The effect of remifentanil versus N2O on postoperative pain and emergence agitation after pediatric tonsillectomy/adenoidectomy
Article information
Abstract
Background
Remifentanil can be an alternative to N2O in general anesthesia. Intraoperative remifentanil may lead to acute opioid tolerance. This study aims to assess the effect of remifentanil substituted for 70% N2O on postoperative pain in children undergoing tonsillectomy/adenoidectomy. In addition, we evaluated the effect of remifentanil infusion on incidence of emergence agitation in these patients.
Methods
Eighty children, aged 2-12 years, undergoing tonsillectomy/adenoidectomy were randomly allocated to the N2O group (Group N; n = 40, sevoflurane and 70% N2O) or remifentanil group (Group R; n = 40, sevoflurane with remifentanil infusion at the rate of 0.17 µg/kg/min). In the recovery room, severity of pain and agitation were assessed by an investigator blinded to the assigned group. Time to eye opening and incidence of severe pain and agitation were compared between groups. Logistic regression was used to identify factors related to occurrence of severe pain and agitation.
Results
Number of patients with severe postoperative pain was 6 and 16 in groups N and R, respectively (P = 0.012). Incidence of emergence agitation was not significantly different between groups. Remifentanil infusion was a significant factor related to the occurrence of severe postoperative pain (P = 0.015), and age was inversely related to occurrence of emergence agitation (P = 0.001).
Conclusions
In children undergoing tonsillectomy/adenoidectomy, intraoperative remifentanil infusion may increase incidence of severe postoperative pain compared to N2O, but it may not affect incidence of emergence agitation.
Introduction
Nitrous oxide (N2O) has been used as an anesthetic adjuvant during general anesthesia for centuries because of its minimum alveolar concentration-reducing effect, rapid offset and low cost. However, there are unwanted side effects such as bowel distension, postoperative nausea and vomiting [1]. Although rare, N2O has also been associated with serious complications such as myelopathy, megaloblastic anemia and vitamin B12 deficiency [2], as it inactivates vitamin B12, a key enzyme for methionine synthase. In addition, N2O may be harmful to the developing brain in animal study [3]. Therefore, other alternatives to N2O may be needed.
Remifentanil is a widely used opioid. Because of its rapid onset and offset, remifentanil can be an ideal substitute for N2O. It can be given in high doses intraoperatively without causing postoperative respiratory depression. However, it has some drawbacks such as muscle rigidity, postoperative nausea and vomiting and dose-dependent decreases in systolic blood pressure and heart rate [4]. There is some evidence that remifentanil increases postoperative analgesic requirement due to acute opioid tolerance [5,6]; however, inconsistent findings have been also presented [7,8]. Further studies on the effect of remifentanil on postoperative pain are needed.
Emergence agitation is a common phenomenon in pediatric patients anesthetized with sevoflurane, which has been the subject of numerous investigations [9]. The use of analgesics may affect the incidence of emergence agitation [10]. However, there is little evidence that intraoperative remifentanil may affect its incidence.
In this study we aimed to compare postoperative pain of sevoflurane-remifentanil anesthesia with that of sevoflurane-N2O anesthesia in children undergoing tonsillectomy/adenoidectomy. Based on the previous study by Lee et al. [7], remifentanil was infused at the rate of 0.17 µg/kg/min as a substitute for 70% N2O. We also compared the incidence of emergence agitation between groups.
Materials and Methods
After obtaining approval of the Institutional Review Board and informed consent from parents, 80 pediatric patients aged 2-12 years (American Society of Anesthegiologists class I, II) and undergoing elective tonsillectomy/adenoidectomy were enrolled. Patients were excluded from the study if they had allergy to opioids, hepatic or renal dysfunction, neurological disease, psychological disease or airway problems.
The sample size required for a 15% difference in incidence of severe pain with different anesthetics was 28 patients for each group (for a level of significance of 0.05 and a power of 0.80). It was calculated based on the assumption that incidence of severe pain in sevoflurane-N2O group would be approximately 20%. For a 15% difference in incidence of severe agitation, the sample size was calculated to be 37 for each group based on the assumption that incidence of severe agitation in the sevoflurane-N2O group would be 30% (for a level of significance of 0.05 and a power of 0.80) [11]. It was decided to include 40 patients in each group.
Patients were randomly allocated to the N2O (group N, n = 40) or remifentanil group (group R, n = 40). A computer generated random numbers table was used for randomization of group assignment.
