Effect of chemotherapy on effect-site concentration of propofol for loss of consciousness in patients with colorectal cancer
Article information

Abstract
Background
The depth of anesthesia is an essential factor in surgical prognosis. The neurotoxic effect of chemotherapeutic drugs affects the sensitivity to anesthetics. This study was conducted to determine whether the effect-site concentration (Ce) of propofol for loss of consciousness (LOC) differs in patients undergoing preoperative chemotherapy.
Methods
A total of 60 patients scheduled for surgery for colorectal cancer under general anesthesia were included in this study. Patients who had received chemotherapy comprised the experimental (C) group, and those without a previous history of chemotherapy comprised the control (N) group. Propofol was administered as an effect-site target-controlled infusion, and the Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scores were evaluated. When the plasma concentration and Ce were similar, and if the MOAA/S score did not change, the target Ce was increased by 0.2 μg/ml; otherwise, the Ce was maintained for 2 min and then increased.
Results
The Ce values of propofol for loss of verbal contact (LVC) in groups C and N were 2.40 ± 0.39 and 2.29 ± 0.39 μg/ml (P = 0.286), respectively, and those for LOC in groups C and N were 2.69 ± 0.43 and 2.50 ± 0.36 μg/ml (P = 0.069), respectively. No significant difference was observed in Ce values between the two groups.
Conclusions
Chemotherapy had no effect on the Ce of propofol for LVC and LOC in patients with colorectal cancer. We do not recommend reducing the dose of propofol for the induction of LOC in patients with colorectal cancer undergoing chemotherapy.
Introduction
Colorectal cancer is the third most diagnosed malignancy and the second leading cause of cancer-related death in the world [1]. Advances in chemotherapy, surgery, and radiotherapy have improved the outcomes for patients with colorectal cancer [2]. Nevertheless, the toxicity of chemotherapeutic drugs to healthy tissues can cause a variety of side effects in various systems in the body, including the nervous, hepatorenal, and pulmonary systems [3]. The systemic toxicity of chemotherapy has important implications for general anesthesia. Studies have reported that chemotherapy induces neurotoxic effects on both the central and peripheral nervous systems, including peripheral and autonomic neuropathy [3–5]. Moreover, there are studies related to changes in sensitivity to anesthetics due to the neurotoxicity of chemotherapeutic drugs [4]. Du et al. [6] reported that the minimum alveolar concentration (MAC) required for 50% blockade of the adrenergic response (BAR) [MAC-BAR] value of sevoflurane in patients with gastric cancer was 2.2% for the chemotherapy group and 3.0% for the control group (P < 0.05). They concluded that chemotherapy reduced the MAC-BAR value of sevoflurane by enhancing the inhibitory effect of sevoflurane on the stress response. Wu et al. [7] also reported that neoadjuvant chemotherapy can enhance the sensitivity of patients with breast cancer to the anesthetic effect of propofol. The drug 5-fluorouracil (5-FU) is the most used chemotherapeutic agent for colorectal cancer, and additionally, leucovorin (LV), irinotecan, oxaliplatin, cetuximab, and capecitabine are frequently used [8,9]. 5-FU has been described as being potentially neurotoxic in patients; however, these side effects are quite rare in clinical practice [10]. Oxaliplatin, a platinum derivative currently used in combination with 5-FU to treat colorectal cancer, induces an acute neurotoxicity manifested as distal dysesthesias as well as chronic sensory peripheral neuropathy [11]. The incidence of chemotherapy-related neurotoxicity in patients with colorectal cancer has been extensively investigated. For instance, Peng et al. [12], reported a neurotoxicity incidence of 69.7% in the case of the XELOX regimen (oxaliplatin + capecitabine), and Petrioli et al. [13] reported that the incidence of neurotoxicity was 84.3% in the case of the FOLFOX-6 regimen (5-FU + oxaliplatin + LV).
Propofol, which is currently the most widely used drug for the induction of anesthesia may cause side effects such as hypotension and apnea when administered in excess [14,15]; hence, it is preferable to administer an appropriate amount according to the desired anesthetic depth based on the exact pharmacology. Moreover, as drugs with nonblood action sites such as propofol exhibit a time delay phenomenon between blood concentration and drug effect, it is important to estimate the effect-site concentration (Ce) that can represent the effect of the drug based on an accurate pharmacodynamic (PD) model.
