Ultrasound-guided anterior quadratus lumborum block for postoperative pain after percutaneous nephrolithotomy: a randomized controlled trial
Article information

Abstract
Background
The quadratus lumborum block (QLB), which is reported to provide analgesia to the abdominal region, is a newly defined fascial plane block method. The present study aimed to investigate the effect of ultrasound guided anterior QLB on the postoperative pain scores after percutaneous nephrolithotomy (PNL).
Methods
In this prospective, randomized, controlled single-blind study, 60 patients with elective PNL operations were randomized into 2 groups. In Group B (n = 30): anterior QLB+ intravenous patient-controlled analgesia (PCA) morphine and in Group C (n = 30): intravenous PCA morphine. Outcome measures were included for visual analog scale (VAS) scores and cumulated consumption for 24 hours postoperatively. Adverse effects, additional analgesic requirement, and intraoperative opioid requirement were recorded.
Results
The mean values of the quantity of cumulated morphine used at the 6th, 12th, and 24th hours were found to be statistically significantly lower in Group B (P < 0.05). The VAS scores were found to be statistically significantly lower in Group B (P < 0.05). There were no statistically significant differences in the rate of adverse effects, additional analgesic requirement, and intraoperative opioid requirement between the groups.
Conclusions
The study results suggest that anterior QLB is an effective treatment option for postoperative analgesia of PNL.
Introduction
Recently, the percutaneous nephrolithotomy (PNL) method, which is often described as a minimally invasive procedure, is frequently used in the treatment of kidney stones. In the updated European Association of Urology stone disease guidelines, PNL is recommended as the first choice in kidney stones above 2 cm [1]. Although PNL is applied as a minimally invasive procedure, dilatation of the renal capsule and parenchymal duct, and peritubular distension of the nephrostomy tube were identified as the cause of postoperative pain [2,3].
For postoperative pain, regional anesthesia methods are frequently used as well as intravenous drugs, which are essential because they reduce postoperative complications and hospitalization periods [2-4]. Intercostal block, paravertebral block, and peritubular infiltration are frequently used as regional anesthesia methods. For all 3 methods, lower pain scores or less opioid use was found in the literature compared to intravenous analgesic drug applications [5-7].
Recently, truncal blocks, which can be described as less risky than central blocks, are used for many surgical procedures with ultrasound guidance [8]. The quadratus lumborum block (QLB), which is reported to provide analgesia to the abdominal region, is a newly defined fascial plane block method. Though the application method seemed similar to posterior transversus abdominis plane (TAP) block when it was first defined, the injection site is deeper and more dorsal to transverse abdominis aponeurosis [9,10]. It has been reported that local anesthesia applied between the quadratus lumborum (QL) and thoracolumbar fascia can spread to the paravertebral area due to the anatomical structure of the fascia; and is effective on somatic and visceral pain at the level of thoracic 5 (T5)-lumbar 1 (L1) after the block [8-10]. QLB can be applied as 4 different types called lateral (QLBI), posterior (QLBII), anterior (transmuscular QLB, QLB III), and intramuscular methods [11-14].
In this study, we aimed to investigate the effect of ultrasound-guided anterior QLB applied to the QL muscle on the pain scores and morphine consumption after PNL. We hypothesized that the patients who applied QLB would have lower visual analog scale (VAS) values and lower morphine consumption than the group for which QLB was not applied.
Materials and Methods
A prospective, randomized, controlled, single-blind study was conducted per the Declaration of Helsinki. The approval of the local ethics committee was received, and 70 patients scheduled for a PNL operation were evaluated in terms of the suitability to the study (Local Ethics Committee Ethical number: 2018-1/32, Clinical Trials.gov identifier: NCT03425162).
