Introduction
The endothelium is crucial to the maintenance of vascular physiology and the coagulation system. If the vessels are injured and the integrity of the endothelium is lost, platelet is exposed to the subendothelial collagen matrix, a potent platelet agonist, and become activated [1]. Although this platelet activation is basically a protective mechanism to stop bleeding, it may cause undesired consequences. The activated platelet may initiate the coagulation cascade and release potent vasoconstrictors. Consequently, tissue damage may be increased.
During coronary artery bypass graft (CABG), damage to the endothelium is difficult to avoid [2], and platelet activation in the coronary artery or graft vessels may cause fatal complication. Thus, aspirin is administered to prevent platelet activation during CABG and aspirin administration in early postoperative period is proven to reduce the morbidity and mortality in CABG patients [3]. However, 5% to 45% of the population is resistant to aspirin [4,5]. Moreover even in non resistant patients, aspirin inhibits only the thromboxane A2 (TxA2)-dependent platelet-activating pathway [6], and the other platelet-activating mechanism can still be activated.
We hypothesized that the variance of preoperative platelet response to collagen in patients who take aspirin might be associated with platelet activation and consequently modulates the myocardial injury during CABG. Therefore, we measured whole-blood aggregometry (WBA) with collagen preoperatively in off-pump CABG patients taking aspirin, to assess the relationship with the postoperative myocardial injuries.
Materials and Methods
Patients
This study was approved by our institutional ethics committee, and written informed consents were obtained from all patients. We enrolled adult patients who were scheduled for elective off-pump CABG and who had taken 100 mg of aspirin (Bayer Healthcare, Leverkusen, Germany) a day for more than a month. The exclusion criteria were the presence of another additional cardiac disease, such as valvular disease, requiring surgical treatment prior to heart surgery, known coagulation disorders, thrombocytopenia (<150 ├Ś 109/L), low-molecular-weight heparin (LMWH) treatment less than 10 days before surgery, or any antiplatelet therapy other than aspirin. Patients with uncontrolled hypertension, alcoholism, heavy smoking, psychiatric illness, renal disease (Cr > 177 ┬Ąmol/L), or active liver disease were also excluded.
Treatment and surgical procedures
The preoperative aspirin medication (100 mg a day in the morning) was continued until two day before surgery. From postoperative day 1, the patients were recommended to take aspirin.
For all the patients, anesthetic and surgical techniques were standardized. Anesthesia was induced with midazolam, etomidate, and sufentanil, and maintained with midazolam, sufentanil, and vecuronium by continuous intravenous infusion. During operation, intravenous fluids and dobutamine were titrated to maintain cardiac index and mean arterial pressure at a minimum of 2.2 L/min/m2 and 65 mmHg, respectively. If hypotension developed with adequate cardiac index and pulmonary capillary wedge pressure (>10 mmHg), intravenous norephinephrine (0.05 ┬Ąg/kg/min to 0.2 ┬Ąg/kg/min) was administered.
After the pericardium was opened, heparin was administered at a dose of 300 unit/kg, and an activated coagulation time (ACT) greater than 300 s was maintained with supplementary doses of heparin until the completion of anastomoses. The surgical technique for CABG was the off-pump technique with a stabilizer (Octopus®2+ Tissue Stabilization System, Medtronic Inc., Minneapolis, MN, USA) and an intracoronary shunt. After the completion of revascularizaton, the heparin effect was not reversed with protamine sulfate. For all the patients in our study with intraoperative bleeding, a cell separator (Cobe BRAT 2, Cobe Cardiovascular Inc., Arvada, CO, USA) was used to concentrate the lost blood, and this blood was reinfused. All patients had mediastinal and pleural drains.
Whole-blood impedance aggregometry (WBA) for evaluation of platelet aggregation
Platelet aggregation was studied in the presence of two different doses of collagen (2 ┬Ąg/ml or 5 ┬Ąg/ml) as stimulatory agents with the impedance method using whole-blood aggregometry (Chrono-Log 592, Chrono-Log Corp., Havertown, PA, USA). One day before surgery, blood samples were collected by sterile venipuncture from the antecubital fossa using a 21-gauge butterfly needle. Samples were transferred into polypropylene tubes containing 0.5 ml of 3.2% (w/v) sodium citrate. Measurements of whole-blood platelet aggregation were made according to the Chrono-Log protocol [7]. Briefly, whole blood diluted 1 : 1 with 0.85% (w/v) saline was incubated with the appropriate antagonist, then supplemented with collagen (2 ┬Ąg/ml or 5 ┬Ąg/ml). The impedance value reflecting the extent of platelet aggregation was read after 6 min. The patients who showed the WBA values in upper 30% were defined as high response group and the other lower 70% patients were defined as low response group.
