The effects of incremental continuous positive airway pressure on arterial oxygenation and pulmonary shunt during one-lung ventilation
Article information
Abstract
Background
Although one lung ventilation (OLV) is frequently used for facilitating thoracic surgical procedures, arterial hypoxemia can occur while using one lung anesthesia. Continuous positive airway pressure (CPAP) in 5 or 10 cmH2O to the non-ventilating lung is commonly recommended to prevent hypoxemia. We evaluated the effects of incremental CPAP to the non-ventilating lung on arterial oxygenation and pulmonary shunt without obstruction of the surgical field during OLV.
Methods
Twenty patients that were scheduled for one lung anesthesia were included in this study. Systemic and pulmonary hemodynamic data and blood gas analysis was recorded every fifteen minutes according to the patient's positions and CPAP levels. CPAP was applied from 0 cmH2O by 3 cmH2O increments until a surgeon notifies that the surgical field was obstructed by the expanded lung. Following that, pulmonary shunt fraction (QS/QT) was calculated.
Results
There were no significant differences of QS/QT between supine and lateral positions with two lung ventilation (TLV). OLV significantly decreased arterial oxygen partial pressure (PaO2) and increased QS/QT compared to TLV. PaO2 and QS/QT significantly improved at 6 and 9 cmH2O of CPAP compared to 0 cmH2O. However, there were no significant differences of PaO2 and QS/QT between 6 and 9 cmH2O CPAP. In 18 patients (90%), surgical fields were obstructed at 9 cmH2O CPAP.
Conclusions
This study suggests that 6 cmH2O CPAP effectively improved arterial oxygenation without interference of the surgical field during OLV when CPAP was applied from 0 cmH2O in 3 cmH2O increments.
Introduction
One lung ventilation (OLV) during thoracic surgery leads to a good surgical field by making the lung collapse, which makes it easy to perform the operation. OLV is used to protect normal lungs from inflammatory tissue, abscess, or hemorrhage by separating normal lungs from the affected lung [1]. As minimal invasive surgeries such as video-assisted thoracic surgery have increased, the requirement for OLV has also been increasing.
Despite its advantages, OLV has major complications such as ventilation-perfusion mismatch and intrapulmonary shunt that can cause hypoxemia [2]. A number of methods to prevent hypoxemia have been introduced. These include applying continuous positive airway pressure (CPAP) to the non-ventilated lung, and positive end-expiratory pressure (PEEP) to the ventilated lung or both. However, CPAP inflates the collapsed lung and this can interfere with surgery. Although many previous studies [3-5] demonstrated the effects of CPAP on arterial oxygenation, the effects of CPAP on the surgical field were not evaluated.
In this study, we investigated the effects of incremental CPAP to the non-ventilating lung on arterial oxygenation and pulmonary shunt, as well as determining the level at which CPAP can interfere with the surgical field.
Materials and Methods
Twenty patients (American Society of Anesthesiologists 1 to 3) scheduled to have elective thoracic surgery requiring OLV under general anesthesia, were included this study. Exclusion criteria included lung resection history, obstructive and restrictive lung diseases, and severe cardiovascular disease. The study was conducted after approval from the institutional ethics committee as well as receiving informed consent from all study participants.
No pre-anesthetic medication was administrated. After arriving at the operating room, the patients were monitored by ECG, NIBP, and pulse oxymetry. After modified Allen's test, a 20 gauge arterial catheter was inserted into the radial artery to measure direct blood pressure and to sample the arterial blood for blood gas analysis. Anesthesia was induced by thiopental sodium 4-5 mg/kg, and vecuronium 0.10-0.15 mg/kg was injected to facilitate tracheal intubation. After induction of anesthesia, 37 Fr. of double lumen endotracheal tube (Bronchocath®, Mallinckrodt, Athlone, Ireland) was intubated for male patients, and 35 Fr. for female patients. Position of the tube was checked by auscultation, and confirmed by flexible fiberoptic bronchoscopy (BRO-Y3S, Fujinon, Japan). Anesthesia was maintained by fixed 1.5 minimum alveolar concentration (MAC) of sevoflurane and 1-5 ng/ml effect-site concentrations of remifentanil was co-administered using a target controlled infusion (TCI) pump (Orchestra®, Fresenius Vial, France).
