Introduction
Compared to its on-pump counterpart, off-pump coronary artery bypass surgery (OPCAB) has been consistently shown to provide short-term outcome benefits regarding renal dysfunction, bleeding complications, and hospital length of stay through the avoidance of contact activation and hemodilution related to cardiopulmonary bypass [1]. In addition, accumulating evidence supports a morbidity and/or mortality benefit with OPCAB in certain high-risk populations such as octogenarians or those with chronic renal failure or reduced left ventricular (LV) function [2–4]. However, large randomized clinical trials addressing the efficacy of OPCAB versus on-pump coronary surgery found conflicting results, suggesting a lack of long-term outcome benefits associated with OPCAB mainly due to the increased risk of early revascularization after surgery [5–7]. Recurrent ischemic attacks after OPCAB have mainly been attributed to the lower number of grafts and poorer graft patency [5–7]. To achieve complete revascularization, successful grafting at the lateral as well as the posterior wall is often required, during which hemodynamic deterioration due to mechanical heart displacement is most severe [8,9], and the expertise of the team becomes crucial [10].
Hemodynamic consequences of mechanical heart displacement
OPCAB requires imperative periods of mechanical heart displacement to expose target vessels. Mechanical cardiac constraint induces both systolic and diastolic dysfunction and conformational alterations in the tricuspid and/or mitral annuli [11,12]. More specifically, when exposing the left-sided target coronary vessels, the enucleation and rotation of the heart results in compression of the right ventricle (RV) against the pleura, which is accentuated by positive ventilation [13]. Compression of the RV, especially the inlet, becomes most prominent during lateral wall exposure for ramus intermedius or obtuse marginal artery, which results in significant RV dysfunction [14]. Furthermore, grafting at the lateral or posterior wall requires the cardiac apex to be repositioned to the uppermost position, which renders diastolic filling against gravity while the ventricles are already being restricted by the mechanical constraint of the stabilizers [9,12,13]. Thus, the primary hemodynamic consequence is impaired bi-ventricular diastolic filling, followed by systolic dysfunction induced by the mechanical constraint, not to mention that systolic and diastolic functions are closely interrelated [11,15]. Consequently, both atria become enlarged, and much higher filling pressures of the atria are needed to fill the constrained ventricles [8,12]. The net hemodynamic consequences of this bi-ventricular diastolic and systolic dysfunction include an inevitable decrease in cardiac output to various degrees with or without valvular insufficiency [11]. Although these hemodynamic consequences are transient (confined to the period of grafting) and usually well-tolerated by most patients, in extreme cases, hemodynamic collapse may occur, requiring emergent conversion to an on-pump procedure, which is well-known to be associated with unacceptably high morbidity and mortality rates [16,17]. As the mechanical cardiac constraint is most severe during lateral wall grafting, followed by the posterior wall [11], attempts at aggressive complete revascularization (the aim of surgical coronary revascularization) are confronted with significant hemodynamic decline, which may result in emergency conversion to an on-pump procedure [18]. Considering that hemodynamic deterioration is mostly attributable to mechanical heart displacement and a conversion rate > 10% is associated with an increased risk of mortality [19], appropriate decision-making regarding whether to proceed with the OPCAB is essential for patient safety before opening the coronary artery. Notably, the reported conversion rates of expert groups are usually < 3% [20], while the conversion rate from scheduled on-pump surgery to OPCAB ranges from 3.6% to 6.4% [5–7].