Glycopyrrolate 0.005 mg/kg was injected intramuscularly as a premedication 30 minutes before anesthesia. When the patient arrived at the operating room, preoperative behavior was evaluated and categorized into one of the following: calm, slightly anxious, uncooperative. This was performed by an anesthesiologist who carried out the anesthesia of all patients in the study. Electrocardiography, non-invasive blood pressure and pulse oximetry were monitored.
In both groups, general anesthesia was induced with thiopental 5 mg/kg, rocuronium 0.6 mg/kg and 3-4 vol% sevoflurane in oxygen 5 L/min (FIO2 1.0). After intubation, group N received sevoflurane and 70% N2O for maintenance of anesthesia (FIO2 0.3). Group R received sevoflurane with remifentanil infusion at the rate of 0.17 µg/kg/min (FIO2 0.3: O2 0.6 L/min, medical air 4.4 L/min) for maintenance of anesthesia. In both groups, sevoflurane was titrated to maintain systolic blood pressure within 20% of pre-anesthetic values.
End-tidal concentrations of sevoflurane and carbon dioxide were continuously monitored (anesthetic Gas Module No. M1026B, Phillips Medical System, Best, Netherlands). End-tidal sevoflurane concentrations were recorded at 5-minute intervals. From these values, the area under the sevoflurane concentration curve was approximated by the trapezoidal rule. Then, it was divided by the total anesthetic time in minutes. This value was regarded as the mean end-tidal sevoflurane concentration (Et-Sevo).
During surgery, the surgeon infiltrated 1% lidocaine with epinephrine (1 : 100,000) at the operation site for bleeding and pain control. At the end of surgery, all anesthetics were stopped and neuromuscular blockade was reversed with pyridostigmine 0.25 mg/kg and glycopyrrolate 0.005 mg/kg. The endotracheal tube was extubated when patients opened their eyes with full recovery of spontaneous breathing and adequate motor activity. The time to eye opening from stopping anesthetics was measured. After extubation, children were transferred to the postanesthetic care unit (PACU).
In the PACU, vital signs, modified Aldrete recovery score, pain score and agitation score were checked at 5-minute interval for 60 minutes by an anesthesiologist who was blinded to the assigned group and not involved in the anesthetic procedure. To assess postoperative pain, the Oucher scale was used, which is a validated and useful measure for pre-school as well as for primary school-aged child [12]. The Oucher scale consists of six gradations from 0 to 100 (0, 20, 40, 60, 80, 100). Pain was assessed via facial expression. A score of 0 was assigned to a child who was calm and complaisant, and 100 to a child in a state of severe distress, accompanied by constant crying and a grimacing expression [12]. Severe pain was defined as an Oucher pain score above 60. To avoid misinterpretation of pain level due to influence of agitation, pain scores in the first 5 minutes of the PACU stay were omitted from the count of severe pain. In case of severe pain or patient's complaint of pain, 0.5 µg/kg of intravenous fentanyl was administered. If additional pain control was required, 0.25 µg/kg of fentanyl was administered as necessary.
Emergence agitation was assessed using a 4-point scale [13] (1, calm; 2, not calm but could be easily calmed; 3, not easily calmed, moderately agitated; 4, combative, excited or disoriented). Severe agitation was defined as an agitation score 3 or 4.
To check nausea and vomiting episodes, a 4-grade scale was used: grade 0 = absence of nausea and vomiting; grade 1 = nausea only; grade 2 = single emetic episode; grade 3 = multiple emetic episodes. If necessary, intravenous ondansetron 50 µg/kg was given to treat nausea and/or vomiting.
Statistical analysis was performed using SPSS version 13.0 for Windows (SPSS Inc, USA). Data were compared between two groups by t-test, Mann-Whitney U test or Chi-square test, as appropriate. Logistic regression was used to identify significant variables involving occurrence of severe pain and agitation. Covariates in logistic regression were age, sex, weight, duration of operation, Et-Sevo, and group (remifentanil infusion or not). P < 0.05 was considered statistically significant.
Results
Of the 80 patients enrolled in the study, two children were excluded because of reoperation. Thus, data from 78 patients were analyzed. No significant differences were found between groups in terms of age, sex and height. Weight was higher in group N than in group R (Table 1). Preoperatively, most patients were calm. Two children were anxious, but they were also cooperative. There were no differences between groups in operation time, time to eye opening and time to reach discharge criteria (modified Aldrete recovery score of 10). The Et-Sevo was higher in group N than in group R (P < 0.05) (Table 2).
