The effects on Apgar scores and neonatal outcomes of switching from a combination of phenylephrine and ephedrine to phenylephrine alone as a prophylactic vasopressor during spinal anesthesia for cesarean section
Article information
Abstract
Background
Ephedrine, unlike phenylephrine, has a dose-related propensity to depress fetal pH during spinal anesthesia during cesarean section. A low arterial umbilical cord pH has a strong association with neonatal mortality and morbidity. The purpose of this retrospective study was to investigate influences of vasopressor change on Apgar scores and adverse neonatal outcomes in cesarean section.
Methods
In obstetric anesthesia, we changed the prophylactic vasopressor from a combination of phenylephrine and ephedrine to phenylephrine alone in 2000. We evaluated the impact of vasopressor change on Apgar scores (1 and 5 min), incidence of Apgar score < 7 (1 and 5 min), neonatal seizure, continuous positive airway pressure (CPAP), intermittent positive pressure ventilation (IPPV), intraventricular hemorrhage (IVH), periventricular leucomalacia (PVL), and hypoxic ischemic encephalopathy (HIE) in low-risk elective cesarean sections during a period when the combination of phenylephrine and ephedrine was used (2008-2009, two years) and the period of phenylephrine use alone (2011-2012, two years).
Results
There were no differences in Apgar scores (1 and 5 min), the incidence of 5 min Apgar score < 7, neonatal seizure, CPAP, IPPV, IVH, PVL, and HIE between the two time periods. However, the incidence of 1 min Apgar < 7 was decreased during the period of phenylephrine use compared with the period of phenylephrine and ephedrine use (P = 0.002).
Conclusions
Conversion from a combination of phenylephrine and ephedrine to phenylephrine alone as a prophylactic anti-hypotensive drug during spinal anesthesia for cesarean section in low-risk pregnancy may be associated with a significant decrease in the incidence of 1 min Apgar < 7.
Introduction
Hypotension is one of common complications in spinal anesthesia for cesarean section. The use of uterine displacement and volume preloading cannot effectively prevent hypotension after spinal anesthesia [1,2]. Therefore, a vasopressor, such as ephedrine or phenylephrine, may be necessary to prevent and treat hypotension. Conventionally, ephedrine was the drug of choice for hypotension during spinal anesthesia for cesarean section. However, a number of studies have suggested ephedrine has a dose-related propensity to depress fetal pH and base excess (BE) in comparison to phenylephrine [3,4,5]. In addition, umbilical artery pH in a combination group of phenylephrine and ephedrine was lower than that of phenylephrine alone group [6,7]. When diverse combinations of phenylephrine and ephedrine were infused to maintain arterial blood pressure during spinal anesthesia for cesarean section, as the proportion of phenylephrine decreased and the proportion of ephedrine increased, decreases were observed in fetal pH, BE and umbilical arterial oxygen content [7]. Fetal acidosis identified by umbilical artery pH in spinal anesthesia for cesarean section is mainly the result of metabolic acidosis with low BE [7,8,9,10]. The metabolic component of acidosis could contribute to the increased risk of adverse outcomes instead of the respiratory component [7,8,9,10].
There is no study about impact of vasopressors on Apgar scores and neonatal outcomes in a large population base. We therefore used a large patient population with low-risk pregnancies to further delineate the impact of vasopressor changes in elective cesarean section on Apgar scores and neonatal outcomes.
Materials and Methods
For obstetric anesthesia, we switched from using a combination of phenylephrine and ephedrine to phenylephrine alone as a prophylactic vasopressor for cesarean sections in 2010. We conducted a retrospective cohort study in our hospital for two time periods, from 2008-2009 and 2011-2012. The study was reviewed and approved by our hospital's Institutional Review Board. We extracted data from the anesthetic, obstetric, operational and neonatal records, including the database of the neonatal intensive care unit. In all, 11,078 cesarean sections were done during the study period (2945 in 2008, 2674 in 2009, 2730 in 2011, and 2729 in 2012).
For the current analysis, we selected elective cesarean sections by spinal anesthesia in mothers who experienced no labor pain before anesthesia and who had a maternal age between 19 and 44 years, a full-term pregnancy (≥ 37 week's gestation), and infants weighing ≥ 2,500 g without any known fetal anomalies. We also included cesarean sections indicated for a previous section, breech presentation, transverse lie presentation, cephalopelvic disproportion, and surgery scarring. We excluded cases in which spinal anesthesia was converted to mask or general anesthesia or those where any sedative was administered before the delivery of the newborn. We also excluded cesarean sections with indications of twins, myoma in the uterus, intrauterine growth retardation, oligohydroamnios, and placenta previa. Mothers with hypertension (including pregnancy-induced hypertension), diabetes mellitus (including gestational diabetes mellitus), cardiovascular, cerebrovascular, respiratory, or renal disease or those who were American Society of Anesthesiologists physical status III or greater were also excluded.
