Breathing circuit leak – an unexpected finding
Article information

Owing to the decreased risk of pulmonary cross-contamination associated with disposable breathing circuits, their use is increasing. However, these circuits may be a source of airway obstruction or leakage [1]. Leaks in the breathing circuit occur in more than 50% of tested circuits, and most are resolved during routine machine checks [2]. We report a case of breathing circuit leakage due to an unintentional human error that occurred intraoperatively. Written informed consent for publication of this report was obtained from the patient.
A female patient aged 17 years and weighing 40 kg was scheduled for a left frontal craniotomy and left frontal bleed evacuation. She had a Glasgow Coma Score of 15 and no motor deficits. The patient was known to have atrial and ventricular septal defects with tricuspid atresia, and her oxygen saturation was 88 percent on room air. Before the start of the case, the anesthesia machine (Dräger Primus; Drägerwerk AG & Co, Germany) passed a routine self-test as per manufacturer’s recommendation, with no errors detected. No leaks or defects were observed in the newly attached disposable anesthesia breathing circuit. After anesthesia induction, the orotracheal intubation was done with a 7.0-mm inner diameter endotracheal tube (ETT) and connected to the ventilator via a disposable breathing circuit. Anesthesia was maintained with sevoflurane in an air-oxygen mixture (50%) at a flow rate of 2.0 L/min. An oxygen saturation of 98%–100% and normocapnia were maintained. Patient was placed supine with 10–15 degree head elevation. The head was turned slightly towards the right and fixed in a Mayfield Skull clamp. The surgical site was prepared, and the patient was draped using sterile sheets. The anesthesia machine was placed at the foot end on the left side of the patient with the breathing circuit running under the sterile surgical drapes connecting the ETT at the head end to the anesthesia machine at the foot end. A skin incision was made, and the skin flaps were retracted using a fishhook retractor. Approximately 10 min after the start of surgery, collapse of the ventilator bellows with inability to deliver an adequate tidal volume and hypocapnia were noted. The ETT position, cuff pressure, circuit connection, and ventilator function were checked; however, no leaks were detected. The surgical procedure was stopped, the surgical clothes were carefully turned to one side to check the breathing circuit under the drape. On turning the drape, it was observed that the towel clip which was used to fix the fish hook retractor to the drapes, has pierced the breathing circuit underneath it and there were small holes in the circuit (Figs. 1A-C). The breathing circuit was replaced and no further leaks were detected. The rest of the intraoperative course was uneventful.
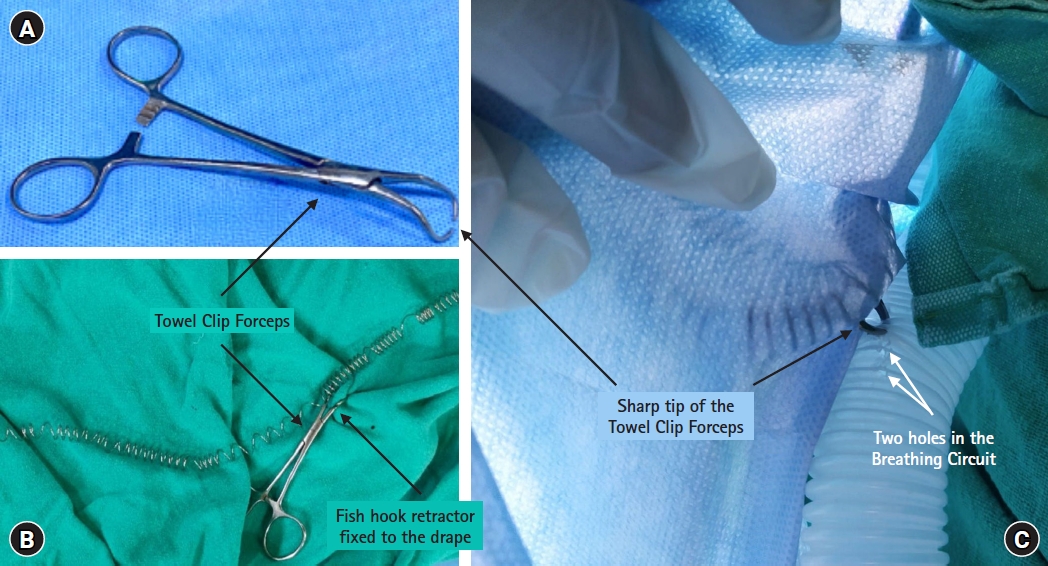
The sharp tip of the towel clip forceps (A) was used to fix the fish hook retractor to the drape (B), which caused the holes in the breathing circuit (white arrows), which led to the leak in the breathing circuit (C).
Leaks in the anesthesia circuit, which can lead to hypoxia, hypoventilation, inadequate delivery of inhaled anesthetic gases, and contamination of the operating room, can be caused by disconnection or damage to the breathing circuit [3]. It can be detected by an audible leak sound, collapse of the breathing bag and ventilator bellows, inability to ventilate, decrease in oxygen saturation, fall in end tidal carbon dioxide, decrease in tidal volume and airway pressure [3,4]. Previous case reports have attributed corrugated circuit leaks to tube holders [3] and hot air fans [5]; however, the sharp tip of towel clip forceps is a unique finding. Thus, whenever anything is fastened to surgical drapes using a sharp object, feeling and identifying the objects underneath the surgical drapes, such as breathing circuits or intravenous tubing, is necessary to avoid unintentional damage. The routine practice of checking for leakage in the breathing system after draping can prevent major mishaps. Leaks in breathing circuits may lead to significant complications if they are not identified. Therefore, anesthesiologists’ vigilance and preparedness in dealing with such situations can help prevent adverse outcomes.
Notes
Funding: None.
Conflicts of Interest: No potential conflict of interest relevant to this article was reported.
Author Contributions: Deepak Nandwana (Investigation); Saurav Singh (Writing – original draft; Writing – review & editing); Gyaninder Pal Singh (Supervision); Srinivasan Ravi (Investigation)