Development of the Geop-Pain questionnaire for multidisciplinary assessment of pain sensitivity
Article information
Abstract
Background
To assess the multidisciplinary aspects of pain, various self-rating questionnaires have been developed, but there have not been sufficient relevant studies on this topic in South Korea. The aim of this study was to develop a new pain sensitivity-related questionnaire in the Korean language that would be simple and would well reflect Koreans' senses.
Methods
A new pain assessment questionnaire was developed through a pre-survey on "geop", which is the Korean word expressing fear, anxiety, or catastrophizing. We named the new assessment questionnaire the Geop-Pain Questionnaire (GPQ). The GPQ was composed of 15 items divided into three categories and rated on a 5-point scale. As a preliminary study, internal consistency and test-retest reliability analyses were conducted. Subsequently, 109 individuals completed the GPQ along with three pain-related questionnaires translated into Korean (Pain Sensitivity Questionnaire [PSQ], Pain Anxiety Symptoms Scale [PASS], and Pain Catastrophizing Scale [PCS]), and the correlations were analyzed.
Results
All items in the GPQ showed appropriate internal consistency, and the test-retest reliability analysis showed no statistically significant differences. The correlations between the GPQ and the existing questionnaires revealed that the GPQ scores had mid-positive correlations with the PSQ scores and strong positive correlations with the PASS and PCS scores.
Conclusions
This study attempted to develop a questionnaire assessing pain sensitivity multidimensionally using the Korean word geop for the first time. The self-rating GPQ showed high correlations with the existing questionnaires and demonstrated potential to be utilized as a pain prediction index in clinical practice.
Introduction
Pain assessment is very important for the accurate assessment of the conditions of patients with pain, as well as for their proper treatment. Pain, however, is a sensory and emotionally unpleasant subjective experience [1] and, in addition to simple tissue damage, has associations with various elements, including the patient's personal emotions, cultural background, past experiences, and socioeconomic environment. Thus, it is difficult to determine the criteria that can be used for definitively assessing pain. If a patient's level of pain sensitivity can be determined, then, based on this sensitivity level, the degree of pain that will be felt by the patient during surgery can be predicted prior to the surgery and an appropriate strategy for individual pain control will be possible. Additionally, this knowledge will be very helpful in the treatment of patients with chronic pain.
In pursuit of methods of pain assessment that will accurately reflect its complex characteristics, many studies have been performed to predict the level of pain sensitivity or to develop questionnaire surveys related to pain, but no significant achievements have been accomplished. Along with the continuous conduct of experimental studies measuring the level of sensitivity and diversity of individuals through the delivery of a pain stimulus [23], the development of self-rating questionnaires is continuously being attempted [4567]. Questionnaire surveys are one of the methods of assessing the pain felt by an individual in multidimensional aspects, and these have been diversely conducted since the first administration of a survey using the McGill Pain Questionnaire (MPQ), which assesses the intensity of pain. Multidimensional questionnaires of this type include the Pain Sensitivity Questionnaire (PSQ) [6], Pain Catastrophizing Scale, (PCS) [5], Pain Anxiety Symptoms Scale (PASS) [8], and Fear-of-Pain Questionnaire (FOPQ) [9], among others.
Compared to the international research, however, the relevant studies that have been performed in South Korea have been far from diverse, and in particular, multidimensional questionnaire surveys useful in the assessment of various types of neuropathic pain or other chronic diseases have not been widely conducted. The reasons for this are as follows. First, there is no existing Korean questionnaire that appropriately assesses the subjective thinking and feelings of the Korean patients. As with the MPQ, PCS, and PSQ, most of the questionnaires that are currently in use in South Korea were developed overseas and began to be employed after undergoing translation and certification processes [1011], but South Koreans' social, economic, and cultural environments are fundamentally different from those found overseas. The second reason is the nature of the South Korean healthcare environment. Visual and objective tests such as ultrasound or magnetic resonance imaging (MRI) are preferred to subjective questionnaire surveys, which are unfamiliar in the South Korean healthcare environment, in which the treatment hours are not sufficient. Furthermore, as the patients are reluctant to provide responses to the questionnaire items, and many of the patients with chronic pain are elderly, there are obstacles, such as difficulty in conveying the contents of the questionnaire items. Therefore, there is a need to develop a questionnaire that can be administered simply, completed in a short time, consist of accessible items, and has a strong association with pain.