Predictors of hemodynamic deterioration
Hemodynamic collapse
Unfortunately, distinct predictors of significant hemodynamic deterioration are not known. However, cogent underlying mechanisms likely involve a complex interplay between the degree of mechanical constraint imposed on the heart and the patient’s cardiac function and coronary reserve. In addition, hemodynamic instability can be influenced by the type of stabilizer device used (suction or compression), as each type of stabilizer conveys a different profile of associated hemodynamic changes [21]. The largest study to date on risk factors for conversion to cardiopulmonary bypass revealed a higher prevalence of preoperative heart failure, left main coronary artery disease, and three or more diseased coronary vessels in patients who required intraoperative conversion to cardiopulmonary bypass [18]. Another large-scaled study has reported that salvage operations, LV hypertrophy, previous coronary surgery, history of cerebrovascular disease, prior myocardial infarction, diabetes, and low body surface area are risk factors for on-pump conversion [16]. The difficulty with predicting conversion was shown in a study that demonstrated that each additional increase in 1% of the LV ejection fraction was paradoxically associated with an incremental risk of on-pump conversion, while the study reported a relatively high conversion rate (11.6%) [22]. To further complicate matters, OPCAB has been associated with benefits in terms of morbidity and mortality in patients with reduced LV ejection fraction [4].
Diastolic function and outcomes
Although LV ejection fraction is the most studied index of systolic function in terms of outcomes [23], it is subject to numerous limitations, including a dependency on loading conditions [24]. Notably, diastolic dysfunction often precedes systolic dysfunction in patients with coronary disease, as early relaxation is an active process requiring adenosine triphosphate [25]. It should also be noted that mechanical heart displacement primarily results in impaired diastolic filling and dysfunction [11]. In this context, the ratio of transmitral flow velocity (E) to early diastolic velocity of the mitral annulus (e') has been shown to accurately predict normal and increased LV filling pressures [26]. Increased LV filling pressure is almost always accompanied by structural changes in the LV; therefore, E/e' serves as an indicator of diastolic dysfunction and has been shown to be closely correlated with mortality after myocardial infarction [27]. Accordingly, patients with elevated E/e' (> 15) were shown to exhibit more significant hemodynamic compromise during mechanical heart displacement in OPCAB, even when the LV ejection fraction was preserved [28]. Moreover, patients with an elevated E/e' ratio had a more significant drop in mixed venous oxygen saturation (SvO2) during grafting, which could not be restored to baseline values after sternum closure. Subsequently, this resulted in a longer ventilation time and length of stay in the intensive care unit. Consistent with these results, large-scale retrospective studies of patients undergoing multivessel OPCAB found that E/e' was an independent risk factor of adverse outcomes, while the LV ejection fraction was not [29,30]. Nonetheless, the degree of hemodynamic deterioration after mechanical heart displacement remains difficult to predict due to its complex mechanisms.
Hemodynamic management strategies during mechanical cardiac displacement
Hemodynamic management strategies during OPCAB should follow the fundamental principles of managing patients with coronary artery occlusive disease; thus, proper maintenance of the myocardial oxygen supply-demand balance should be given utmost priority before successful grafting is completed [31]. In general, mean arterial pressure (MAP) should preferably be maintained above 70 mmHg to ensure adequate coronary perfusion and the heart rate should be maintained at the lower end of normal ranges to minimize myocardial oxygen demand while avoiding a precarious reduction in cardiac output [11,32].
Preload
In this context, assuming that the mechanical cardiac displacement can be tolerated, a major countermeasure to restore the decrease in cardiac output would be preload augmentation. This would be the most plausible intervention considering that mechanical cardiac displacement primarily results in impaired diastolic filling [11,33]. Accordingly, preload expansion has been shown to be sufficient to counteract the reduction in cardiac output and coronary blood flow in most cases [33]. For this purpose, a fluid bolus can be administered; however, it will inevitably result in increased interstitial edema when the heart is returned to its normal position. Thus, shifting the patient temporarily to the Trendelenburg position can result in effective central volume augmentation and restoration of MAP and coronary blood flow while facilitating the exposure of the lateral or posterior wall target vessels [34]. However, caution is advised as prolonged and extreme Trendelenburg position combined with RV compression by stabilizers may result in cerebral venous congestion from impaired venous drainage, which may yield adverse neurologic outcomes [35].