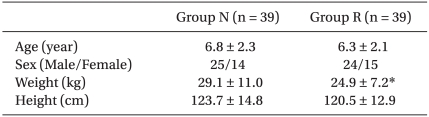
Demographic Data

Mean Sevoflurane Concentration, Surgical and Recovery Durations
Immediately after arriving at the PACU, pain and agitation scores were not different between groups. More patients showed severe postoperative pain in group R than in group N (number of patients with severe postoperative pain: 6 and 16 in group N and R, respectively; P = 0.012). In addition, the number of patients receiving fentanyl in the PACU was higher in group R than in group N (10 and 20 in group N and R, respectively. P = 0.020). However, there were no significant differences between groups in the count of fentanyl administration (0.38 ± 0.91 and 0.59 ± 0.64 [mean ± SD] in groups N and R, respectively). Fentanyl dose given in the PACU did not differ significantly between groups (Table 3). In cases of severe pain, there was no difference in time to onset between groups (mean ± SD: 23.3 ± 13.3 and 18.4 ± 6.3 minutes in groups N and R, respectively). Incidence of severe agitation was not different between groups (Table 3).
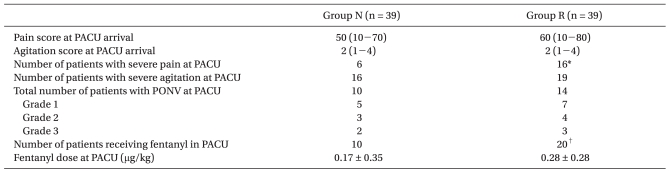
Postoperative Profiles
For logistic regression, age, sex, weight, duration of operation, Et-Sevo and group (remifentanil infusion or not) were included as covariates. In univariate and multivariate logistic regression, group was the only covariate associated with severe pain (P = 0.015). Severe agitation was significantly related with age (P = 0.001), weight (P = 0.003), and Et-Sevo (P = 0.049) in univariate analysis. However, in multivariate analysis, only age remained significant.
The following equations were obtained from logistic regression with forward stepwise (Wald) for severe pain and agitation.

Z = -3.047 + 1.342 × remifentanil infusion (P = 0.015)
Odds ratio (95% Confidence interval) for remifentanil infusion group: 3.826 (1.301 - 11.253).

Z = 3.161 - 0.537 × age (P = 0.001)
Odds ratio (95% Confidence interval) for increasing age: 0.585 (0.429 - 0.797).
Remifentanil infusion was a significant factor related to occurrence of severe postoperative pain (P = 0.015), and age was inversely correlated with occurrence of emergence agitation (P = 0.001).
Number of patients who experienced postoperative nausea and vomiting was 10 and 14 in groups N and R, respectively (Table 3). In each group, 5 patients were treated with ondansetron 50 µg/kg. No major complications were observed in any patient during the study period.
Discussion
In the current study, 0.17 µg/kg/min of remifentanil infusion led to higher incidence of severe postoperative pain compared to 70% N2O. This finding was also supported by results of logistic regression analysis.
Increased postoperative pain in the remifentanil group may have been related with acute opioid tolerance.
Intraoperative remifentanil infusion can lead to acute opioid tolerance [5,6]. Though the underlying mechanism remains unknown, activation of N-methyl-D-aspartate (NMDA) receptor function has been suggested to play important roles [14,15]. Opioid tolerance is known to develop very rapidly. In experimental pain models with volunteers receiving constant rate infusion of remifentanil, hyperalgesia or opioid tolerance was observed after a 30- to 90-min infusion [16,17].
The dose of remifentanil is a factor affecting development of opioid tolerance. In adult patients, postoperative pain score and morphine consumption were higher in patients receiving a high dose of intraoperative remifentanil (0.3 µg/kg/min) compared to those receiving a low dose (0.1 µg/kg/min) [6]. In another study, it was demonstrated that hyperalgesia to painful pressure stimuli developed after high dose remifentanil (0.4 µg/kg/min) rather than low dose (0.1 µg/kg/min) [18].
In a study by Lee et al. [7], intraoperative remifentanil infusion at the rate of 0.17 µg/kg/min did not induce acute opioid tolerance. However, the same dose of remifentanil altered postoperative pain in the present study. The inconsistent results could be caused by differences in study populations, surgical procedures and postoperative pain management between the two studies. In addition, the actual infusion schemes were not the same. While remifentanil was infused at a fixed rate in our study, variable infusion rates were used in the other study and mean infusion rate was calculated later.