The primary purpose of this study was to determine whether the Ce of propofol for loss of consciousness (LOC) differs in patients who had previously undergone chemotherapy. The secondary purpose was to estimate the PD parameters, the Ce of propofol with a 50% probability of a given sedation level (Ce50), and the Hill coefficient (γ) by PD modeling.
Materials and Methods
Study design
This observational cohort study was reviewed and approved by the Institutional Review Board (IRB No. 2019-01-015) and a Clinical Research Information Service (CRIS No. KCT0003769). The study was conducted in accordance with the Helsinki Declaration-2013. We explained the study method and obtained a written informed consent from the hospitalized patients on the day before surgery. We recruited patients scheduled to undergo surgery for colorectal cancer or colostomy reconstruction under general anesthesia, considering the following inclusion criteria: age 18–75 years, body mass index (BMI) 18–29.9 kg/m2, and American Society of Anesthesiologists physical status 1–2. The exclusion criteria were as follows: a history of neurological or neuropsychiatric treatment, medication of sedatives, chronic alcoholics, difficulty in communicating, difficulty in maintaining airway during induction of anesthesia, and a history of chemotherapy of ≥ 13 months before surgery (Fig. 1). As a result of the pilot study, the mean Ce values of propofol for LOC were 2.57 μg/ml in the experimental (C) group and 2.93 μg/ml in the control (N) group, with a common standard deviation (SD) of 0.35. To calculate the number of samples, set G*Power (version 3.1.9.2, Franz Faul, University Kiel, Germany) to ‘t-test, mean: difference between two independent means (two groups), tails: two, effect size: 1.02, power: 0.95, alpha: 0.05, allocation ratio: 1:1' Based on the calculation of the number of samples, there were 26 patients in each group, and 30 patients in each group were enrolled in consideration of dropout during the study. The study methods for groups C and N were similar. Upon entering the operating room, vital signs (blood pressure, electrocardiography, heart rate, and pulse oximetry) and Bispectral IndexTM (BIS; Covidien, USA) were monitored. For airway management, 100% oxygen was supplied at 6 L/min using a facial mask with end-tidal CO2 (capnography) monitoring. For the induction of anesthesia, propofol was administered as an effect-site target-controlled infusion (Effect-site TCI, Orchestra® Base Primea, Fresenius Kabi Company, France) using the Schnider model [16], and the initial target of Ce was 1.0 μg/ml. The Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scores (Table 1) were evaluated every 30 s [17], and the BIS value at that time point was recorded. When the plasma concentration (Cp) and Ce became similar, and if the MOAA/S score did not change, the target of Ce was increased by 0.2 μg/ml, or if the MOAA/S score decreased, the target Ce was not increased immediately but was maintained for 2 min and then increased. This process was repeated until the MOAA/S score became zero.

Description about the participants. The experimental (C) group, who have received chemotherapy for colorectal cancer within 12 months of the date of surgery, the control (N) group, who have never received chemotherapy; 30 patients were recruited in each group.

Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) Scores
Statistical analysis
An MOAA/S score of 2 or 3 is defined as ‘loss of verbal contact (LVC),’ and an MOAA/S score of 0 or 1 is defined as ‘LOC.’ Statistical analyses were performed using the software MedCalc (version 18, MedCalc Software Bvba, Belgium) and GraphPad Prism (version 9, GraphPad Software, USA). T-test was performed to compare the mean values of two independent samples (e.g., experimental vs. control group, male vs. female), and one-way analysis of variance (ANOVA) was performed to test the difference between the mean values of several subgroups of a variable (multiple testing). Data were expressed as mean ± SD or median ± 95% CI. P values of < 0.05 were considered to be statistically significant.