Patients were not premedicated, and they received lactated Ringer's solution at the full rate upon entering the operating room. Standard noninvasive monitoring was applied. We allowed the patients to rest undisturbed in the supine position for several minutes while their blood pressure (BP) was measured at least twice every minute to establish a baseline. Spinal anesthesia was administered with the patients in the left lateral position at the L3-4 or L4-5 vertebral interspace, and 0.5% hyperbaric bupivacaine 10 mg and fentanyl 15 µg were injected intrathecally using a 25-gauge pencil point needle (Pencan®, B/Braun, Melsungen, Germany). After spinal anesthesia, phenylephrine (Phenylephrine HCl®; Hana Pharmaceuticals, Seoul, Korea) and ephedrine (Ephedrine HCl®; Daewon Pharmaceuticals, Seoul, Korea) were infused at a rate of 25 µg/min and at a rate of 2 mg/min, respectively, in 2008-2009 (Group P+E). Instead of phenylephrine and ephedrine, phenylephrine alone was infused at a rate of 50 µg/min in 2011-2012 (Group P). We checked patients' BP and heart rate (HR) at 1-min intervals until delivery. If the systolic blood pressure (SBP) was above the baseline, the infusion was stopped; if it was at or below the baseline, the infusion was continued. Hypotension, defined as a SBP ≤ 80% of baseline SBP despite the phenylephrine infusion, was treated with a bolus of phenylephrine 100 µg. Bradycardia was defined as HR < 50 beats/min and was treated with glycopyrrolate 0.2 mg. After delivery, Apgar scores at 1 and 5 min were measured by an anesthesiology specialist or by 2nd-year or higher residents.
We compared the Apgar scores and neonatal outcomes in both groups during the two time periods (Group P+E; 2008-2009, Group P; 2011-2012). Data were expressed as mean ± SD, median (interquartile range) or number of patients (%). Demographic data were analyzed using Student's t-test after the Kolmogorov-Smirnov normality test. Apgar scores were analyzed with MannWhitney U test. A comparison of the categorical variables was performed using χ2 analysis. The relative risk and 95% confidence intervals were calculated when appropriate. Statistical analyses were performed with SigmaStat version 4.0 (San Jose, CA, USA). P values < 0.05 were considered statistically significant.
Results
Baseline and obstetric characteristics of the study population are listed in Table 1. There were no statistically significant differences in maternal height, maternal weight, birth weight, gestational age, and incidence of a nuchal cord. However, the maternal age of Group P+E was lower than that of Group P (P < 0.001).
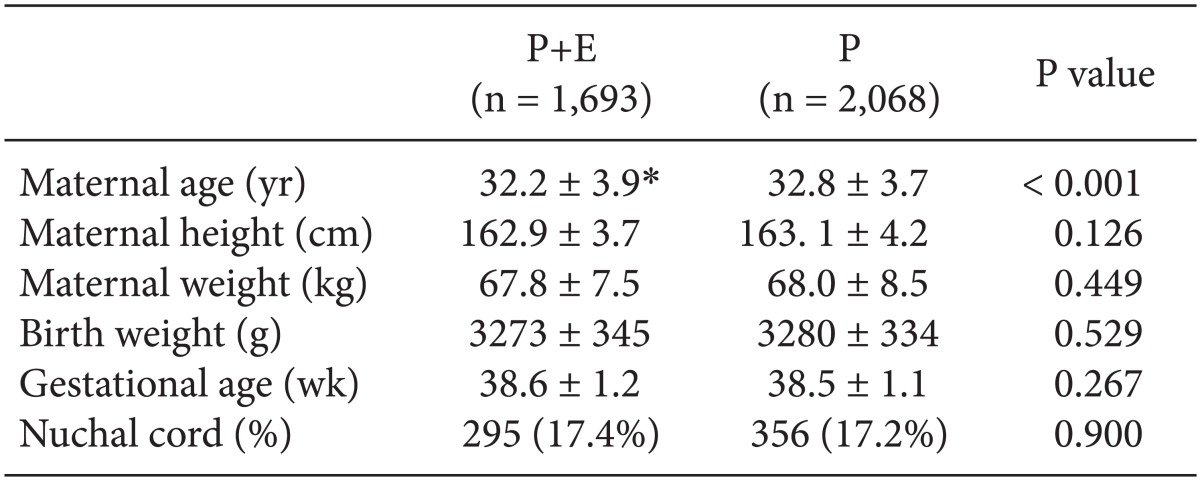
Demographic and Labor Characteristics according to Vasopressor Use
The median value of the 1 min Apgar score and the 5 min Apgar score as well as the incidence of neonates with 5 min Apgar scores < 7 were similar between the two groups (Table 2). Group P+E had a significantly increased incidence of neonates with 1 min Apgar < 7 compared with Group P (relative risk = 0.39, 95% confidence interval 0.21 to 0.70, P = 0.002). The incidence of neonates with neonatal seizure, application of continuous positive airway pressure or intermittent positive pressure ventilation, intraventricular hemorrhage, periventricular leucomalacia, and hypoxic ischemic encephalopathy was similar between the two groups.