Patients aged 20-60 years, American Society of Anesthesiologists physical status I-II risk class and undergoing PNL operations were included in the study. Exclusion criteria were the presence of allergies to medications used, not giving consent to participate in the study, the presence of infection at the site of the blockage, and a body mass index (BMI) above 35 kg/m2. Sixty patients agreed to participate in the study and received written informed consent. These patients were randomized with a spontaneous numbers table into 2 groups labeled Group B (n = 30): anterior QLB with bupivacaine (20 ml, 0.25%) + intravenous patient-controlled analgesia (PCA) morphine, and Group C (n = 30): intravenous PCA morphine (Fig. 1).
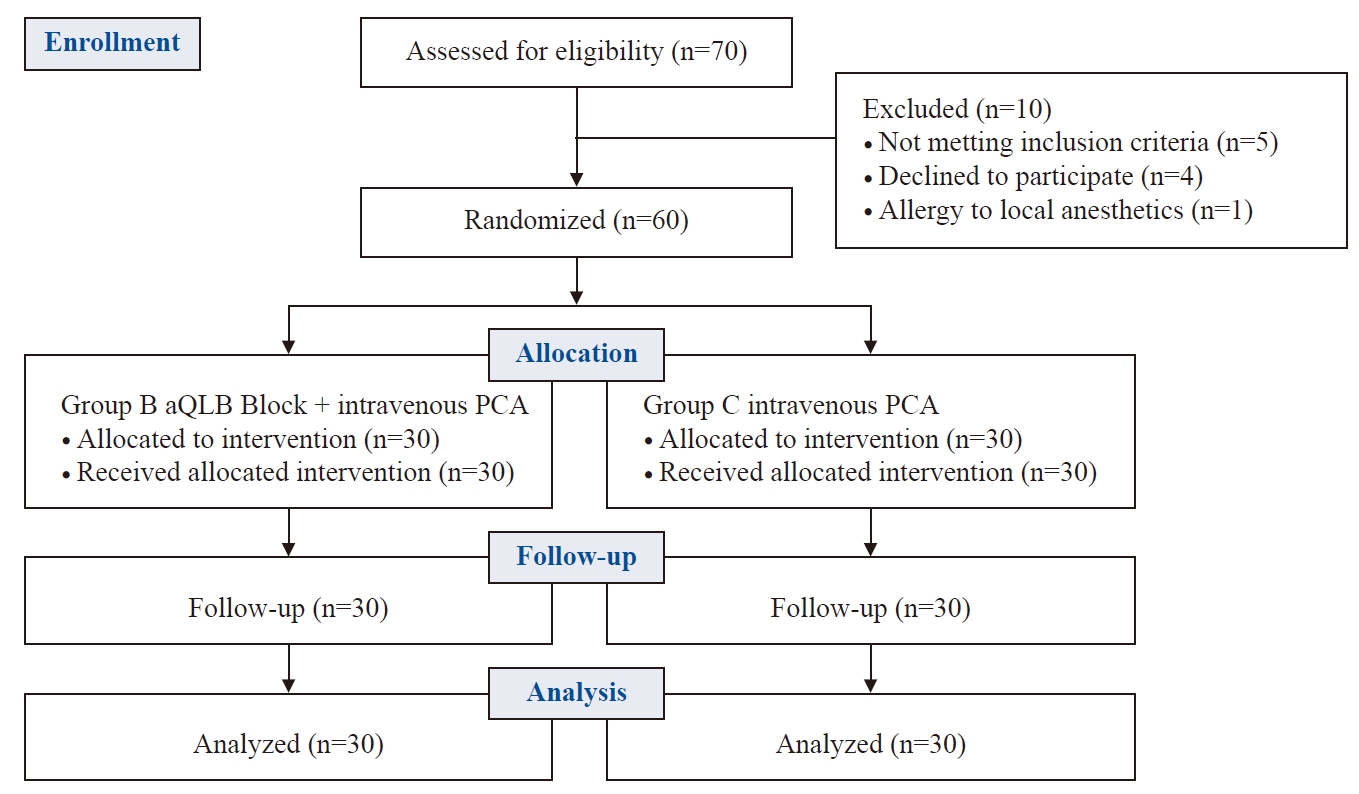
CONSORT diagram. aQLB: anterior quadratus lumborum block, PCA: patient controlled analgesia.