PD modeling
We performed PD modeling to determine the Ce of propofol for each MOAA/S score using the nonlinear mixed-effects modeling software (NONMEM® 7.5, ICON Development Solution, Ireland). The relationship between the probability of response (MOAA/S score) and the Ce of propofol was analyzed using the following sigmoid Emax model:
where P (MOAA/S ≤ n) was the probability of the sedation level that would be equal to or less than a given MOAA/S score (n), Ce50 (n) was the Ce of propofol with a 50% probability of MOAA/S score (n), and γ (Hill coefficient) was the slope steepness of the Ce versus the response (MOAA/S score) curve. We defined the likelihood (L) of the observed response (R; 0 or 1) on the MOAA/S score (n) using the following equation:
The values of interindividual variability (η) of Ce50 (4), Ce50 (3), Ce50 (2), Ce50 (1), Ce50 (0), and γ were fixed at zero; this indicated that no interindividual random variability was assumed. The model parameters were estimated using the option in NONMEM of ‘LIKEHOOD LAPLACE METHOD = conditional.’ A nonparametric bootstrap procedure was performed for internal validation of the model using Pirana Modeling Workbench 3.0 (Certara, USA), and the original data set was randomly sampled to generate 1000 bootstrap replicates. The final model parameter estimates were compared with the 2.5%–97.5% CIs of the model parameters from the bootstrap.
Results
We enrolled 60 patients in this study, of whom 2 were excluded due to a mistake in propofol dose adjustment during the study. Hence, the data of 58 patients were analyzed. Group C consisted of 23 male and 7 female, and group N consisted of 16 male and 12 female. The characteristics of the participants are summarized in Table 2. In Group C, the 30 patients who received chemotherapy were divided into four subgroups according to the type of chemotherapy drug as follows: 14 patients (11 male/3 female) treated with xelobig (capecitabine), 3 patients (3 male) treated with FOLFIRI (irinotecan + LV + 5-FU), 11 patients (8 male/3 female) treated with mFOLFOX (oxaliplatin + LV + 5-FU), and 2 patients (1 male/1 female) treated with oxaliplatin and capecitabine. The median duration of chemotherapy for patients in Group C was 44.5 (range: 16–437) days, the median duration from the last chemotherapy to surgery was 48.5 (range: 1–146) days, and among them, 12 patients had a duration of < 30 days. The changes in vital signs and BIS values are depicted in Figs. 2 and 3 shows the Ce of propofol for LVC, LOC, and each MOAA/S score of groups C and N. The comparison of Ce and BIS values at LVC and LOC between groups C and N is summarized in Table 3. No significant difference was observed in Ce and BIS values between the two groups. However, the Ce of propofol for LOC showed a significant difference depending on gender (2.67 ± 0.41 μg/ml for male, 2.45 ± 0.37 μg/ml for female, P = 0.04). Time spent on LOC was 14.28 ± 2.57 min for male and 12.41 ± 2.49 min for female (P = 0.01). BIS values at LOC were 68.00 ± 7.53 for male and 71.84 ± 7.99 for female (P = 0.08). Supplementary Table 1 shows the comparison of Ce and BIS values at LVC and LOC according to whether chemotherapy was administered in male and female. Supplementary Table 2 shows the differences in Ce and BIS values at LVC and LOC according to gender in groups C and N, respectively. Table 4 summarizes the PD parameter estimates, along with the standard error of the nonparametric bootstrap replicate of the final PD model and the median parameter with the ranges of 2.5, 97.5% for each MOAA/S score. The probability of reaching ‘MOAA/S ≤ n’ and ‘MOAA/S = n’ as a function of predicted Ce for propofol based on the final PD model is shown in Fig. 4. The predicted propofol concentrations producing a 50% probability of moderate sedation (defined as ‘MOAA/S ≤ 3’) and deep sedation (defined as ‘MOAA/S ≤ 1’) were 2.25 and 3.11 μg/ml in group C and 2.12 and 2.66 μg/ml in group N, respectively.

Characteristics of Participants

Changes in vital signs and value of BIS during study period. Gray circle and red line: experimental (C) group (those who had received chemotherapy), white circle and blue line: control (N) group (those who did not receive chemotherapy), middle bold line and error bar: median and 95% CI. MOAA/S: Modified Observer’s Alertness/Sedation scale, SBP: systolic blood pressure, DBP: diastolic blood pressure, HR: heart rate, BIS: bispectral index.