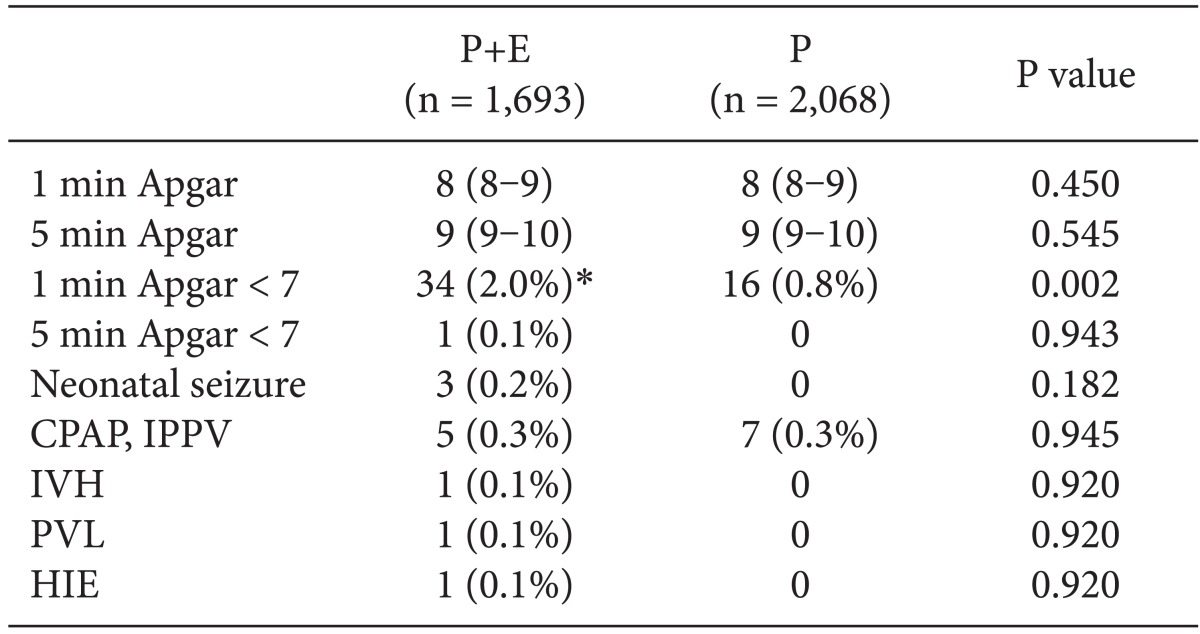
Apgar Scores and Neonatal Outcomes according to Vasopressor Use
Discussion
We observed a significant decrease in the incidence of 1 min Apgar < 7, but no decrease in the incidence of 5 min Apgar < 7 or adverse neonatal outcomes were seen when the prophylactic vasopressor was changed from the combination of phenylephrine and ephedrine to phenylephrine alone in spinal anesthesia for elective cesarean section in low-risk pregnancy.
Cooper and Gowni [11] evaluated the impact of changing the vasopressor from ephedrine to phenylephrine as the first-line vasopressor on umbilical artery pH and the incidence of fetal acidosis for cesarean section regardless of the type of anesthesia with a study population of 1,009 deliveries. They found a small increase in umbilical artery pH and a small decrease in the incidence of fetal acidosis. They claimed the main reason for the improvement of the acid-base balance was improved obstetric management of the highest-risk patients instead of the vasopressor change between the time periods. In contrast, we studied low-risk pregnancy in spinal anesthesia to minimize unevaluated risk factors that could influence the neonatal outcomes between the time periods. Previous studies found the umbilical artery pH of the phenylephrine and ephedrine group was lower than that of the group receiving phenylephrine alone, but proportions of neonates with an umbilical artery pH < 7.2 were not different between the two groups even though the study population was too small to obtain adequate statistical power [6,7]. Meta-analysis by Veeser et al. [12] demonstrated that ephedrine use increased the risk of fetal acidosis (defined by an umbilical artery pH < 7.2) and lowered BE values. However, to my knowledge, there has been no meta-analysis comparing the incidence of fetal acidosis in the phenylephrine and ephedrine group with that in the phenylephrine group.