The pain questionnaires suggested above utilize terms such as fear, anxiety, and catastrophizing, but South Koreans commonly use the word "geop" when they recall the pain-related term. The word geop means fearful heart or psychological tendency, and its synonyms include horror, fear, fright, hesitation. That is, the meaning of geop is thought to be similar to fear, anxiety, avoidance, catastrophizing. Additionally, South Koreans are believed to have a high understanding of the dictionary meaning and concept of geop.
Therefore, this study aimed to develop a multidimensional questionnaire that can predict the level of a patient's pain sensitivity and that is easy to understand and well reflects South Koreans' feelings and emotions, instead of using an existing questionnaire that was developed overseas and utilized after going through translation and certification processes. In addition, the correlation between the level of geop and the occurrence of pain was investigated.
Materials and Methods
This study was approved by the Institutional Review Board. It was conducted targeting patients and their caregivers aged older than 20 years who visited a hospital. The study subjects were volunteers with sufficient knowledge of Korean, with no restrictions in filling out the questionnaire, with the ability to voluntarily communicate and seamlessly express what they want to express, and with no special disease. In the pre-survey for questionnaire item development, there were 80 volunteer participants; the preliminary study for verifying the validity of the questionnaire targeted 40 volunteers; and the main study was conducted with 120 volunteer participants. Prior to the surveys, it was sufficiently explained to the study subjects that the aim of the study was to investigate individuals' thoughts and feelings on the association between geop and pain. Participants were instructed to ask questions if they encountered questionnaire items that were difficult to understand while filling out the GPQ.
Pre-survey
The purpose of this study was to develop a questionnaire on the association between geop and pain using the Korean word geop for the first time. Thus, initial items relating to geop were created, and an initial survey was performed to organize the concept of geop. After confirming that the 80 study participants understood the concept of geop, they were asked to write about the situations in which they most strongly experienced geop.
Development of the Geop-Pain questionnaire (GPQ)
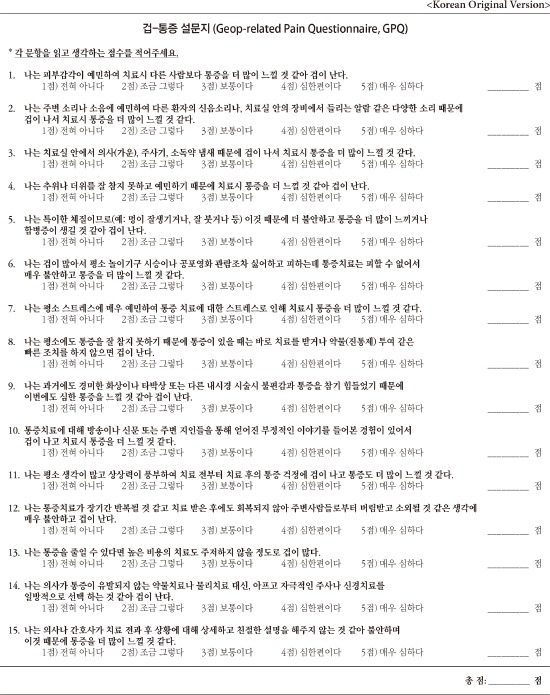
Referring to the data collected from the pre-survey as well as the existing questionnaires, a preliminary questionnaire reflecting various factors related to pain was created. The questionnaire was divided into three dimensions (sense, experience, and "other"), with the other dimension consisting of catastrophizing and socioeconomic environmental factors. Each dimension included five items, and consequently, the questionnaire had a total of 15 items. Items 1 to 5, belonging to the sense dimension for geop, were related to the differences in the senses (e.g., vision, hearing); items 6 to 10, belonging to the experience dimension for geop, were related to geop after experiencing fear or pain; and items 11 to 15, belonging to other dimension for geop, were items in which exaggerated thinking, a victim mentality, a sense of alienation, and cost were associated with geop. For each item, unrealistic elements were eliminated from the geop-inducing situations expressed by the participants in the first survey, and only the episodes that were both associated with pain and commonly occur in everyday life were used. After completion of the questionnaire, it was reviewed by two pain specialists. The scores that were given as responses to the questionnaire items ranged from 1 (not at all) to 5 (very severe).
