Epidural analgesia with local anesthetics and opioids has been widely used after total hip arthroplasty for postoperative pain relief [1]. However, studies have suggested that the benefits of epidural analgesia must be reconsidered against its potential adverse effects such as urinary retention, hypotension, pruritus, nausea, and motor block that delays mobilization [2]. The lumbar plexus block (LPB) may be considered as an alternative to epidural or systemic analgesics for pain control after hip surgery. However, this block is technically difficult to perform, even with ultrasound guidance [3]. Moreover, the LPB carries a risk of serious complications, including direct nerve injury, motor blockade, total spinal anesthesia, and diffusion of local anesthetic into the epidural space, causing a loss of sympathetic tone and subsequent hemodynamic instability [3].
Recently, the quadratus lumborum block (QLB) was reported as a suitable option for analgesia after abdominal surgery. The QLB utilizes a simple and easy fascial plane technique, rather than a perineural technique, and can provide a wide area of sensory blockade from T4–8 to L3 [4,5]. Compared with the LPB, the QLB is easier to perform and is associated with a lower risk of direct nerve injury and epidural spread. Here we report a case involving an elderly man in whom a continuous transmuscular QLB provided highly effective analgesia after total hip arthroplasty.
Case Report
An 83-year-old man weighing 64 kg presented with loosened hip screws one year after proximal femoral nail antirotation. Hardware removal and right-sided total hip arthroplasty were planned, and the patient provided written informed consent for the use of a QLB and publication of this report, which was approved by the Institutional Review Board of The Catholic University of Korea, Daejeon St. Mary’s Hospital (DC17ZESI0092). The patient had a history of hypertension and benign prostatic hypertrophy, both of which were well controlled by medication. He had previously undergone kyphoplasty for a compression fracture in the L1 vertebra. Otherwise, his history assessment and preoperative evaluation were unremarkable.
In the operating room, after standard monitoring was implemented, fentanyl 50 µg and midazolam 1 mg were intravenously administered for sedation and analgesia. The patient was then placed in a left lateral decubitus position, and epidural anesthesia was induced at the level of the L4–L5 interspace using the median approach with an 18-gauge Tuohy epidural needle. Loss of resistance to 1 ml of normal saline was achieved on the first attempt, and a test dose comprised of 1% mepivacaine 3 ml and epinephrine 15 g was administered, followed by a bolus comprised of 0.5% ropivacaine 13 ml and fentanyl 50 µg.
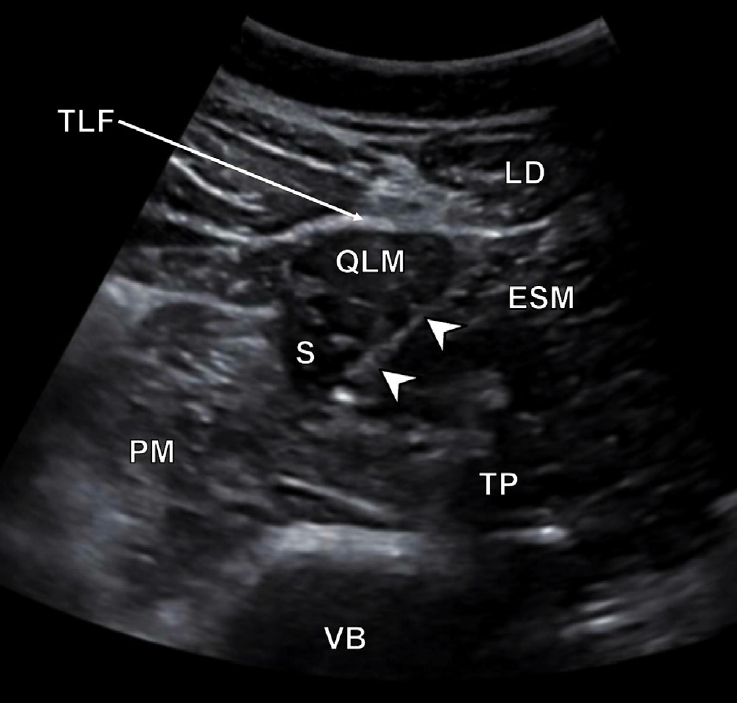
Following the epidural procedure, a transmuscular QLB was performed under ultrasound guidance following an acute pain service protocol. Subsequent to the placement of a 2- to 7-MHz curved ultrasound probe over the midaxillary line, the external oblique, internal oblique, and transversus abdominis muscles were identified along with the transversus abdominis aponeurosis. The probe was moved to trace the muscles (quadratus lumborum [QL], psoas major, and erector spinae) in the anterior to posterior direction using the shamrock sign. After skin infiltration with 1% mepivacaine 2 ml, an 18-gauge, 90 mm Tuohy needle attached to intravenous extension tubing between the needle and syringe was inserted in the posterior to anterior direction. The needle was aimed between the QL and psoas major muscles (Fig. 1). After confirmation of the needle position via injection of 2 ml of saline, a 19-gauge epidural catheter was inserted 2 cm through the epidural needle under real-time ultrasound guidance (Fig. 2). Accurate catheter placement was confirmed by Doppler ultrasonography. Following catheter placement, the patient was returned to the supine position, and his condition was confirmed to be stable before proceeding with surgery.