General anesthesia was administered initially intravenously with propofol and rocuronium, and then by inhalation anesthesia with sevoflurane, air, and O2 mixture, 2.5-3 L/min flow. Analgesia was given as 1 μg/kg fentanyl if needed. The surgical procedure was performed in the prone position.
Surgical procedure
Patients were placed prone, and percutaneous access was achieved under fluoroscopy using an 18 gauge (G) needle and guidewire. Channel dilatation was performed using Amplatz dilators, and the Amplatz renal sheath was placed in either 30 F or 32 F. We used a nephroscope and a ureteroscope to work with the collection system. Ultrasonic or laser lithotripsy was performed to break up the kidney stones. After collection of all fragments, a 14 F or 16F reentry nephrostomy tube was placed, and then the procedure was terminated.
Unilateral QLB
Block applications were performed after the operation was completed, while the patient was still under general anesthesia. The patient was placed in a lateral decubitus position such that the side for the operation was on top. A convex ultrasound probe (2-6 MHz MyLab30; Esaote, Italy) was placed on the iliac crest and in the transverse position to the posterior axillary line. Subsequently, the L4 vertebral body at the L4 vertebra level, along with the L4 transverse process, the QL, the erector spinae, and the psoas muscle, were identified as the Shamrock sign (Fig. 2). A 21 G (100 mm) peripheral nerve block needle (Quincke SonoPlex Pajunk, Germany) was directed towards the TLF from the posterior aspect of the transducer to the posteromedial anterolateral direction between the psoas muscle and the QL muscle, anterior to the QL muscle [14,15]. After confirming the site by hydrodissection, bupivacaine was injected with a concentration of 20 ml of 0.25% [14,15] (Fig. 2). Twenty minutes after the operation, 8 mg intravenous tenoxicam was administered for postoperative analgesia, and PCA infusion started. Intravenous morphine infusion was administered as a 0.5 mg bolus and 1 mg loading from the solution prepared with PCA (CADD-Legacy® PCA, Smiths Medical, St Paul, USA) at a concentration of 0.4 mg/ml, with a lock time of 20 minutes. Using a cold test, at least 4 dermatomal levels were evaluated for decreased sensory loss compared to a successful contralateral side block at the 30th postoperative minute. If VAS was greater than 4, then 1 g paracetamol (intravenous) was ordered for additional analgesia.

Anterior quadratus lumborum block. A. (A) convex ultrasound probe was placed on the iliac crest and in the transverse position to the posterior axillary line. Subsequently, the L4 vertebral body at the L4 vertebra level, along with the L4 transverse process, the quadratus lumborum, the erector spinae, and the psoas muscle, were identified as the Shamrock sign. (B) 21 G (100 mm) peripheral nerve block needle was directed towards the thoracolumbar fascia—from the posterior aspect of the transducer to the posteromedial anterolateral direction between the psoas muscle and the quadratus lumborum muscle. (C) Local anesthetic was injected after confirming the site by hydrodissection.
QL: quadratus lumborum muscle, PM: psoas muscle, ES: erector spinae muscle, VB: vertebral body, TP: transverse process, PTLF: posterior thoracolumbar fascia, ATLF: anterior thoracolumbar fascia, MTLF: middle thoracolumbar fascia, TLF: thoracolumbar fascia, White arrow: ultrasound visible block needle, White star: injection site. White circle: local anesthetic spread in the QM.
Outcome measures
Primary measures
Primary measurements recorded were the VAS scores (30th min, 2nd, 6th, 12th, and 24th hours post-operation). The patients were informed of the VAS score questionnaire before the operation, and the VAS was explained. The patients marked the level of pain that they felt, using their own hands, on the 10 cm line.
Secondary measures
Secondary measurements recorded were the quantity of cumulated morphine used (at the 2nd, 6th, 12th and 24th hours post-operation), any additional analgesic requirement, side effects such as nausea and vomiting, pruritus, respiratory depression, bradycardia, hypotension, and intraoperative opioid requirement. Further, an investigator, blinded to the patients’ group assignments, evaluated the patients.
