.
The same mechanisms have been accepted for both PDPH and postdural puncture subdural hematoma (PDPSH) [4]. Cerebrospinal fluid (CSF) leakage causes a reduction in the intraspinal and intracranial pressure. These alterations result in caudal displacement of the brain and stretching of pain-sensitive structures and bridging veins [9].
PDPH is the most frequent and benign complication of spinal anesthesia. Headache is the most common symptom of both PDPH and PDPSH. This common feature usually delays or masks the diagnosis of PDPSH, potentially resulting in morbidity or mortality. Patients with headache must therefore be examined carefully. Headache after spinal anesthesia is almost always postural and located in the frontal or occipital region. Relief of the pain after a few days of bed rest is typical for PDPH. However, nonpostural headache and vomiting are warning signs in most patients with subdural hematoma [9]. Headache secondary to subdural hematoma is caused by an increase in intracranial pressure. Pre-eclamptic headache, subarachnoid hemorrhage, migraine, meningitis, tumor, and cerebral venous thrombosis should also be kept in mind as differential diagnosis of PDPH. The delayed diagnosis in most previously reported cases indicates that none of the above-listed pathologies, including PDPSH, were taken into consideration as a potential cause of the headache [1,9]. Central facial paralysis in the first patient and prolonged and severe headache in the second patient were the reasons for the investigations. Physicians should be alert to the development of any focal signs, disorientation, convulsions, or nonpostural, prolonged headaches, such as those in the present cases.
Most previously reported cases of PDPSH were unilateral; however, both of our cases involved bilateral subdural hematomas. This finding may be attributable to the greater loss of CSF, which is caused by the use of larger needles in epidural anesthesia. Zeidan and Baraka [10] made a similar comment on this issue as some of the patients in his review also developed bilateral hematomas.
CT is a safe, easy, and low-cost method of detecting subdural hematomas. Patients with severe, prolonged, or atypical headaches must first be examined with CT to avoid catastrophic results [4,5].
The administration of enoxaparin may have been a factor in the development of the subdural hematoma in the second patient in this report. The widespread use of low-molecular-weight heparin in orthopedic surgery may increase the risk of intracranial hemorrhage after spinal anesthesia [11]. Unintentional dural puncture during induction of epidural anesthesia was the cause of the subdural hematoma in both of the present cases. Accidental dural puncture is a well known cause of acute, subacute, and chronic subdural hematoma [3,12,13]. Larger needles are usually preferred in epidural anesthesia. In nearly half of the cases reported in the literature, unintentional dural puncture following epidural anesthesia was the cause of PDPSH [9].
The diameters of the needles used in the present cases are unknown. The risk of PDPSH can be decreased by using small needles because the extent of leakage is directly related to the size of the needle [6,8,9]. Some authors believe that blood patching is an effective method of blocking CSF leakage [14]. The success rate of blood patching in patients with PDPH is 60 to 90% [3]. However, recent studies have shown that the probability of success depends on the timing of the patch. Better results are achieved if the blood patch is performed 72 h after dural puncture [7].
Subdural hygromas or hematomas may resolve spontaneously. The true incidence of PDPSH is unknown because most affected patients are probably managed without further investigation. Therefore, the true incidence of PDPSH may be greater than stated in previous reports. The management of subdural hematoma is either conservative or surgical. Surgery should be performed if neurological impairment or significant brain compression is present. Hematomas of <5 mm usually resolve spontaneously; therefore, close clinical observation is the best choice [3,7]. Surgical treatment was performed in the present cases, and very good clinical and radiological outcomes were achieved.
Although PDPSH is very rare, physicians must keep this condition in mind to prevent catastrophic results after spinal anesthesia. CT is the most effective and easiest way to rule out intracranial complications in patients with postdural puncture headache.