Internal consistency and test-retest reliability analyses
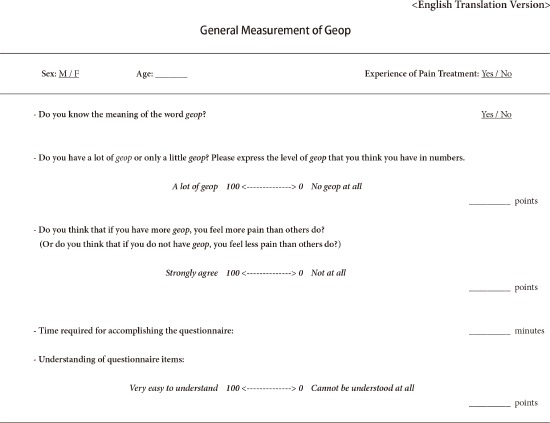
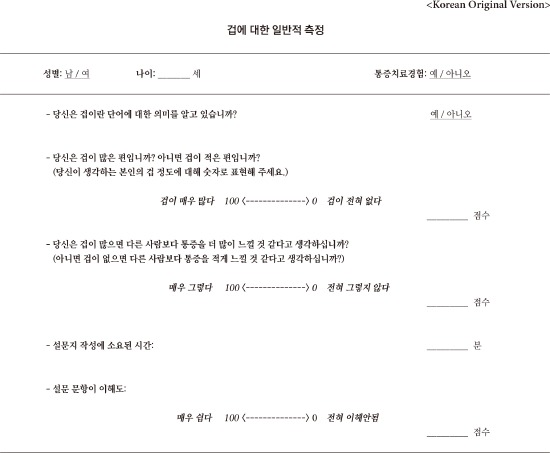
The first preliminary study was conducted targeting 40 volunteers, and after three weeks, the second preliminary study was conducted using the same questionnaire. Excluding three participants who could not be involved in the second preliminary study and two participants whose data were partially omitted, the data of 35 participants were utilized for analyses. Using the data gathered from the two preliminary studies, to determine the degree of homogeneity among the questionnaire items belonging to the same dimension (sense, experience, other), the validity of the items was analyzed, and to determine if the respondents' answers to the questionnaire items were consistent, the reliability of the answers was analyzed. For the test-retest reliability, the first and second preliminary study data were compared. After the preliminary studies, the final questionnaire was named the "Geop-Pain Questionnaire (GPQ)" (Appendix 1). In addition, to investigate the basic characteristics of the study participants and their thoughts on geop and pain, a questionnaire for the general measurement of geop (Appendix 2) including items on sex, age, pain treatment experience, level of geop, and degree of Geop-Pain association was administered during the preliminary studies and the main study, along with the GPQ. In the questionnaire, the participants were asked to express the level of geop they believed they had (level of self-rating geop) and whether they thought geop was associated with pain (Geop-Pain association) in numbers ranging from 0 to 100.
Main study
The purpose of the main study was to verify whether the GPQ could be used clinically. Targeting 120 volunteers, the GPQ was administered along with the PSQ, PASS-20, and PCS, and following the exclusion of 11 respondents with partially omitted records in their completed questionnaires, the data of 109 individuals were finally analyzed. To identify the correlations between the GPQ and the three existing questionnaires, first, the correlations between the total score on the GPQ and those on the three existing questionnaires were analyzed. Additionally, the correlations of the three dimensions of the GPQ (sense, experience, and other) with the PSQ, PASS-20, and PCS were analyzed. Moreover, the correlations between the GPQ score with the level of self-rated geop and the Geop-Pain association score were analyzed.
Statistical analysis
Statistical analyses were performed using SPSS (Windows ver. 14.0, SPSS Inc., Chicago, IL, USA). For the continuous variable, mean ± standard deviation was used, and for the categorical variables, frequency and percentage (%) were utilized. Internal consistency (IC) was used to verify the validity of the items, and Cronbach's alpha was utilized as an index for reliability. The IC was assessed to be appropriate if it was higher than 0.3, and Cronbach's alpha, if it was higher than 0.7. The test-retest reliability was analyzed using the paired t-test. Based on the data obtained from the main study, factor analysis was performed to determine whether each item in the GPQ was well distributed to the three dimensions. Using principal component analysis (PCA) applying varimax rotation, the dimensions were constructed by binding the items with higher factor loading. In addition, the variances explained by each dimension were calculated. To analyze the correlations with the scores in the three existing questionnaires, Spearman's rank correlation was employed. For the correlations of the GPQ score with the level of self-rated geop and the Geop-Pain association score, the multiple linear regression model was applied, and adjusting the age, sex, and pain treatment experience, the regression coefficients were estimated. As the range of the score of each dimension in the GPQ is different from that of the total score, using the sizes of the standardized coefficient beta, their linear relationships with the scores of the three pain questionnaires were compared. All statistical analysis results were determined to be significant when P < 0.05.
