Ambiguous pediatric endotracheal tube intubation depth markings: a need for standardization
Article information

The use of uncuffed endotracheal tubes (ETTs) is preferred in children for securing the airway during general anesthesia or in the intensive care unit. We noticed a difference in the depth marks of uncuffed tubes such as single line, double line, broader black line at different lengths, and even no markings at all (Fig. 1). Tube markings vary from 1.8 to 6.5 cm, and there are no manufacturer recommendations for them. This issue needs to be reviewed to improve safety margins in pediatric intubations. Adherence to ETT insertion depth guidelines may be insufficient to prevent malposition [1]. ETTs have a black line (vocal cord marking) near the distal end that guides proper placement. This is a simple, safe, and reliable method for ensuring appropriate length and avoiding endo-bronchial intubation. Many trainees are uncertain about the use of common vocal cord markings on ETTs. Neonates and infants are at a higher risk of endo-bronchial intubation due to short tracheal length. A wide discrepancy in intubation depth marker placement can create confusion [2]. Even positioning ETTs by auscultation may lead to deeper placement than the mid-trachea [3]. We use tracheal palpation, PALS (Pediatric Advanced Life Support) predictive formula, and bilateral chest auscultation to ensure equal breath sounds [4]. Further confirmation can be done by using fiberoptic broncoscope or ultrasonography if required [5]. We suggest standardizing ETT markings as well as the enforcement of clear manufacturer recommendations for their usage to avoid endo-bronchial intubations.
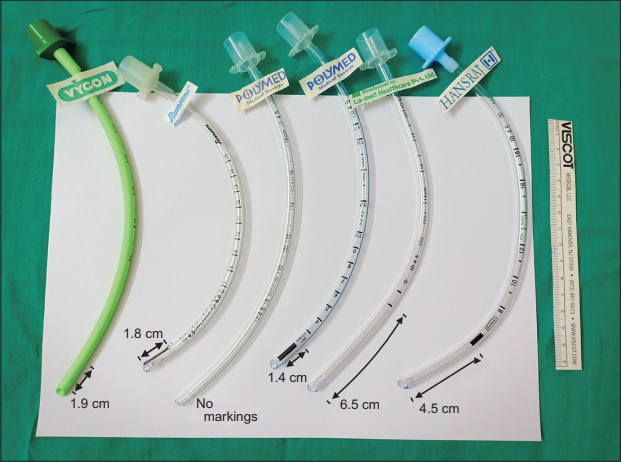
Pediatric endotracheal tubes (ETT) marking variations.
Acknowledgements
Mr. Surya Kanta Acharya and Mr. Prakash Kumar Swain (OT Staff).
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Authors’ contribution
Neha Singh (Conceptualization; Supervision; Writing–original draft; Writing–review & editing)
Chitta Ranjan Mohanty (Conceptualization; Writing–original draft)
Parnandi Bhaskar Rao (Conceptualization; Writing–original draft)