Mean arterial pressure
Apart from preload optimization, vasopressors are usually required to help maintain the MAP above 70 mmHg. Dopamine should be avoided because of its arrhythmogenic tendency and negative influence on outcomes [36,37], while the use of norepinephrine with vasopressin in an additive manner has been shown to be a useful strategy [38]. In contrast to phenylephrine, which is a pure Alpha-1-adrenergic receptor agonist, norepinephrine exerts some beta effects, although its predominant action is vasoconstriction in clinically recommended dose ranges [39]. Norepinephrine has been shown to not exert dangerous beta-adrenergic effects that may increase myocardial oxygen demand in dose ranges < 0.3–0.5 μg/kg/min and is the preferred vasopressor across many critical care centers [38,39]. In the case that the norepinephrine requirement exceeds this dose range however, the addition of vasopressin up to 2.4 to 4 IU/h may be used to maintain the MAP, as this avoids the negative effects associated with norepinephrine [38]. Vasopressin not only acts on its own V1 receptor to induce vasoconstriction, but also augments the effects of norepinephrine [39]. Moreover, it is especially useful in patients receiving angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, even in cases of catecholamine refractory shock related to relative vasopressin depletion [40,41]. It is also valuable in vasoplegic shock involving the excessive production of inducible nitric oxide since its mechanisms of action involve the inhibition of cyclic guanosine monophosphate [39]. Moreover, V1 receptors are nearly absent in the pulmonary vasculature; thus, vasopressin was shown to induce an increase in MAP without increasing pulmonary vascular resistance, which is especially favorable for the failing RV [42,43].
Afterload and contractility
Other main determinants of cardiac output that we can potentially manipulate to augment forward stroke volume against the mechanical constraint include a reduction in afterload, which is usually reduced by general anesthesia, and further pharmacological interventions to achieve additional afterload reduction may endanger coronary perfusion [44]. Pharmacological interventions to increase myocardial contractility may be attempted, although this inevitably increases myocardial oxygen demand and may result in an ischemic insult, though the exact threshold for this cannot be predicted. The most commonly used inodilator is dobutamine, which has the advantage of fast onset and offset and can be titrated from low to high doses depending on the patient’s coronary reserve [45]. However, the majority of patients presenting for coronary surgery are taking beta-blockers, which may render the myocardial contractile response to beta-agonists, such as dobutamine, unreliable. Moreover, dobutamine has been demonstrated to increase myocardial oxygen demand beyond the supply in patients with coronary disease [46]. In contrast, milrinone has a late onset (thus, requiring a loading dose, which would accelerate the onset at the expense of hypotension) and offset (1 h after discontinuation). A continuous infusion of milrinone for 30 min yields similar efficacy (as with a bolus) with an improved safety profile, as it requires no bolus dose and is not associated with hypotension [47]. As a phosphodiesterase III inhibitor, the inotropic and afterload-reducing effects of milrinone can be reliably anticipated even in patients on long-term beta-blockers. In addition, milrinone has been shown to maintain the myocardial oxygen supply-demand balance at a ratio of 1 : 1 [48], making it a more appropriate choice in patients with coronary disease. Furthermore, a continuous infusion of milrinone (without a bolus) has been shown to be effective in reducing mitral regurgitation during OPCAB without eliciting any untoward events, such as increased heart rate [49], which broadens its indications in patients undergoing OPCAB.
Heart rate
On the other hand, an increase in heart rate can be an attractive option to increase the cardiac output, as it can be precisely controlled through atrial pacing during OPCAB and as the more severe form of mechanical constraint results in cardiac dysfunction mimicking compressive syndromes [11]. Thus, assuming that the preload is optimized, the stroke volume becomes relatively fixed, and the cardiac output becomes more heart-rate-dependent [50]. However, an increase in heart rate induces a linear increase in myocardial oxygen demand, and an increase in contractility [51]. Thus, pacing should be reserved for patients with extreme bradycardia (< 55 beats per minute [bpm]), depending on the patient’s coronary reserve and the surgeon’s expertise with performing a graft at a faster heart rate. A heart rate up to 70 bpm is generally well-tolerated in most patients and does not result in serious disruptions in the myocardial oxygen supply-demand balance or hinder the surgeon’s ability to perform the grafting procedure. In cases of significant heart failure and/or increase in mitral regurgitation, faster heart rates up to 80 bpm may be attempted, whilst cautioning the prerequisite of maintaining the myocardial oxygen-supply demand balance.