Statistical analysis
In addition to the descriptive statistical techniques (frequency, percentage, mean, standard deviation, median, min-max), a chi-square test was used to compare qualitative data in the evaluation of the study data. A Kolmogorov-Smirnov test was used to test the data for normality; and when normal distribution was detected, the Student’s t-test test was used for the inter-group comparisons in this study. Probability (p) values less than α = 0.05 were considered significant and indicative of a difference between the groups. The analysis of the data was performed using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., USA. Released 2013). The primary outcome measure of this study was a 15% reduction in the control group’s VAS scores (7.6 ± 1.26) at 6 hours post-operation [7]. For a study power of 90% (α = 0.05), the calculated, required sample size per group was 27, for a total of 54 patients. In order to increase the power of the study and assuming a 10% participant attrition, 30 patients were planned for each group.
Results
The study was completed with a total of 60 patients. The demographic characteristics of the patients are shown in Table 1. There was no statistically significant difference between the 2 groups for age, BMI, gender, and the amount of opioid given during the operation (Table 1). There was no statistically significant difference in the cumulative morphine usage between the two groups at the 2nd hour (P = 0.09), but statistically significant differences were found between the 2 groups, which was lower in Group B at other measurement times (Table 2). When VAS scores were examined, there were statistically significant differences at all measurement times (P < 0.001) except 30 minutes (P = 0.109) (Table 3). There was no statistically significant difference in the frequency of side effects, consumption of paracetamol as rescue analgesia, and the duration of the operation between the 2 groups (P > 0.05). No complications were found in any of the patients who underwent block (Table 4).

Comparison of the Demographic Characteristics of the Patients
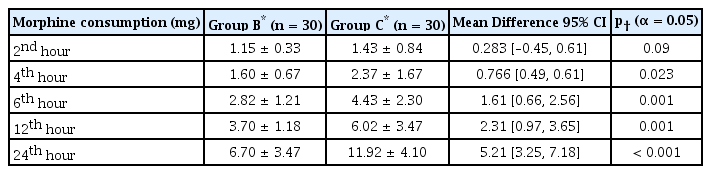
Cumulative Morphine Consumption in the First 24 Hours following Surgery

Comparison of VAS Scores between Groups

Side Effects, Additional Analgesic Requirement, Duration of Surgery (min) and Block Complications
Discussion
After a PNL operation was performed under general anesthesia, we evaluated the efficacy of the anterior QLB group compared to the placebo group. In the QLB group, VAS scores except for the 30th minute postoperative time and morphine consumption except for the 2nd postoperative hour were found to be lower in the other measurement times.
After a PNL operation, postoperative pain, mucosal injury, and inflammation in the renal capsule and collecting system are conducted through sympathetic fibers from the T8-L12 spinal segments, while the sensations of muscle and skin pain are conducted through the intercostal nerves at the T6-T10 level [16]. In the literature, different types of analgesic techniques have been used for PNL operations. Although the intravenous analgesia is the standard technique, regional anesthesia such as a paravertebral block, intercostal block, and nephrostomy tube cannula infiltration have all been used as alternate postoperative analgesia for PNL [2,5,7,17,18].
In the literature, there are studies which successfully used paravertebral block administration for pain palliation. Ak et al. [19], while evaluating postoperative morphine consumption values and VAS scores after the block, found lower opioid use-values. At the time of this study, many other studies have focused on fascial plane blocks that may be an alternative to neuraxial blocks [8-12]. QLB is also a recently used facial plane block in several types of surgical procedures and for which proper indications must still be determined. This block, which initially was used for postoperative pain control after abdominal surgery, has now been used in various operations such as distal lower extremity surgery and nephrectomy pain.