Results
The data that were collected from the first survey for questionnaire item development were classified by type (Table 1). The general characteristics of the participants, the time required for accomplishing the questionnaire, the level of geop, and the Geop-Pain association are presented in Table 2. The proportion of males was greater than that of females, and the 20–30-year-old age group was the largest. In the preliminary and main studies, 22 (62.9%) and 80 (73.4%) respondents, respectively, had an experience of pain treatment. The mean self-rated geop scores were 58.3 ± 20.2 and 57.4 ± 19.9, respectively; the standard deviation was high, about 19–20; and the range of the self-rated geop score was 35–80, showing that the scores were widely distributed. For the Geop-Pain association, the scores were 66.4 ± 23.6 and 63.1 ± 23.9, respectively, indicating that the scores were widely distributed between 40 and 80, with a large standard deviation, as with the level of self-rated geop score. The time required for accomplishing the questionnaire was almost the same in both cases (5.9 ± 4.2 and 5.6 ± 3.8 minutes, respectively), and the mean of the values representing the respondent's understanding of the questionnaire items were 79.4 ± 18.1 and 80.8 ± 17.0, respectively.

Pre-survey for Geop

Characteristics of the Study Population
In the analysis results regarding the IC of the GPQ using the data obtained from the preliminary study targeting 35 individuals, Cronbach's alpha was higher than 0.7 in all three dimensions (sense, experience, and other), which was appropriate (Table 3). The reliability was also very high in all the dimensions and in the total score on the GPQ, showing that the preliminary questionnaire well reflected the respondent's consistent response. As the results of the test-retest in which the tests were given twice using the same questionnaire did not show a statistically significant difference (Table 4), the GPQ was evaluated to be an instrument that could obtain consistent responses. Therefore, without any amendments to the questionnaire items, the main study was conducted.
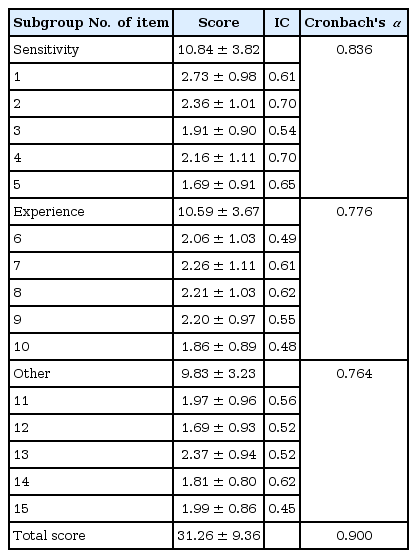
Internal Consistency of Geop-Pain Questionnaire (N = 35)

Test-retest Reliability for Geop-Pain Questionnaire (N = 35)
In the main study targeting 109 subjects, as a result of the factor analysis, it was confirmed that each item of the GPQ was well arranged in the three dimensions (Table 5). Between the PSQ score representing the level of pain sensitivity and the GPQ score of each dimension and the total GPQ score, there were statistically significant mid-positive correlations, ranging from 0.2 to 0.3 (sense, r = 0.296; experience, r = 0.242; other, r = 0.237; total, r = 0.294). Among the three dimensions, the sense dimension had the strongest correlation with the PSQ (Fig 1, Table 6). Between the PASS-20 score investigating the association between anxiety and pain and the GPQ score of each dimension and the total GPQ score, there were statistically significant strong positive correlations, ranging from 0.55 to 0.65 (sense, r = 0.553; experience, r = 0.625; other, r = 0.587; total, r = 0.647). Among the three dimensions, the experience dimension had the strongest correlation with the PASS-20 (Table 6).

Factor Analysis for Explained Variance and Factor Loading for the Measurement Variables

Scatter Plot of GPQ Scores and the Other Questionnaires. Score 1: sensitivity, 2: experience, 3: other. GPQ: Geop-Pain Questionnaire, PSQ: Pain Sensitivity Questionnaire, PASS: Pain Anxiety Symptoms Scale, PCS: Pain Catastrophizing Scale.