RV function and ventilatory management
Being a low-pressure, more compliant chamber with thinner walls, the RV may suffer more severe compression and dysfunction by mechanical constraint compared to the LV [9,21]. To alleviate RV compression against the pleura, vertical pleurotomy can be attempted; however, its clinical benefit remains unclear [52]. Removing the positive end-expiratory pressure and decreasing the tidal volume usually create additional space for the RV to engage in, which may help relieve the constraint. Hemodynamic management strategies using inodilators and atrial pacing, targeted at improving RV function, are essentially the same as that described above. Other considerations include the fact that the pulmonary artery pressure usually increases during mechanical heart displacement, especially during lateral wall grafting, due to increased left atrial pressure and impaired diastolic filling [9,14]. Accordingly, a possible rescue strategy for RV dysfunction in conjunction with increased pulmonary artery pressure would include the application of inhaled milrinone (possibly in combination with epoprostenol) [53], which would act more on the pulmonary vasculature to relieve the afterload of the RV in addition to its inherent inotropic action. However, the efficacy of this strategy in OPCAB remains unknown, although a case report showing the beneficial effect of inhaled epoprostenol on relieving RV afterload and venous congestion is available [54].
Hemodynamic targets during mechanical cardiac displacement
The mechanical constraint can be severe enough to incur tamponade physiology and compressive syndromes that cannot be overcome by optimizing the aforementioned major determinants of cardiac output. Thus, proper hemodynamic targets need to be established that will be used to objectively guide the decision to relieve or adjust mechanical cardiac displacement or allow conversion to an elective on-pump procedure (which is not associated with dismal prognosis in contrast to an emergent conversion) before coronary arteriotomy in refractory cases.
Pulmonary artery catheter
Pulmonary artery catheter (PAC) monitoring can be especially helpful for ruling out the intractable form of mechanical heart displacement. Tamponade physiology and compressive syndromes can be characterized by the equalization of diastolic pressures between the left and right heart chambers [55]. In this context, the central venous pressure (CVP) measured by the PAC reflects the RV end-diastolic pressure, while the pulmonary artery diastolic pressure (PADP) roughly reflects the pulmonary artery occlusion pressure (PAOP), which is a surrogate of LV end-diastolic pressure [56]. Therefore, if the CVP is equal to or greater than the PADP after mechanical heart displacement, the cardiac constraint conveys compressive syndromes. In addition, when using a PAC with an RV pacing port that enables simultaneous monitoring of RV pressure, severe RV failure can readily be appreciated by an increase in RV end-diastolic pressure above the PADP. Thus, the surgeon should be advised to relieve mechanical constraint before coronary arteriotomy to avoid tamponade physiology and subsequent hemodynamic collapse. PAC monitoring can reflect these dynamic changes after cardiac displacement in real time, allowing for quick decision-making.