During the operation, fresh gas flow rate and inspired fraction of oxygen (FiO2) were 5 L/min and 1.0, respectively. Minute ventilation was controlled by 10 ml/kg of tidal volume (TV), and the respiratory rate was adjusted to 35-38 mmHg of end-tidal CO2 pressure. Fresh gas flow rate, FiO2, and TV were maintained in the study period during OLV. Pulmonary artery catheter (Balloon thermodilution catheter, 7Fr. ARROW, USA) was inserted in to the right internal jugular vein. A portable chest X-ray was taken to confirm the accurate catheter position. Cardiac output was measured by the thermodilution method, and arterial and mixed venous bloods were sampled for gas analysis. After changing the patient's position from supine to lateral, the location of double lumen endotracheal tube was rechecked by flexible fiberoptic bronchoscopy.
Systolic, diastolic, and mean blood pressures (BP), heart rate (HR), systemic vascular resistance (SVR), central venous pressure (CVP), cardiac output (CO), arterial blood gas analysis (ABGA), and mixed venous blood gas analysis (VBGA) were recorded at: 1) supine position with TLV, 2) lateral position before opening chest wall with TLV, 3) lateral position after opening chest wall with TLV, 4) OLV without CPAP, and 5) OLV with CPAP by increment of 3 cmH2O using the CPAP device (Bronchocath® CPAP system, Mallinckrodt, USA). For an accurate measurement of CPAP, U-shaped water columns were connected to the CPAP device and the pressure difference between the two columns was measured. Hemodynamic parameters and blood gas analysis were measured 15 minutes after changing position and applying different levels of CPAP. CPAP application was ceased when a surgeon mentioned that the expanded lung interfered with the surgical field. The entire operation was conducted by a single surgeon.
Cardiac output was measured three times by the thermodilution method and averaged at every period. Intrapulmonary shunt fraction (QS/QT) was calculated by the following formula: QS/QT = ([PAO2 - PaO2] × 0.003) / (3.5 + [PAO2 - PaO2] × 0.003) [6]. This formula was used according to Shapiro's theory that under circumstance FiO2 more than 0.3, pulmonary end capillary oxygen content can be regarded as 100% [7]. Data were expressed by mean ± standard deviation. Repeat measured ANOVA was used for statistical analysis and Holm-Sidak test as post-hoc test was performed. If the P value < 0.05, the result was considered statistically significant.
Results
Patient's characteristics are shown in Table 1. Of the 20 patients, CPAP application was ceased for 18 patients at 9 cmH2O and for 2 patients at 12 cmH2O when the surgical field was interfered. Hemodynamic data is presented in Table 2. Cardiac output significantly increased when the chest wall was opened. Arterial oxygen partial pressure (PaO2) was decreased from 452 ± 38 mmHg to 251 ± 136 mmHg by OLV and significantly increased at a pressure of 6 and 9 cmH2O CPAP to 383 ± 103 and 375 ± 131, respectively. However, PaO2 was not significantly different between 6 and 9 cmH2O CPAP (Fig. 1).
Patient Characteristics in this Study

Hemodynamic Data Collected in this Study

Arterial oxygen partial pressure (PaO2) decreased by OLV and significantly increased at the pressure of 6 and 9 cmH2O CPAP. All data are expressed as mean ± S.D. Sup-TLV: supine position with two lung ventilation, Lat(CC)-TLV: lateral position with two lung ventilation before chest cavity open, Lat(OC)-TLV: lateral position with two lung ventilation after chest cavity open, OLV-0, 3, 6 ,9: one lung ventilation with CPAP 0, 3, 6, 9 cmH2O, TLV: two lung ventilation after stop CPAP. *Significantly different (P < 0.05) from supine position with two lung ventilation (Sup-TLV). †Significantly different (P < 0.05) from one lung ventilation without CPAP (OLV-0).
After the chest wall was opened, QS/QT increased from 15 ± 3.1 to 26 ± 6.6 by OLV. At 6 cmH2O CPAP, QS/QT was 19 ± 5.5 which was not significantly different from TLV (Fig. 2). Four patients showed less than 100 mmHg of PaO2 at the time OLV start. Of them, 3 patients in 3 cmH2O and 1 patient in 6 cmH2O CPAP showed PaO2 improvement of more than 100 mmHg.