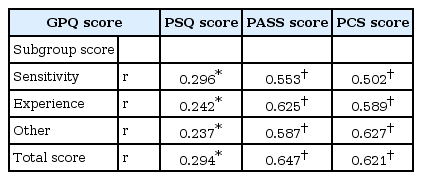
Correlation between GPQ and the Other Questionnaires
Between the PCS, which measures the degree of catastrophizing pain, and the GPQ score of each dimension and the total GPQ score, there were statistically significant strong positive correlations, ranging from 0.50 to 0.63 (sense, r = 0.502; experience, r = 0.589; other, r = 0.627; total, r = 0.621). Among the three dimensions, the other dimension, including catastrophizing and socioeconomic environments, had the strongest correlation with the PCS (Table 6). The scores of all three dimensions showed positive correlations with the self-rated geop score, and the standardized coefficients (beta) of all the dimensions were significant (Table 7). Likewise, the Geop-Pain association score showed statistically significant associations with the GPQ scores of the sense and experience dimensions and the total GPQ score, and the standardized coefficients were very large. Although the catastrophizing and external dimension had a positive correlation with Geop-Pain association, their relationship was not statistically significant (P = 0.095) (Table 7).

Linear Regression for Self-rating on Geop and Subjective Rating on the Relation of Geop and Pain
Discussion
In the past decades, many studies have attempted to assess the level of a person's pain sensitivity using a multidimensional approach. To experimentally measure and evaluate the diversity of pain perception between individuals, stimulations with various properties, such as thermal, mechanical, ischemic, and electronic stimulations, have been used [61213]. The experimental pain assessment methods, however, are limited by the equipment, time, and relevant cost, and most of all, may induce serious discomfort and pain in the individuals whose levels of pain sensitivity are being assessed. As such, practical methods that can replace the experimental assessment methods and can evaluate subjective experiences related to pain have been suggested. Among these methods are many self-rating questionnaires, and questionnaire surveys connecting various factors (e.g., fear, anxiety, sensitivity, catastrophizing, vigilance and awareness) with pain and grading them have been attempted [4567814].
In the Eastern social and cultural environments, where people do not usually express themselves actively, self-rating questionnaires have not yet been widely used. In South Korea, self-rating questionnaires are clinically used primarily for academic purposes. One of the reasons for this is that it is not easy to find a pain-related questionnaire that was developed in South Korea. As for the MPQ, one of the few multidimensional pain questionnaires in use in South Korea, Diller [15] argued that if it were used in non-English-speaking areas, the words in the items could be interpreted differently from their dictionary definitions and might lose their original meanings. Kim et al. [16] stated that pain has various dimensions and that the expression of pain using one's native language is important; thus, they developed various pain terminology measurement cards in Korean. Additionally, using the concept of geop for the first time, by grading geop like the Numeric Rating Scale (NRS) and comparing its grade with the results obtained from the existing pain questionnaires, the authors reported that geop was statistically significantly correlated with pain [17]. They also mentioned, however, that their study was an exploratory study for identifying the tendency between geop and pain, and that further studies were required to make the NRS of geop one of the indicators of pain perception.
In this aspect, the first purpose of the current study was to develop a Geop-Pain questionnaire for the first time, with the goal of determining the level of a person's pain sensitivity by connecting the various meanings and conceptions of the Korean word geop with pain. Another important purpose of this study was to determine whether a change in the degree of pain felt by a patient could be predicted depending on the level of geop. In this study, it was most important to ensure that the participants' thoughts and feelings about geop were correctly and consistently reflected in the GPQ, expressed as specific sentences. Accordingly, to develop new questionnaire items instead of using the translated ones, before constructing the items, various thoughts on geop were researched, and based on the research results, efforts were made to ensure that the formulated questionnaire items could be easily and correctly understood, by using more familiar expressions. In the preliminary studies performed prior to the main study, the test-retest reliability was high in all the dimensions, showing that the respondents' consistent responses were well reflected (Tables 3 and 4).
In the main study, the GPQ was diversely compared with three pain-related questionnaires used after translation and certification, and because they showed strong correlations, the potential of the GPQ as a new questionnaire could be confirmed. However, the FOPQ [9] being used in studies for questionnaire development in the dentistry and traditional-Korean-medicine areas (mainly acupuncture), with very similar pain treatments, exploring the idea that the anxiety and fear felt before the treatment might affect the degree of pain felt after the treatment, was not included in this study because the validity of the FOPQ has not been proven in South Korea. It is believed, however, that it is necessary to compare this questionnaire with the GPQ in the future.