In addition, the importance of monitoring SvO2 through the PAC has been appreciated [57]. The target to maintain SvO2 above 60% has been advocated mainly based on the physiological limit of the oxygen extraction ratio, by which the tissue can still obtain adequate oxygen supply despite reduced cardiac output and oxygen delivery [58,59]. Recently, a single-center, retrospective analysis involving 1,071 OPCAB patients showed that even a transient decrease in SvO2 < 60% during lateral wall grafting was associated with adverse outcomes (odds ratio: 2.72, 95% CI [1.60, 4.61], P < 0.001) along with well-known risk factors including advanced age, chronic kidney disease, E/e', and EuroSCORE II [9]. In contrast, the MAP and cardiac index were not significantly different between the morbidity and non-morbidity groups (which were greater than 75 mmHg and 1.7 L/min/m2, respectively) during grafting in that study. Regarding the emphasis on the association between an MAP < 65 mmHg and poor outcomes in major surgeries [60,61], the lowest MAP score was 68 mmHg in that study (per protocol, the MAP was maintained over 70 mmHg), thereby it had no negative effect on outcomes. While the cardiac index decreased to a mean of 1.7 L/min/m2, it was not associated with poor outcomes, suggesting the superior prognostic importance of SvO2 reflecting the net circulatory threat of the disrupted oxygen supply-demand balance induced by cardiac displacement. Accordingly, the use of inotropics alone to increase the cardiac index may not be sufficient to solve the problem. Interestingly, hyperoxia has been shown to enhance oxygen supply without increasing the cardiac index in animal models of circulatory shock, possibly due to the redistribution of blood flow to hypoperfused splanchnic tissues [62,63]. Indeed, an increase in FiO2 to 0.8 has been shown to increase SvO2 by 6–8% in cardiac surgery patients [64]. However, given the potential drawbacks of oxygen toxicity in patients with stable multivessel coronary disease in terms of post-stenotic myocardial deoxygenation and dysfunction [65], caution is advised when applying high FiO2 in OPCAB, which merits further study.
Transesophageal echocardiography
The role of transesophageal echocardiography (TEE) in assessing the degree of cardiac constraint is also indispensable. Although the insonation windows become limited due to the posterior pericardial stitch and gauze swabs, most of the mid-esophageal (ME) or upper-esophageal (UE) views can still be obtained. The most useful images are obtained by ME RV inflow-outflow and ME long-axis views [66]. Especially during lateral wall grafting when the constraint is most severe, the ME 4-chamber view can be deceiving as the RV compression may appear severe. In this case, the ME RV inflow-outflow view can be more helpful for assessing the degree of RV free wall compression, especially at the inlet, to rule out significant mechanical compression with or without tricuspid stenosis or regurgitation. Compression of the RV outflow tract extending to the free wall can be frequently observed during right mammary artery harvesting using the sternal blade of the internal mammary artery sternal retractor (Supplementary Video 1). Depending on RV function, such outflow tract narrowing may not be tolerated, and thus, changing the retractor to a lifting type fixed at the surgical table (e.g., Rultract Skyhook Retractor SystemsTM, Rultract Inc., USA) may be required. Continuous-wave Doppler assessment of the pressure gradient at the RV outflow tract may help to rule out severe mechanical obstruction (peak flow velocity > 4 m/s), which must be avoided. For this purpose, the ME ascending aortic short axis view or UE aortic arch short axis view may be helpful (Fig. 1). In extreme cases of RV compression and failure, RV end-diastolic pressure would likely surpass the PADP, leading to a diastolic opening of the pulmonary valve, which must be avoided [67]. In contrast, application of a sternal retractor for left internal mammary artery harvesting usually results in compression of the right pleural margin near the cardiac border and rarely causes serious RV compression.
Inspection of the ME long-axis view is also essential to rule out compressive syndromes and ventricular interdependence, development of mitral regurgitation, LV outflow tract obstruction (LVOTO) with or without systolic anterior motion (SAM) of the mitral valve, or intracardiac gas introduction. In addition to the dynamic changes in the relationship between the CVP and PADP, significant mechanical constraint can be portrayed as ventricular interdependence created by RV compression against the pleura and LV compression by the stabilizer, despite being enucleated out of the opened pericardium. This can be observed as paradoxical septal motion or dyskinesia of the entire segment of the LV wall, which must be avoided for safe completion of an OPCAB. On the other hand, as the ascending aorta remains fixed at its natural position, mechanical verticalization and rotation of the heart bring the basal portion of the LV antero-septum closer to the anterior leaflet of the mitral valve and may create LVOTO with or without SAM (Supplementary Video 2), which must be avoided. In mild cases, segmental dyskinesia of the basal portion of the LV antero-septum without LVOTO can be observed after heart displacement, which can be tolerated as long as the other previously mentioned hemodynamic targets (MAP > 70 mmHg, SvO2 > 60%, and CVP < PADP) are met (Supplementary Video 3). In theory, these findings are more likely to occur in patients with a sigmoid septum and/or dilated ascending aorta [68].