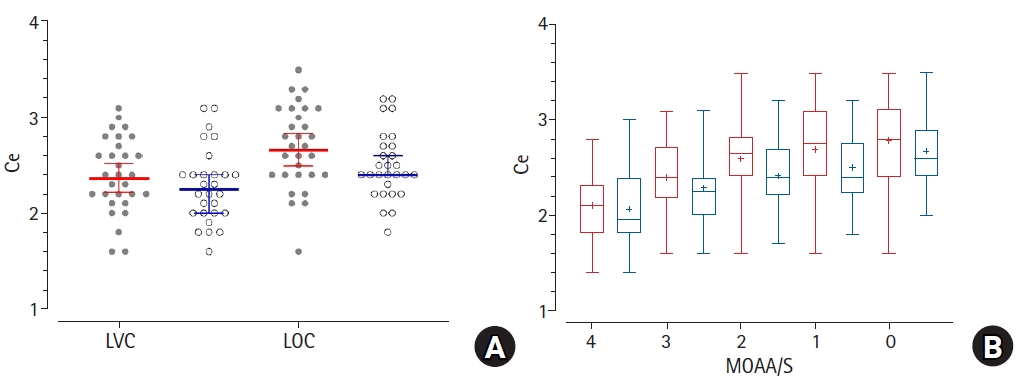
Comparison of the Ce of propofol for LVC, LOC and each MOAA/S score between the experimental (C) group and the control (N) group. (A) Ce of propofol for LVC and LOC, gray circle and red line: experimental (C) group (those who had received chemotherapy), white circle and blue line: control (N) group (those who did not receive chemotherapy), middle bold line and error bar: median and 95% CI, (B) Ce of propofol for each MOAA/S score, red: group C, blue: group N. In this box-and-whisker plot, the center line of the box represents the median value, whiskers are 2.5–97.5 percentiles, plus sign (‘+’) represents the mean value. Ce: effect-site concentration of propofol, MOAA/S: Modified Observer’s Alertness/Sedation scale, LVC: loss of verbal contact (when the MOAA/S score was 3 or 2), LOC: loss of consciousness (when the MOAA/S score was 1 or 0).

Comparison of Ce and BIS Values at LVC and LOC according to Whether Chemotherapy Was Administered
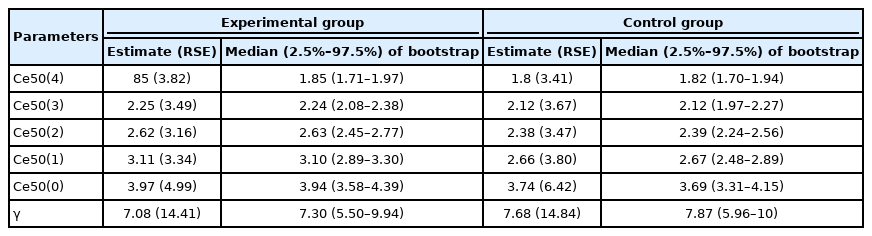
PD Modeling Results of Experimental Group and Control Group

Probability curve on reaching a given sedation level of the experimental (C) group and the control (N) group based on the final PD model. (A) Probability of reaching each MOAA/S scale being equal to or less than a given level (MOAA/S ≤ n), (B) Probability of reaching each MOAA/S scale being equal to a given level (MOAA/S = n), left: experimental (C) group (those who had received chemotherapy), right: control (N) group (those who did not receive chemotherapy). PD: pharmacodynamic, MOAA/S: Modified Observer’s Alertness/Sedation scale.
Discussion
Due to an increase in the number of patients receiving preoperative chemotherapy, the number of patients with potentially dangerous and undesirable side effects when using intravenous anesthetics may also increase. Therefore, it is valuable and important to consider the pharmacological interactions between chemotherapeutic drugs and anesthetics. Moreover, studies have demonstrated that the neurotoxicity of chemotherapeutic agents affects sensitivity to anesthetics, reduces the MAC of inhaled anesthetics, and reduces the Ce of propofol required for LOC. Several studies have already been conducted to examine the correlation between chemotherapy and anesthesia for breast cancer, hepatic cancer, and gastric cancer [6,15,18]. However, the types of chemotherapeutic agents used for treatment differ according to the type of cancer [19]. Our results showed that chemotherapy had no effect on the Ce of propofol for LOC in patients with colorectal cancer. In contrast, previous studies on patients with breast cancer reported different results from those of our study. According to the study of He et al. [18], the Ce of propofol at LOC in patients with breast cancer who received chemotherapy with taxol and CAF therapy (cyclophosphamide + adriamycine + 5-FU) was significantly lower than that in patients who did not receive chemotherapy. Wu et al. [7] also reported that patients with breast cancer who received neoadjuvant chemotherapy (docetaxel + epirubicin + cyclophosphamide) had a significantly shorter duration of propofol infusion and a lower mean propofol dosage for LOC. The differences in results between our study and other studies are believed to be due to the difference in the types of chemotherapy drugs. Our study patients had received chemotherapy with xelobig (capecitabine), FOLFIRI (irinotecan + LV + 5-FU), mFOLFOX (oxaliplatin + LV + 5-FU) or oxaliplatin + capecitabine.