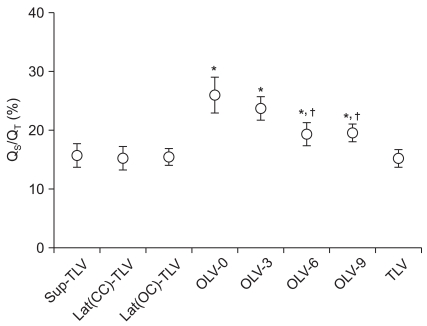
Pulmonary shunt fraction (QS/QT) increased by OLV. All data are expressed as mean ± S.D. Sup-TLV: supine position with two lung ventilation, Lat(CC)-TLV: lateral position with two lung ventilation before chest cavity open, Lat(OC)-TLV: lateral position with two lung ventilation after chest cavity open, OLV-0, 3, 6 ,9: one lung ventilation with CPAP 0, 3, 6, 9 cmH2O, TLV: two lung ventilation after stop CPAP. *Significantly different (P < 0.05) from supine position with two lung ventilation (Sup-TLV). †Significantly different (P < 0.05) from one lung ventilation without CPAP (OLV-0).
Discussion
Because PaO2 can decrease by increased intrapulmonary shunt fraction during OLV [8], an important aspect of anesthetic management during OLV is to prevent this mechanism. The anesthetic methods to increase PaO2 include using high FiO2 [8], application of positive end expiratory pressure (PEEP) to the dependent lung [9] and/or CPAP to the nondependent lung [10], intermittent TLV, and temporary ligation of the pulmonary artery [11]. Although CPAP is commonly recommended to prevent hypoxemia to the non-ventilating lung because of its simplicity and effect [12], high levels of CPAP to the operating lung can interfere with the surgical field. We attempted to evaluate the effects of incremental CPAP on PaO2 and QS/QT during OLV and determine the level of CPAP that could interfere with the surgical field. We found that 6 cmH2O CPAP effectively improved arterial oxygenation without the interference of the surgical field during OLV.
In previous studies [3-5,13], CPAP application to the non-ventilating lung increased PaO2 and decreased QS/QT. However, these studies did not consider ensuring the surgical field, which is the main purpose of OLV. In our results, 6 cmH2O CPAP compared with 9 cmH2O did not interfere with the surgical field in most patients without any significant differences between PaO2 and QS/QT. A total of 3 cmH2O CPAP did not show any effects on PaO2 and QS/QT, although the surgical field was not interfered with by the expanded lung in all patients tested.
Theoretically, a high pressure of CPAP on the non-ventilated lung moves more blood flow to the ventilated lung so that it seems to increase PaO2 to a greater exchange by pulmonary gas exchange. Alfery et al. [13] reported blood flow to the non-ventilated lung considerably decreased after adding 15 cmH2O of CPAP, but PaO2 and shunt decreasing rate was similar to that of 10 cmH2O. However, an expanded lung by high pressure of CPAP can interfere with the surgical field. This goes against the main purpose of OLV. Although we did not apply CPAP to 10 cmH2O, 6 cmH2O CPAP was significantly effective in preventing hypoxemia and securing the surgical field compared with 9 cmH2O CPAP.
We found that 4 patients (20%) showed less than 100 mmHg of PaO2 although mean PaO2 was 251 ± 136 mmHg during OLV. A total of 3 and 1 patient with 3 and 6 cmH2O of CPAP improved PaO2 more than 100 mmHg, respectively. In 18 patients (90%), 9 cmH2O CPAP interfered with the surgical field. Therefore, our study recommends using gradual increments of CPAP from low pressure at the beginning of CPAP application to improve oxygenation and secure the surgical field rather than fixed high pressure CPAP.
There were some limitations in this study. First, the lung was ventilated with FiO2 1.0 and CPAP increased by 3 cmH2O. If the lung was ventilated with less than FiO2 1.0 or CPAP increased by 1 or 2 cmH2O, the best pressure of CPAP could be different with what we found. Second, because there were no patients with significant hypoxemia during OLV in this study, there were some limitations in applying CPAP with our results to the patients with severe hypoxemia. Third, interference with the surgical field was a single thoracic surgeon's subjective decision. The decision could be affected by several factors, including the techniques used by the surgeon as well as the range and site of the lung resection. In conclusion, 6 cmH2O CPAP effectively improved arterial oxygenation without interference of the surgical field during OLV when CPAP was applied from 0 cmH2O in 3 cmH2O increments.