Comprehensive monitoring (evolving issues)
Considering the importance of gathering comprehensive information from PAC monitoring, TEE, and the surgical field (or any adjunct monitors that may be required depending on the patient’s comorbidities) for proper decision-making after mechanical cardiac displacement, evolving monitoring modes incorporate all of the intraoperative monitoring inputs in a single monitor to aid in quick decision-making (Supplementary Video 4).
Other modalities of monitoring include cerebral oximetry and transgastric abdominal ultrasound (either by TEE or point-of-care ultrasound) that enable appreciation of not only the effects of OPCAB on cardiac structure and function, but also on extracardiac organs such as the brain, liver, and kidney. For instance, Trendelenburg position combined with RV compression and impaired cerebral venous drainage during lateral wall grafting that subsequently results in emergence delirium can manifest as significant cerebral desaturation through increased deoxyhemoglobin variation (indicating venous congestion) and burst suppression detected by Root O3® cerebral oximetry (Masimo, USA) and processed electroencephalography, respectively [35]. In line with these observations, systemic venous congestion elicited by mechanical RV compression and dysfunction may result in renal, hepatic, or portal venous congestion. The latter has been portrayed as portal vein pulsatility that can be readily assessed with TEE in real-time and has been identified as an independent predictor of detrimental outcomes in cardiac surgery in an international study [69]; however, OPCAB was excluded from this study.
Troubleshooting
Myocardial ischemia
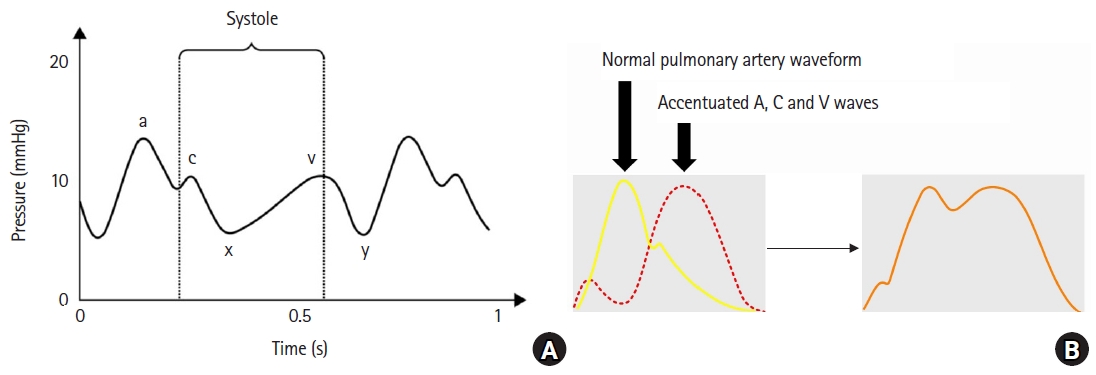
Apart from hemodynamic deterioration solely induced by mechanical heart displacement, myocardial ischemia and subsequent cardiac dysfunction may also cause hemodynamic collapse. The significance of ischemia is dependent on the degree of target-vessel stenosis and the collateral network. The most detrimental ischemia occurs when flow is interrupted in a culprit vessel, usually with the percentage of stenosis between 50% and 80% and poor collateralization [31]. Thus, these events are rare in patients undergoing OPCAB when the graft reconstruction time remains below 15 to 20 min [9], as they usually present with more than 80% stenosis accompanied by some degree of collateral network [70]. Nonetheless, some form of distal coronary perfusion (such as an intracoronary shunt) is usually applied during left anterior descending artery grafting (largest myocardial area at risk of ischemia after temporary occlusion to obtain a bloodless surgical field), distal right coronary artery grafting (due to the risk of complete atrioventricular [AV] nodal block), or culprit lesions without angiographically documented collateral networks [11,31]. Conventional electrocardiographic (ECG) ST-segment changes can be misleading, as the electrical gain is significantly reduced due to mechanical cardiac displacement and loss of continuity with the surrounding pericardium. Even after increasing the ECG gain, which will increase the introduction of artifacts as well, proper ECG waves are often poorly visible, hindering its ability to detect ischemia. Moreover, cardiac displacement causes changes in the electrical depolarization