A systematic review that analyzed 481,753 infants demonstrated that a low pH of the umbilical artery had a strong association with neonatal mortality and morbidity (hypoxic ischemic encephalopathy, seizures, intraventricular hemorrhage, periventricular leucomalacia, and cerebral palsy) [13]. In our study, there were no significant neonatal adverse outcomes between the two groups. This finding may be associated with the lack of an increase of neonates with low umbilical artery pH in the combination phenylephrine-ephedrine group compared to the phenylephrine group [6,7]. However, the proportion of neonates with adverse outcomes in our study was small (0.1-0.3%). Therefore, no definite conclusion about the impact of vasopressor change on neonatal outcomes could be drawn.
Another method of newborn evaluation is the Apgar score. Though 60 years have passed since the Apgar scoring system was developed by Virginia Apgar, the Apgar score remains an important method for the early detection of infants at risk for serious and fatal conditions [14,15]. There were no differences in Apgar scores and the risk of low Apgar scores between the phenylephrine and ephedrine groups and among the phenylephrine, ephedrine and combination of phenylephrine and ephedrine groups [3,4,6,7,16,17,18,19,20]. However, the sample sizes of these studies may be too small to detect differences in Apgar scores.
The correlation of umbilical artery pH and Apgar score is unclear. An Apgar scores less than 7 at 5 min neonatal intensive care unit admission and assisted neonatal ventilation had significant inverse relationships with both umbilical artery pH and BE (P < 0.0001) in a study of term singleton births with no major abnormalities [21]. However, only a small portion of neonates with low 5 min Apgar scores had metabolic acidosis evidenced by cord pH [22].
Known risk factors for low Apgar scores include preterm birth, postterm birth, low birth weight, small for gestational age, congenital malformation, and maternal smoking during pregnancy [23,24,25]. We excluded most risk factors in our study.
Median values of 1 min Apgar scores in both groups were similar, but the incidence of 1 min Apgar scores less than 7 was higher in the combination phenylephrine and ephedrine group than it was in the phenylephrine group in our study. We evaluated low-risk parturients, but depression of fetal pH caused by ephedrine combined with phenylephrine could increase the incidence of low 1 min Apgar scores when parturients have unanticipated risks, like a nuchal cord. However, the effect of low umbilical artery pH on Apgar scores presumably caused by ephedrine seemed to be temporary in our study. Median values of 5 min Apgar scores and the incidence of low 5 min Apgar scores were similar in both groups. Richardson et al. [26] reported a small drop in umbilical artery pH, and BE was generally well tolerated, with no difference in incidence of 5 min Apgar scores < 7.
We used 10 mg of heavy bupivacaine for spinal anesthesia. Low-dose bupivacaine between 5-7 mg may provide adequate analgesia for cesarean delivery and reduce consumption of vasopressors [27]. In addition, we used vasopressors prophylactically. A relatively large dose of bupivacaine and the prophylactic use of a vasopressor could increase the total infused dose of the vasopressor. If we performed low-dose spinal anesthesia, the ephedrine consumption would be reduced, and a proportion of low Apgar scores may be reduced as well. However, low-dose spinal anesthesia could increase the risk of intraoperative pain and an incomplete motor block [27,28].
Even though the ephedrine in the combination phenylephrine and ephedrine group could depress umbilical artery pH, it did not appear to reduce the median value of 5 min Apgar scores in our study. The five-minute Apgar score was a better predictor of neonatal outcome than umbilical artery pH, even for newborn infants with severe acidemia [29]. In accordance with this finding, neonatal outcomes of the two groups were not significantly different in our study. However, the Apgar score may be inappropriate for predicting long-term neurologic outcomes of these neonates [25].
Our study had several limitations. First, the mean age of the phenylephrine group was older than that of the combination phenylephrine and ephedrine group. This trend reflects the rapid aging of parturient patients in Korean society. However, the age difference between the groups was only 0.6 years, and previous studies reported the age range that was a risk factor for a low Apgar score is < 19 years or > 44 years, and we excluded such a range of age in our study population [24,30]. Second, our study had a small number of infants with low 5 min Apgar scores and adverse neonatal outcomes. During the periods of four years, only 8 with 5 min Apgar scores < 7 and 18 with adverse neonatal outcomes were observed when evaluating the 3,761 infants born in our hospital.
In conclusion, conversion from the combination of phenylephrine and ephedrine to phenylephrine alone as a prophylactic anti-hypotensive drug during spinal anesthesia for cesarean section in low-risk pregnancy was associated with a significant decrease in the incidence of 1 min Apgar < 7, but no decreases in the incidence of 5 min Apgar < 7 or neonatal outcomes were found. These results could indicate that when used in cesarean section, ephedrine can cause transient low Apgar scores of neonates in low-risk pregnancies. This is the first study to report such an association. Further prospective research evaluating both the umbilical artery acid-base balance and neonatal outcomes according to the use of different vasopressors will be necessary to confirm this finding.