It was reported that QLB block provides analgesia on the lateral and anterior abdominal wall after two different versions of the block were described by Blanco and McDonnell with injection types administered to the QLBI and QLBII of the QL muscle. Afterward, QLBIII was described as an alternative route using a local anesthetic injection administered between the QL and the psoas muscle [14]. The literature information includes clinical studies, cadaver studies, and case reports for different types of QLB block administration [14,20-22].
In studies designed as RCT, Blanco et al. [10,11] used QLB for pain control after cesarean operations in two different studies. In their study with the placebo group, they found less morphine consumption in the QLBI (type 1) group, while in their other study, they compared the results of patients who received QLBII (type II) with those who received a TAP block. In the results of this study, they reported that they provided less morphine consumption and more prolonged analgesia in patients receiving QLB. In another study of a pediatric patient group, Öksüz et al. found a decrease in the requirement for rescue analgesia after a posterior QLB block [23].
In a series of 22 patients who received a subcostal anterior QLB block after upper urinary system operations, dermatomal spread and VAS scores were reported. The mean VAS scores of the patients who had a follow-up for 3 days were 3.7 on the 1st day (Range 4 to 5, on a 1–10 scale). The authors of that report opined that these values might be due to previous chronic pain in 3 patients [24]. In our study results, it is remarkable that the mean VAS scores of the group treated with a block were lower than in that earlier study. However, a different type of surgery and relatively less invasive PNL procedures may change the results. The reported results of 1 pediatric and 3 adult patients who received the block for analgesia after open kidney surgery suggest that an anterior QLB block provides successful analgesia [25-27].
Although the studies suggest that QLB provides successful analgesia, there are still unclear issues regarding the block. The first one seems to be the amount of local anesthetic administered. Some studies achieved successful block results after the administration of local anesthetics at doses of 20-30 ml [10-11,24-27]. The amount of local anesthetic that we used (20 ml) achieved a lower VAS score in postoperative pain and lowered morphine consumption values compared to the control group. The other two important points are sensory block level and the mechanism by which the local anesthetic drugs acts. The mechanism of action has been focused on for ganglion blockade, sympathetic block, and paravertebral spread [28,29]. In the literature, there are many predictions that drugs administered to the fascial plane may lead to variations in the spread due to biomechanical effects. However, it is also emphasized that there are unresolved indications that use of anesthetized, administration of muscle relaxant, and block administration position may affect the spread.
Further, the data obtained in our study results were not sufficient to discuss the sensory block and mechanism of action. Complications that may arise because of an anterior QLB block depend on the technique and the amount of local anesthetic administered. Technically, full visualization of the needle tip during the injection is essential due to the closeness of the administration site to the abdominal structures. Since the frequency of using local anesthesia is higher than peripheral nerve block administration, it has been reported that this may cause potential local anesthetic systemic toxicity (LAST) related complications due to systemic absorption [30]. Although it was found that local anesthetic levels after QLB did not reach a toxic dose, we think that further studies are needed to quantify the potential risk [21]. In this study, we administered 20 ml local anesthetics and unilateral block resulting in no clinical occurrences of LAST.
A case report and a study presented in the literature, reported weakness in the lower extremity on the block administration side [22,31]. In the study by Okmen et al. [22], it was found that pneumoperitoneum established during laparoscopic cholecystectomy might cause this weakness by increasing the drug spread. We found no weakness in the lower extremities and no other complications in patients included in this study who received a block. Lower local anesthetic dose compared to other studies might be a factor.
Limitations of this study are that sensory block level ranges and the block time could not be monitored after block administration, the patients’ follow-up was limited to 24 hours, and the amount of opioid use during the operation varied depending on the patients' weights (despite attempting to standardize).
The results of this study demonstrate that anterior QLB administered for pain after PNL may be an effective analgesia technique. Determining the analgesic level and duration of action of the block are important opportunities for future research.
Notes
No potential conflict of interest relevant to this article was reported.
Author Contributions
Korgün Ökmen (Investigation; Conceptualization; Supervision; Data curation; Writing–original draft; Methodology)
Burcu Metin Ökmen (Formal analysis; Supervision; Writing–review & editing)