vector of the myocardium, thereby altering the positional relationship between the limb and chest leads (usually II [right coronary territory] and V [left anterior descending territory] in cardiac surgery) and the corresponding myocardium [11,21]. Likewise, the detection of newly developed regional wall motion abnormalities can be challenging due to the limited insonation window and systolic dysfunction induced by cardiac constraint, irrespective of ischemia. Of note, the pulmonary artery pressure waveform can also aid in the detection of myocardial ischemia during grafting. An increase in the pressure with changes in the waveform induced by superimposition of the prominent A, C, and V waves can be indicative of early subendocardial myocardial ischemia and the resultant reduction in LV compliance (with or without mitral regurgitation), even preceding the ECG changes (if any ECG changes can be detected at all) (Fig. 2) [71]. Whenever these changes in the pulmonary artery waveform are observed, significant myocardial ischemia should be suspected with high specificity and managed accordingly [31]. If the coronary artery is not opened, the heart should be returned to its natural position. If these changes are observed during grafting, insertion of an intracoronary shunt to facilitate distal perfusion should be considered along with hemodynamic management strategies aimed at increasing coronary perfusion pressure and decreasing myocardial oxygen demand.
However, monitoring the PAP, along with the PAOP, has been shown to be insensitive to detecting myocardial ischemia in patients undergoing on-pump coronary surgery [71]. An increase in PAOP of 3 mmHg over the baseline yielded a sensitivity of 33% for detecting ischemia, whereas all patients who exhibited an increase in PAOP had inferior wall ischemia and possible transient papillary muscle dysfunction accompanied by regurgitation [72]. Therefore, all monitoring methods have limitations during OPCAB, and vigilantly relying on their combination rather than a single monitor to detect intraoperative myocardial ischemia must be exercised [21,31].
Atrioventricular nodal block
Another form of critical ischemia that can be observed during OPCAB is AV nodal block. This can usually be observed during grafting at the distal right coronary artery in the vicinity of the AV nodal branch, which is the exclusive feeding vessel for the AV node in 80% of patients [73]. Fortunately, complete AV nodal block does not occur suddenly, and AV nodal ischemia usually presents stepwise from first-degree AV nodal block advancing to second-degree and then eventually to complete AV nodal block [74]. Therefore, the PR interval should be closely monitored, and any signs of prolongation should alert clinicians to an ensuing complete AV nodal block. Attempts to promote AV nodal branch flow should be initiated, such as inserting an intracoronary shunt and increasing the MAP. Most importantly, epicardial (or endocardial using a PAC with an RV pacing port) RV pacing should be ready at hand to allow ventricular pacing in case of complete AV nodal block. Ventricular pacing allows for additional time to finish the grafting procedure while providing cardiac output even in the presence of AV nodal block, as AV nodal ischemia is usually resolved after completion of grafting in most cases.