The current study intended to develop a Geop-Pain questionnaire that maximally reflects the components of the existing pain-related questionnaires based on the definition of "pain". For this reason, the questionnaire was divided into three subdimensions, and not only the GPQ as a whole but also the subdimensions of the GPQ were compared with the existing questionnaires. The difference in actual feelings or sensitivity, one of the indicators of diversity between individuals, may cause a change in geop and pain. Ruscheweyh et al. [67] stated that a great difference in the level of pain sensitivity was shown between individuals, and that pain sensitivity could be a risk factor progressing to chronic-pain disease; thus, its assessment is very important. Moreover, as a useful method of measuring an individual's pain sensitivity, the authors developed the PSQ, a self-rating questionnaire examining the intensity of pain expected to be felt when certain body parts are injured, by assuming various pain situations that may occur in everyday life.
In this study, GPQ items 1 to 5 were intended to reflect sense-related geop, and its correlation with the PSQ emphasizing the sensory parts explaining pain sensitivity was analyzed. Among the subdimensions of the GPQ, the sense dimension was confirmed to show the strongest correlation with the PSQ. Meanwhile, in cases when a person has undergone a painful and fearful experience such as receiving root canal treatment at a dental clinic, at the next treatment, the geop increases, and for the same treatment, the person feels more pain, and the pain can further increase. Conversely, if a person has a vague fear of pain, after going through an adaptation process or after directly experiencing the pain, the fear is eliminated, and the person may feel less pain at the next treatment [18].
For the PASS, which consists of 40 items in the four dimensions of cognitive factor, escape/avoidance factor, fear factor, and physiological anxiety, the stability, reliability, and convenience of the questionnaire have been verified in clinical practice and in the research field, among many methods measuring anxiety by associating it with pain, and it is widely used [19]. The PASS-20 is a short form of the PASS, with 40 items [8]. To reflect avoidance or a cognitive change, or anxiety through experience, items 6 to 10 in the GPQ were related to experience, and the correlation with the PASS-20 was analyzed. The PASS-20 revealed strong positive correlations with all dimensions of the GPQ and the total score on the GPQ, and the experience dimension of the GPQ had the strongest correlation with the PASS-20 (Table 6).
Lastly, items 11 to 15 in the GPQ were regarding exaggeration, catastrophizing, and socioeconomic factors, and reflected Geop-Pain association. Catastrophizing, conceptualized by Rosenstiel and Keefe [20], means that the negative cognitions of noxious stimuli are amplified, and as the negative aspects of the pain situation are focused on too much or are worried about, a person expects only negative results and consequently develops a feeling of helplessness, to the extent that he or she is unable to cope with the pain. The PCS was developed in 1995 by Sullivan et al. [5] to assess the degree of catastrophic thinking with regard to pain, and they stated that catastrophizing is an important psychological construct evaluating a person's thoughts and feelings when he or she is in pain, and adjusting the person's behavioral responses to pain. Moreover, Sullivan et al. [21] defined catastrophizing as an exaggerated negative feeling imposed while actual or expected pain experiences appear. The PCS consists of subscales, including rumination, magnification, and helplessness, and is widely used in assessing pain-related catastrophizing. The PCS is currently in use in South Korea as its translation and certification have been completed [22]. Items 11 to 15 in the GPQ were intended to reflect catastrophizing, and the external factors showed the strongest correlation with the PCS among all dimensions of the GPQ (Table 6). On the other hand, in the comparisons of the total GPQ score and the total scores in the other questionnaires, the PASS-20 and the PCS were found to have stronger correlations with the GPQ compared to the PSQ. The present study showed that the total GPQ score and the subdimensions were highly associated with the existing three questionnaires. In particular, as intended when developing the questionnaire, between the sense dimension of the GPQ and the PSQ, the experience dimension and the PASS-20, and the catastrophizing and external dimension and the PCS, there were strong correlations, which means that the GPQ has potential to become a new pain-related questionnaire that can be applied to clinical practice.
