Regurgitation immediately after valve replacement surgery is not an unusual complication. It is caused mostly by an incomplete disc closure with the use of a mechanical valve, or by paravalvular leakage. Rarely, it can be caused from injury of the prosthesis during surgery, which is prone to happen in patients undergoing concomitant surgery or having an unfavorable anatomy. We experienced a case of prosthetic injury in a patient who underwent aortic valve replacement and septal myectomy with concomitant coronary artery bypass graft (CABG) surgery.
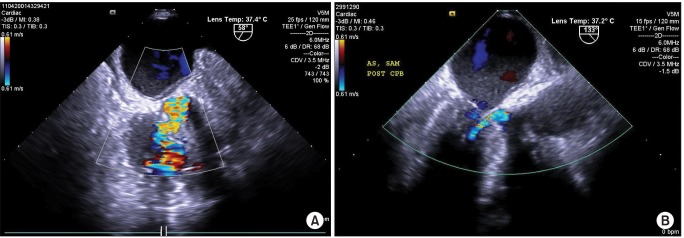
A 68-year-old woman who was diagnosed with severe aortic stenosis and coronary artery disease combined with asymmetrical left ventricular (LV) basal wall hypertrophy (maximal diameter at systolic phase: 20 mm) was referred to us for surgery. The operation was performed through the median sternotomy under standard general anesthesia. After accomplishing a conventional cardiopulmonary bypass (CPB) and aortic cross clamping, a transverse aortotomy was made just above the sinus of the Valsalva. Additionally, the removal of the calcified aortic valve leaflets and resection of the LV septal muscle were performed. A 19 mm Epic supra annular tissue valve (St. Jude Medical, Inc., St. Paul, MN, USA) was chosen, but the patient's aortic annulus and root were so narrow and rigid that aortic root enlargement had to be performed for the implantation of the prosthesis. After closure of the aortotomy, CABG surgery was performed by anastomosing the saphenous vein graft from the ascending aorta to the right coronary artery and the internal mammary artery to the left anterior descending artery. After weaning the patient off CPB, the transesophageal echocardiography (TEE) revealed a ventricular septal defect (VSD) on the mid-esophageal right ventricular (RV) inflow-outflow view (Fig. 1A). The VSD was membranous in location, 6-7 mm beneath the prosthetic aortic valve, and measured 5-6 mm in diameter. The CPB was reinstituted, and patch repair of the VSD was performed through a right atriotomy. At the end of the second CPB, no VSD was evident, but a newly appeared periprosthetic regurgitant was seen on the TEE (Fig. 1B). The color-flow Doppler showed a high-velocity, eccentric turbulent regurgitant jet, suggesting pathological leakage. We recommended against proceeding with the surgery since the leakage occurred to a mild extent and further prolongation of the CPB time might have been excessively harmful to the patient. The total CPB time was 4 hr 37 min. She was transported to the intensive care unit, receiving norepinephrine and vasopressin. She progressively deteriorated, resulting in multiorgan failure, and expired the day after the surgery.
One of the common causes of pathological regurgitation through a prosthetic valve that can be seen immediately after surgery is a paravalvular regurgitation. Its origin is typically outside the sewing ring, but in this case, the origin of the leakage was within the orifice of the sewing ring. Another common cause is an incomplete disc closure of the mechanical valve, but a bioprosthetic valve, as used in this case, rarely causes valve dysfunction early after the surgery [1]. In this case, prosthetic valve insufficiency occurred due to injury from the repeated manual manipulations of the prosthesis. Because of her small aortic annulus, the prosthesis was implanted very tightly and with difficulty, even though aortic root enlargement preceded the procedure. In addition, septal myectomy is a technically challenging cardiac operation, because of the limited exposure of the septal bulge through the aortotomy view, leading to many complications including inadvertent injury to the aortic valve leaflet [2,3]. We detected the VSD following the myectomy, and a repair surgery was performed. The additional procedure caused the CPB time to be prolonged, which leads to deterioration in the vast majority of cardiac surgeries [4]. In addition, a surgery that is performed in the vicinity of the aortic valve, such as repair of the VSD, also involves the risk of inadvertent injury to the aortic valve, resulting in leaflet perforation with regurgitation [3].
This case report provides cautions for the potential risks of performing multiple concomitant surgical procedures in patients with complicated diseases or an unfavorable anatomy. For those patients, adequate preventive procedures to eliminate intraoperative complications have to be considered before the surgery. Moreover, a more careful assessment of valvular lesions, periprosthetic leakage, and other complications of surgery by intraoperative TEE is mandatory.