Massive coronary gas embolism
An unexpected devastating form of ischemia with hemodynamic collapse during grafting after coronary arteriotomy may develop due to massive air embolism [75]. To facilitate visualization of the anastomosis site by obtaining a bloodless surgical field, CO2 blowers are often used in conjunction with the proximal coronary snare. In cases where the proximal snare cannot provide complete occlusion due to severe calcified atheromatous changes of the coronary artery, CO2 along with room air (due to the Venturi effect) can migrate retrogradely to the proximal site of the coronary artery all the way to the coronary ostium and sinus of Valsalva as the CO2 blower can create pressures exceeding 50 mmHg, which can be higher than the systemic diastolic pressure [75]. When the amount of gas embolism is overwhelming, exceeding the body’s clearance capacity, mechanical obstruction of the right coronary ostium by the gas can be induced, yielding RV dysfunction and hemodynamic collapse (Supplementary Video 5A). Therefore, even when everything seems in order during the grafting procedure, intermittent inspection of the ME long-axis view is imperative to detect possible gas embolism and to prevent further build-up that may incur devastating hemodynamic consequences (Supplementary Video 5B). In cases of hemodynamic collapse, needle aspiration of gas and intra-aortic epinephrine injection along with conventional resuscitative measures may help to restore the hemodynamic status [75,76].
Elective on-pump conversion
Despite endeavors to adjust the mechanical constraint (according to the previously described hemodynamic targets) and optimize loading conditions to promote forward ejection at the given target vessel stabilization, critical decisions to choose elective on-pump conversion before opening the coronary artery must be made in the following situations. First, while no comprehensive evidence exists in this regard, the authors recommend that even when other macro-hemodynamic variables seem acceptable, serious consideration should be given to conversion when the SvO2 falls below 50%, which indicates a shock state beyond the limit of compensation by increased oxygen extraction ratio in the tissues [1,58,59]. Second, severe mitral regurgitation may force on-pump conversion. Mitral regurgitation, either by mechanical constraint alone or in combination with ischemia, may develop, which would sometimes take a considerable time to resolve even after placing the heart in its natural position without coronary arteriotomy. Apart from the adjustment of the mechanical constraint, intravenous milrinone has been shown to be beneficial [49]. In cases of ischemic origin with congestion, intravenous nitrate along with venous phlebotomy (aseptic venous blood removal through the large-bore central venous access to a cell salvage device, which would later allow autotransfusion of packed erythrocytes) in amounts of up to 500 to 700 ml depending on the degree of congestion may help. In a similar context, temporary, partial inferior vena cava snaring was reported to be effective in ameliorating ischemia-related sudden increase in pulmonary artery pressure and aggravated mitral regurgitation accompanied by severe LV dysfunction during OPCAB through decreased venous return and cardiac chamber dimensions [77]. Nonetheless, severe mitral regurgitation may continue to develop after mechanical heart displacement, and if the target vessel is the culprit vessel or if complete revascularization seems essential, on-pump conversion is required. In the case that the surgical team decides to perform on-pump ‘beating’ surgery without cardioplegic arrest, it is advisable to insert an LA or LV vent depending on the residual degree of mitral regurgitation after cardiopulmonary bypass to avoid left atrial distention and subsequent pulmonary edema.
Conclusion
Mechanical heart displacement during OPCAB exerts various degrees of hemodynamic deterioration depending on the complex interplay among the degree of mechanical constraint, cardiac function, and coronary reserve. To safely perform an OPCAB, certain hemodynamic targets need to be met to avoid jeopardizing the patients’ prognosis. These targets are as follows: 1) maintenance of MAP above 70 mmHg, 2) maintenance of SvO2 above 60%, and 3) preventing the CVP from rising above the PADP, which may indicate compressive syndromes and/or severe RV failure (Fig. 3). Also, TEE examinations should rule out significant ventricular interdependence manifested by dyskinesia involving a whole segment of the LV wall or septum. In addition, careful observation for diastolic opening of the pulmonary valve (indicating RV failure), LVOTO, mitral regurgitation (whether induced by mechanical constraint and/or ischemia), and air embolisms should be undertaken to rule out rare causes of hemodynamic collapse that may force emergent conversion to an on-pump procedure yielding detrimental outcomes. Finally, flawless communication with the surgeon is essential to avoid unnecessary periods of hemodynamic instability that may harm patient outcomes.