The patient was intraoperatively sedated by continuous propofol infusion. His vital signs remained stable during surgery, which was completed uneventfully. No additional analgesics were required. The total operation time was 3 h and 30 min. At the end of surgery, the patient received intravenous ketorolac 30 mg and ramosetron 0.3 mg; 25 ml of a prepared mixture of 0.2% ropivacaine and 5 µg/ml of epinephrine was injected though the indwelling catheter.
The multimodal postoperative analgesia regimen included oral medication, intravenous analgesia, and regional anesthesia, with rescue analgesics available on demand. This regimen was in accordance with the acute pain service protocol at our hospital. The patient was prescribed oral celecoxib 200 mg twice daily for seven days. The 0.2% ropivacaine and epinephrine mixture was continuously infused at a rate of 8 ml/h through the indwelling catheter, using a patient-controlled analgesia (PCA) pump (Hospira GemStar® Pump, Hospira Inc., USA). Intravenous fentanyl was also provided using a second PCA pump (Hospira) with the following settings: demand dose, 30 µg (0.5 µg/kg); no basal infusion; lockout time, 7 min; and a 4 h limit of 240 µg (4 µg/kg). Postoperative pain was assessed using a visual analogue scale (VAS). If the VAS score exceeded 4, the patient was eligible to receive intravenous tramadol 25 mg and meperidine 25 mg as rescue analgesics as per our protocol.
In the post-anesthesia care unit, the patient experienced no pain because of residual epidural anesthesia. However, he complained of shivering, so a forced-air warming blanket was provided and intravenous meperidine 25 mg was administered. Four hours after surgery, the patient reported that his dorsiflexion, plantar flexion, and the knee flexion returned to his usual range of motion bilaterally. Assuming that the epidural anesthetic effect had worn off, we evaluated the patient’s sensory blockade, motor blockade, and pain scores. His resting and dynamic VAS scores were 2 and 4, respectively. He showed sensory blockade from T8 to L3 at the midaxillary line (T8–9: decreased pinprick sensation of pain relative to the contralateral side; T10–L3: no pinprick sensation of pain). Moreover, he showed mild weakness against resistance during right knee extension but no issue with flexing and extending his left knee against both gravity and resistance.
The patient’s resting and dynamic VAS scores remained stable at 2–3 and 3–4, respectively, at 4, 12, and 24 h after surgery. In fact, all resting and dynamic pain scores were 1–2 and 1–3, respectively, throughout postoperative day 5 (Fig. 3). Monitoring the VAS score of the patient settled below 4, perineural PCA was discontinued at 48 h after surgery, and intravenous PCA was discontinued on postoperative day 5, in accordance with our hospital protocol. The patient’s fentanyl consumption was tracked using the PCA program. He received the first demand dose of fentanyl 30 µg through the PCA pump at 17 h after surgery. During the first 48 h, he pressed the PCA button four times, and his total fentanyl consumption was 120 µg. He pressed the PCA button twice on day 3, three times on day 4, and nine times on day 5. None of the pain scores exceeded 4, and no rescue analgesics were required during the first five postoperative days. At the 1 week and 1 month follow-up visits, the patient did not exhibit residual sensory-motor deficits or complain of symptoms suggestive of a neurological injury.