Cardiac enzymes
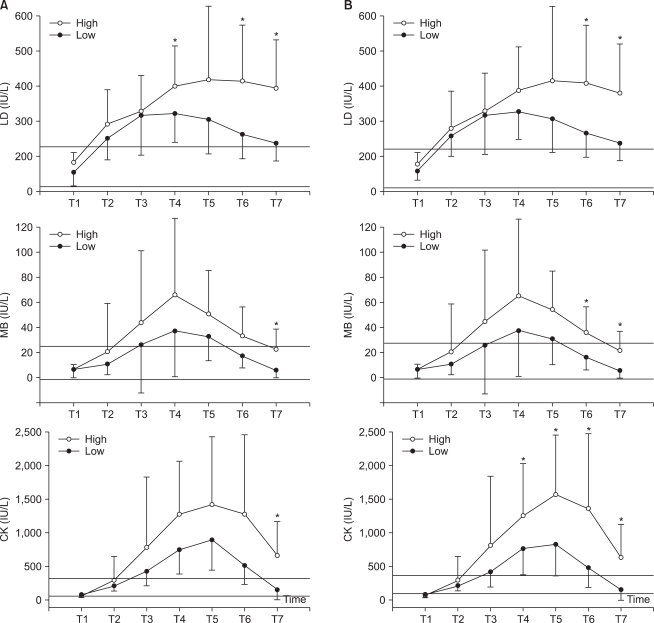
Blood was sampled for the measurement of creatine kinase (CK, reference range 20-270 IU/L), creatine kinase-MB (CK-MB, reference range 0-24 IU/L), and lactate dehydrogenase (LD, reference range 100-225 IU/L) immediately before surgical incision (T1), at the end of the operation (T2), 6 hours (T3), 1 (T4), 2 (T5), 3 (T6), and 5 days (T7) after the operation.
Electrocardiograms
Twelve-lead electrocardiograms were obtained at the end of the operation, 1, 2, 3, and 5 days after the operation. All electrocardiograms were read and agreed upon by two cardiologists blinded to the patient's clinical course and cardiac enzyme concentrations. Cardiac events measured by electrocardiographic criteria were classified as one of the following: (1) persistent new Q waves (Ōēź40 ms) occurring in at least two leads; (2) persistent new R waves (Ōēź40/50 ms) occurring in V1/V2, in more than two leads; and (3) new-onset complete bundle branch block.
Postoperative bleeding
Chest tube outputs were assessed at 8 and 24 hours after surgery to measure postoperative bleeding. The chest tube outputs were calculated from the contents in the water-seal chest drainage system.
Statistical analysis
Continuous variables are presented as means ┬▒ SD. Categorical variables are presented as frequencies and percentages. Unpaired t or Rank Sum test (if not normally distributed) were used to compare the demographic, clinical variables and the postoperative parameters (cardiac enzymes) at each time point between the 2 groups. The correlation between variables was assessed by Pearson's correlation. A P value of < 0.05 was considered statistically significant. In our pilot study, LD level of low response group was 250 ┬▒ 53 IU/L in 2 ┬Ąg/ml and 265 ┬▒ 58 IU/L in 5 ┬Ąg/ml at postoperative 3 day. We expected 50% increase of LD in high response group. A sample size of at least 5 patients was needed in both 2 ┬Ąg/ml and 5 ┬Ąg/ml group, to obtain a power of 0.8 with two sided alpha value of less than 0.05. Analyses were performed using SigmaStat ver.3.1 (Systat Software Inc., Chicago, IL, USA) and SPSS ver.12.0 (SPSS Inc., Chicago, IL, USA).
Results
Clinical characteristics
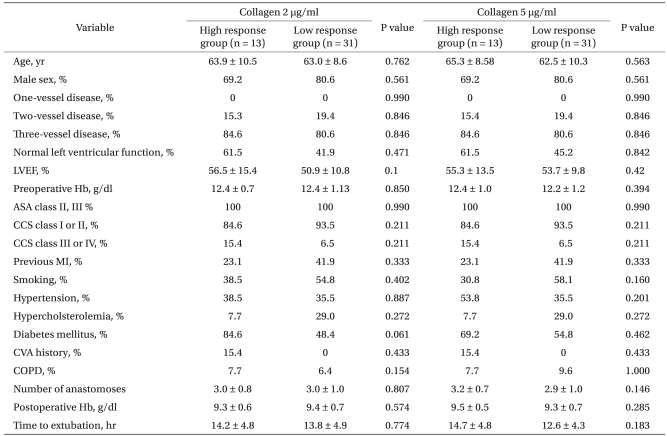
Forty-four patients were enrolled in this study and completed the trial. No deaths or serious adverse events were reported over the treatment period. Demographic and clinical characteristics of high and low respond groups for 2 and 5 ┬Ąg/ml collagen WBA are shown in Table 1. Among 44 patients, 13 and the other 31 patients were classified as high and low response groups respectively.
Whole-blood impedance aggregometry for platelet aggregation
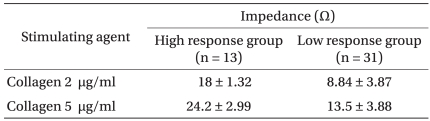
The platelet aggregation data are presented in Table 2.