We suspected that chemotherapy drugs could enhance the action of propofol by causing neurotoxicity. However, the present study failed to validate our suspicion, and we found that chemotherapy drugs did not influence the PDs of propofol in these patients. Standard chemotherapy for breast cancer is administered by injection every 3 weeks for 3–6 months. The most effective anticancer drugs for breast cancer are anthracyclines (doxorubicin) and taxanes (docetaxel), which are among the drugs with relatively several neurotoxic side effects [20]. On the other hand, standard chemotherapy for colorectal cancer is to administer the FOLFOX combination therapy by injection every 2 weeks for a total of 12 times for about 6 months [21]. In general, surgery is performed approximately 6–10 weeks after the completion of chemotherapy [21]. Differences in the therapeutic agents used for chemotherapy for breast cancer and colorectal cancer and differences in the treatment duration may be the reasons for the difference in the results of propofol sensitivity between previous studies and our study.
However, in our study, there were differences in the Ce of propofol for LOC depending on gender. The Ce of propofol for LOC was higher in male than in female (2.67 ± 0.41 μg/ml for male and 2.45 ± 0.37 μg/ml for female, P = 0.04). Kodaka et al. [22] compared the Ce of propofol at LOC in male and female and found that it was significantly higher in male than in female (2.9 ± 0.2 μg/ml for male and 2.7 ± 0.1 μg/ml for female). A difference existed in the susceptibility to propofol between male and female. As shown in Supplementary Table 1, the Ce of propofol at LOC did not differ according to whether chemotherapy was administered in male and female. Moreover, according to Supplementary Table 2, there was no statistical difference in the Ce of propofol at LOC according to gender in groups C and N. In a previous study, Adachi et al. [23] investigated the factors that affect the Cp of propofol required for sleep induction among patient characteristics. The Cp of propofol until LOC was found to be significantly affected by cardiac output, age, and weight. They found no significant difference in age, but the mean weight of male was significantly higher than that of female. In our study, the average height and weight of male were higher than those of female, but there was no difference in age and BMI.
Our study has some limitations. First, we did not directly measure the Cp of propofol in a laboratory, and it was only deduced by the TCI machine system. The two values could have certain differences. Second, the chemotherapy regimens used in our study were diverse, and the number of subjects for each chemotherapy regimen was not sufficiently large. Therefore, in further studies, it is necessary to increase the number of patients for each chemotherapy regimen and determine whether a difference exists in the Ce of propofol for LOC according to the regimen. Third, there was a difference between the sex ratios of group C (male:female = 23:7) and group N (male:female = 16:12). Such difference in the sex ratio between these two groups may have affected our study results.
In conclusion, under the conditions of this study, we found that the Ce values of propofol for LOC were 2.69 ± 0.43 and 2.50 ± 0.36 μg/ml for patients undergoing elective colorectal surgery in the presence and absence of chemotherapy, respectively. We do not recommend reducing the dose of propofol for the induction of LOC in patients with colorectal cancer undergoing chemotherapy. Moreover, we found that the Ce of propofol for LOC showed a significant difference between male and female (2.67 ± 0.41 for male and 2.45 ± 0.37 μg/ml for female, P = 0.04). We do recommend reducing the dose of propofol for the induction of LOC in female patients with colorectal cancer.
Notes
Funding
None.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Seunghee Ki (Conceptualization; Visualization; Writing – original draft)
Yongwon Cho (Data curation; Writing – original draft)
Youngkyung Choi (Methodology; Resources)
Sehun Lim (Project administration; Supervision)
Myounghun Kim (Formal analysis; Investigation)
Jeonghan Lee (Writing – review & editing)
Supplementary Materials
Comparison of Ce and BIS values at LVC and LOC according to whether chemotherapy was administered in male and female
Comparison of Ce and BIS values at LVC and LOC according to the sex of the experimental (C) group and the control (N) group