Incidence of severe pain and number of patients receiving fentanyl in the PACU were higher in the remifentanil group. However, fentanyl doses in the PACU were not significantly different between groups in the current study. This discrepancy seems to originate from variability in total fentanyl doses among children. Since in some patients fentanyl was given more than once (initially 50 µg/kg then additional 25 µg/kg if needed), the total fentanyl doses were variable among patients.
In some studies, intraoperative infiltration of local anesthetics to the surgical field and/or non-steroidal anti-inflammatory drugs provided adequate postoperative analgesia [19,20]. In the present study with intraoperative injection of local anesthetics, 56 children (71.8%) did not complain of severe pain in the PACU.
Emergence agitation is a common phenomenon in pediatric patients after anesthesia. It is known to be affected by type of anesthetic, age, gender, previous surgery, preoperative anxiety, adaptability, type of surgery (especially ophthalmology and otorhinolaryngology procedures), analgesics, and time to awakening [21,22]. Incidence of emergence agitation in pediatric patients after sevoflurane anesthesia has been reported to be about 33-80% [23,24]. In children aged 3-9 years undergoing strabismus surgery, incidence of emergence agitation assessed by a 4-point scale was 35% in the sevoflurane group [23]. In a study by Cravero et al. [24], emergence agitation was measured based on two different criteria in children scheduled for magnetic resonance imaging. In the study, when high threshold criteria (level 5, thrashing behavior requiring restraint) were applied, the incidence after sevoflurane anesthesia was 33%. However, with lower threshold (level 4, crying) criteria, incidence was 80% in the same group of children.
In the present study, incidence of severe emergence agitation was 44.9% in total. No difference was found between groups (41.0% and 48.7% in groups N and R, respectively). Rapid awakening after use of insoluble anesthetics may initiate emergence agitation by worsening underlying apprehension in children [25]. Even though remifentanil has the same characteristics (rapid awakening), there is no evidence that remifentanil can cause emergence agitation. From the logistic regression of this study, remifentanil infusion was not associated with increased incidence of severe agitation. However, age was inversely related to probability of emergence agitation, which is consistent with a previous study [26].
In this study, we considered remifentanil infusion at the rate of 0.17 µg/kg/min to be equipotent to 70% N2O based on the previous findings of Lee et al. [7], which were obtained from adult patients undergoing colorectal surgery. However, in the present study, patients in group R consumed less sevoflurane than those in group N by 11% (Table 2), which suggests the equipotent dose of remifentanil to 70% N2O may be slightly less than 0.17 µg/kg/min. Mathews et al. [27] reported that 66% N2O may be replaced by a remifentanil bolus 0.7 µg/kg followed by infusion of 0.085 µg/kg/min, which corresponds to 2 ng/ml of remifentanil blood concentration in adult patients for ambulatory orthopedic surgery. Dissimilarities among studies in the way of assessing anesthetic depth and type of surgery seem to be the main causes of inconsistent findings. It has been reported that clearance of remifentanil is higher in children compared to adults [28]. Therefore, pharmacokinetic differences between adults and children might be another factor causing the inconsistencies between this study and others.
Even though Et-Sevo was slightly higher in group N, no difference was observed between groups in recovery indices such as time to eye opening and time to reach discharge criteria. The 50% washout time of sevoflurane is less than 5 minutes [29]. Therefore, it is less likely that the difference in Et-Sevo affects altered incidence of severe postoperative pain between groups.
There were some limitations in the present study. Since lidocaine infiltration was done by a surgeon, the amount of lidocaine was not controlled. This might affect the severity of postoperative pain because lidocaine infiltration was the only measure for postoperative analgesia. Using established protocol of local infiltration or intraoperative analgesics might eliminate this potential problem. Another limitation was the lack of objective measure such as bispectral index in assessing depth of anesthesia. Even though we assessed the analgesic component of anesthesia based on vital signs, additional usage of bispectral index could be helpful for titrating sevoflurane concentrations and for confirming the equipotent dose of remifentanil to 70% N2O.
In conclusion, in children undergoing tonsillectomy/adenoidectomy, intraoperative remifentanil infusion may increase incidence of severe postoperative pain compared to 70% N2O. However, incidence of severe emergence agitation did not change when substituting intraoperative remifentanil infusion for N2O.
Acknowledgements
This work was supported by the 2006 Inje University research grant.