Discussion
The main origins of acute pain after total hip arthroplasty include the hip joint and incision site. Prior study has provided support for the LPB as an effective regional analgesic after total hip arthroplasty, with less opioid consumption compared to conventional systemic analgesia [6]. In a double-blind prospective trial, for example, the LPB provided enhanced analgesia and significantly reduced cumulative morphine consumption in the plexus group (5.6 ± 4.7 mg) as compared to the control group (12.6 ± 7.5 mg) until 6 h after randomization [6]. However, even with ultrasound guidance, the LPB is technically difficult to perform and carries a risk of serious complications [3]. Transmuscular QLB may be an effective alternative analgesic to the LPB. The QLB has been successfully used for surgical anesthesia during lower extremity amputation [7], as well as minimally invasive and total hip arthroplasty [8]. In our present case, the patient received a continuous transmuscular QLB as part of a multimodal analgesia after hardware removal and total hip arthroplasty. Notably, the patient did not request analgesic agents, beyond the perineural infusion and regularly scheduled oral celecoxib, until 17 h following surgery. Furthermore, our patient’s total opioid consumption during the first 48 h post-surgery was equivalent to 12 mg of morphine (fentanyl 120 µg) while about 40 mg of morphine was administered until the first 48 h in the study of Stevens et al. [6], indicating that this multimodal analgesia regimen was highly effective. In one cadaveric study, the transmuscular QLB demonstrated consistent spread of the local anesthetic to the L1 to L3 nerve roots, covering the genitofemoral, femoral, and obturator nerves [5]. In another cadaveric study, the transmuscular QLB resulted in the spread of the local anesthetic to the lumbar paravertebral space in 63% of the specimens, with the solution reaching the upper branches of the lumbar plexus and psoas major muscle in 70% of the specimens [9]. Consistent with the observed spread of anesthetic in cadavers following the QLB, patients receiving a QLB have reported lower extremity muscle weakness [10], and a retrospective study demonstrated that 357 of 2,382 patients showed evidence of quadriceps muscle weakness after all type of QLB (transmuscular QLB). Notably, the incidence was as high as 90% in anterior QLB [11].
We hypothesize that the transmuscular QLB provides effective analgesia after hip surgery, because this method partially or totally blocks the lumbar plexus (T12–L4), which innervates the hip joint and the incision site. After the QLB, our patient showed sensory blockade from T8 to L3. This sensory blockade presumably provided analgesia for the hip joint as well as the incision site through blockade of the lateral femoral cutaneous nerve (L2–3), subcostal nerve (T12), and ilioinguinal and iliohypogastric nerves (L1) [12].
Although our patient could extend the knee against both gravity and resistance, he exhibited decreased strength against resistance. There are two possible explanations for this finding. First, the local anesthetic solution spread to the L3 spinal nerve, because of which the femoral nerve (L2–4) was partially blocked. Second, although unlikely, differential blockade could have occurred because of the infusion of 0.2% ropivacaine instead of a more diluted solution through the catheter.
Additionally, it is known that the severity of pain decreases and the risk of catheter-related infection increases rapidly 48 h after total hip arthroplasty [13–15], so the catheter was removed 48 h after surgery. Although the indwelling catheter was removed at 48 h after surgery, the patient’s pain remained well controlled through postoperative day 4, following which his analgesic requirement sharply increased. In a follow-up interview, the patient reported that he only pressed the PCA button when his pain score was ≥ 4, in accordance with our acute pain service protocol. It remains unclear whether the prolonged analgesia after removal of the perineural catheter in our patient was a result of the QLB, although a previous case report has described prolonged analgesia after a QLB [4]. Further prospective studies are required to clarify this finding.
In summary, we described the successful use of a continuous transmuscular QLB as part of a multimodal analgesia regimen after total hip arthroplasty. Notably, the QLB provided highly effective analgesia without significant motor blockade. In addition, the block was technically easy to perform because the key targets could be easily located under ultrasound guidance; this also decreases the risk of complications. The findings from this case suggest that the continuous transmuscular QLB is a suitable alternative to the LPB for multimodal analgesia after total hip arthroplasty; however, additional case reports and prospective, randomized control trials are needed to further clarify our findings.