Cardiac enzymes
High response group on low dose (2 ┬Ąg/ml) collagen WBA showed higher LD on postoperative 1, 3 and 5 days (P values = 0.012, <0.001 and <0.001 respectively), CK on postoperative 1, 5 days (P values = 0.027 and 0.009 respectively) and CK-MB on postoperative 5 day (P value = 0.004) than low response group. High response group on high dose (5 ┬Ąg/ml) collagen WBA also showed higher LD (postoperative 3 and 5 days with P values of 0.004 and 0.002 respectively), CK (postoperative 1, 2, 3 and 5 days with P values of 0.027, 0.007, 0.005 and 0.001 respectively) and CK-MB (postoperative 2, 3 and 5 days with P values of 0.019, 0.001 and <0.001) than low response group. On high dose collagen WBA, there was no difference between low and high response groups on preoperative cardiac enzyme levels. However, on low dose collagen aggregometry, high response group showed higher LD and CK levels (P values = 0.009 and 0.028 respectively) (Fig. 1) than low response group.
Correlation between variables
Fig. 2 illustrates the relationship between CK-MB, CK and LD at 3 day after operation. A significant correlation was found only between CK-MB and CK (r = 0.699, P < 0.001).
Postoperative bleeding
There was no significant difference on postoperative bleeding between two groups (Table 3).
Discussion
This study shows that high response to collagen on preoperative WBA is associated with increased perioperative myocardial injury in the patients undergoing off-pump CABG even if they take aspirin.
The clinical importance of endothelial damage during CABG is well known, and measures are taken to prevent endothelial damage. However, even when the 'no-touch technique' is used, injury to the endothelium is difficult to avoid [2]. Damaged endothelium exposes the subendothelial collagen, a platelet agonist, and activated platelet generates microemboli, which may be an important mechanism of myocardial injury [8]. In addition, during carotid endarterectomy, preoperative platelet aggregation induced with collagen was significantly higher in patients with more microemboli on intraoperative transcranial doppler monitoring [9]. The other studies have stressed that coronary spasm induced by TxA2 released from activated platelet is an important mechanism underlying the myocardial injury caused by activated platelet [10,11].
Aspirin inhibits platelet cyclooxygenase (COX)-1, which converts arachidonic acid to TxA2 [4,12]. TxA2 activates the platelet TxA2 receptor. Thus, aspirin activity is usually reflected in the platelet response to arachidonic acid. In addition, the aspirin effect can also be detected using low and high dose collagen WBA. In low dose collagen WBA, only normal platelets aggregate, whereas in high dose collagen WBA, both normal and aspirin-inhibited platelets aggregate [13]. In this study, both low and high dose of collagens were used as platelet agonists. The result that high responders on low dose WBA showed higher myocardial injuries can be explained by aspirin resistance. However, considering the previously reported rate of aspirin resistance [14], the number of patients in our study is not sufficient to cause the difference between groups on low dose collagen WBA by the aspirin resistance alone. Moreover, there were differences on the preoperative myocardial enzyme levels between low and high responders on low dose collagen WBA (Fig. 1). Therefore in this study the results by low dose collagen aggregometry might be influenced by not only aspirin resistance but also the difference of the preoperative disease activity expressed on both baseline myocardial enzyme and low dose collagen aggregometry.
The preoperative variance of high dose WBA values in our study could have reflected a polymorphism in platelets or been related to the variously activated state of the platelets. Either way, this study showed that the preoperative variations in the platelet response to collagen correlated with postoperative myocardial injury during CABG. Consequently, it stresses the importance of collagen-mediated platelet activation on myocardial injury during CABG and suggests the potential role of blocking the receptor for protective strategy. Although several receptors have been proposed as platelet collagen receptors, glycoprotein VI (GPVI) has recently received considerable attention. Mouse or human platelets in which GPVI has been pharmacologically blocked or immunodeleted are unresponsive to collagen [15]. Collagen signaling is conferred by the expression of GPVI in hematopoietic cell lines that express its coreceptor FcRg [16]. This suggests that GPVI signaling is both necessary and sufficient for the activation of platelets by collagen under conditions of abundant receptors and ligands. Studies with mice have shown that GPVI-deficient mice display a nearly complete abolition of the platelet response to endothelial injury [17].
Moreover, GPVI-deficient mice do not exhibit an overt bleeding phenotype and that GPVI-deficient humans show only minor bleeding diatheses rather than major bleeding phenotypes. This is consistent with the observation in this study that collagen WBA only correlated with myocardial injury and not with blood loss after CABG. Considering the preoperative use of platelet inhibitors, such as aspirin, may increase postoperative bleeding, potential importance of collagen receptor block during CABG is more stressed.
In conclusion, this study demonstrates that even in patients taking aspirin who undergo off-pump CABG, the preoperative platelet response to collagen correlates with postoperative myocardial injury. This emphasizes the importance of collagen-mediated platelet activation during CABG.