To examine the second purpose of this study, the influence of the level of geop on pain, the associations of the self-rated geop and Geop-Pain association with each dimension of the GPQ and the total GPQ score were analyzed (Table 7). The level of geop was significantly associated with the GPQ scores, and the Geop-Pain association score for investigating the participant's perception of Geop-Pain association was also significantly associated with the subdimensions of the GPQ and the total GPQ score. That is, the study participants thought that if they had more geop, they would feel more pain. In this study, however, the number of participants in their 20s was greater than the number of participants in the other age groups, and in terms of sex, there were slightly more females than males, which could pose a problem in generalizing the study results.
The simple dictionary meaning of geop may sound somewhat different from that of stress, but thinking in relation to pain, geop can be assumed to act as a stressor to patients. The influence of stress on pain has been reported in many studies, and the results were revealed in two different patterns. In an animal experiment using mice, Quintero et al. [23] explained that due to the reduction and delay of gamma-aminobutyric acid inhibitory control, which is involved in the activation of the post-synaptic N-methyl-D-aspartic acid receptor, pain hypersensitivity occurred due to stress. Martenson et al. [24] argued that as in their study, the pain-inducing neurons were activated by the activation of stress-related circuits located in the hypothalamus, and pain sensitivity occurred. Donello et al. [25] mentioned that in an experimental study in which repetitive stress stimuli were given, pain sensitivity was caused by the sympathetic nervous system in association with peripheral adrenergic receptors.
Contrary to the aforementioned claims, however, Carrive et al. [26] have also reported that repetitive stress reduced pain. If a person persistently experiences stress due to pain, the pain will be reduced due to the adaptation process and to the increase of the pain threshold. These contradictory results seem to be due to the fact that the influence of the emotional elements on pain has a complex and multidimensional structure. In the case of the initial experience or occurrence of anxiety or fear, when there are repetitive stimulations, the pain is reduced, but individuals experiencing unresolved persistent anxiety become more sensitive to pain [18]. Additionally, as in the results of a study in which the pain thresholds due to a noise stimulus were compared between males and females, within the same environments, different results may be generated depending on the sex, age, and various other factors of the study subjects [27].
Thus, the level of a patient's pain sensitivity can be predicted by conducting a pre-assessment, such as with the GPQ, before performing surgery or a procedure, and if the factors increasing pain sensitivity and stress can be eliminated, the GPQ can be a useful instrument for reducing pain. In recent years, with regard to the prediction of postoperative pain, many studies have reported that a patient's postoperative pain can be reduced by predicting the risk factors related to pain, which differ from one person to another, before surgery. Werner et al. [28] reported that the degree of pain perception of a preoperative patient was correlated with the degree of the patient's postoperative pain in experimental methods using pain stimuli. Additionally, in another study targeting 85 pregnant women scheduled to undergo cesarean section, the pregnant women who received a sufficient explanation of the procedure they were to undergo from an anesthetist before the surgery, and who were emotionally supported by their spouses, became less anxious, obtained greater postoperative satisfaction, and recovered rapidly [29]. Although it is not a predictor of pain, distraction, which reduces pain by decreasing the sensory and psychological factors, has also received attention. In children and adolescents, who may feel more pain than that which is actually produced by the stimulation that they receive due to their severe anxiety and fear of injection, the use of distraction, which disperses and offsets the psychological factors, can reduce the occurrence of pain [30]. The limitations of the current study include the small sample size and the fact that the experimental methods were not used together. Therefore, further studies targeting more diverse age groups or various patient groups, such as patients waiting for surgery or dental or patients receiving pain treatment, will be conducted, with a larger sample size. Additionally, based on the results obtained from this survey, as reported by Rhudy et al. [1227] or Ruscheweyh et al. [67], diverse additional investigations regarding pain perception by individuals are necessary, through the analysis of the associations between self-rating questionnaires and experimental methods performing experiments using cold, heat, noise, and electronic stimulations.
In conclusion, to predict complex pain in multidimensional aspects, a self-rating questionnaire that is easy to understand and that well reflects the condition of the patient must be formulated. As such, this study first attempted to develop a new questionnaire using the Korean word geop instead of using translated questionnaires. As a result, the potential of the newly developed questionnaire for use as a pain prediction index in clinical practice was demonstrated as it showed high correlations with the existing questionnaires. Moreover, it was revealed that if the study subjects had more geop, they believed that they would feel more pain, and it was confirmed that the level of geop could be used as a predictor of pain.
Notes
This is a thesis for a Doctor's degree by Sung-Hwan Cho.
Appendices
Appendix 1
Geop-Pain Questionnaire

Appendix 2
Survey of Geop Score and Geop-Pain Scale