Serratus anterior plane block combined with monitored anesthesia care for surgery of lateral side of breast -a case report-
Article information

Abstract
Background
In breast surgery, regional anesthesia rather than primary anesthesia has been mainly used for postoperative analgesia. Serratus anterior plane block is a new method for ultrasound-guided thoracic wall block. It is less invasive and relatively safer than conventional regional anesthetic techniques.
Case
We report a case of breast surgery under serratus anterior plane block as primary anesthesia with monitored anesthesia for a 78-year-old patient with a medical history of cardiopulmonary resuscitation due to stress-induced cardiomyopathy caused by pneumonia.
Conclusions
Serratus anterior plane block might be simple and effective technique for breast surgery when a lesion is located on lateral side.
Breast surgery under regional anesthesia is rarely performed. However, regional anesthesia via thoracic epidural anesthesia, thoracic paravertebral block, intercostal nerve block, or pectoral nerve block has been used to treat postoperative pain after breast surgery [1]. Serratus anterior plane block is a new method of ultrasound-guided thoracic wall block with pectoral nerve (Pecs) block [2]. There are no reports about its complications. It is relatively easy and reduces complications such as hematoma, pneumothorax, or local anesthetic toxicity [1]. Here, we present a breast surgery using serratus anterior plane block as primary anesthesia with monitored anesthesia care to avoid complications related to general anesthesia and control postoperative pain.
Case Report
A 78-year-old female patient (height: 150 cm; weight: 40 kg) was hospitalized for breast cancer and scheduled for hook-wire excision and sentinel lymph node biopsy. The lesion was located 2 cm lateral to the nipple on the right breast. She had a history of cardiopulmonary resuscitation due to severe left ventricular dysfunction with an ejection fraction of 30% that was diagnosed as stress-induced cardiomyopathy caused by pneumonia a year ago. She also had history of congestive heart failure, controlled hypertension, and chronic obstructive lung disease. Her physical status was classified as the American Society of Anesthesiologists III. A recently performed transthoracic echocardiograph showed a left ventricular ejection fraction of 68%. Her pulmonary systolic arterial pressure was 41 mmHg without regional wall motion abnormality. Considering her medical history and the operation site, we decided to perform surgery under regional anesthesia. We provided the patient and her relatives with a detailed explanation and obtained informed consent.
No premedication was administered. Standard monitoring included electrocardiography, non-invasive blood pressure, and pulse oximetry after the patient had entered the operation room. Before the patient was sedated, an ultrasound-guided block (WS80A, Samsung Medison, Korea) using a convex transducer (1–7 MHz) was performed in the left lateral position with the patient raising her arm upward towards her head (Fig. 1). Her skin was disinfected using betadine. The ultrasound probe and cable were protected with a sterile vinyl cover. The probe was placed below the axillary region after checking for the fifth rib. We confirmed the location of serratus anterior and latissimus dorsi muscles and then administered a single injection of 20 ml 0.75% ropivacaine into the inter-fascial plane between the serratus anterior and latissimus dorsi muscles using a 23-gauge 60-mm Quincke-type needle (Kovax-NeedleⓇ, Korea Vaccine Co., Korea) (Fig. 2).

Position of the patient and probe. In-plane technique to serratus anterior plane block.
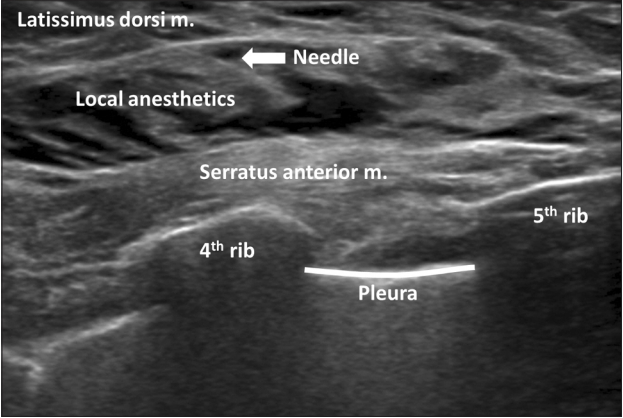
Ultrasound image of the injection of serratus anterior plane block. Local anesthetics were injected between the latissimus dorsi and serratus anterior muscles.
Fifteen min after performing the block, we checked anterolateral hemithorax lateral to the midclavicular line from T2–T7 dermatomes of sensory loss using a cold test with alcohol sponges. The patient then wanted to sleep. We started monitoring anesthetic care using dexmedetomidine and remifentanil. Dexmedetomidine was infused with a loading dose of 1 μg/kg for 10 min followed by a maintenance dose of 0.6 μg/kg/h. Remifentanil 0.1 μg/kg/min was then infused to achieve a Ramsay sedation score of 2–3. Total doses of 65 μg dexmedetomidine and 260 μg remifentanil were administered over 1 h and 5 min.
The operation proceeded to hook-wire excision after sentinel lymph node biopsy. Total operation time was 1 h and 20 min. When dissection of the axillary fascia and pectoralis major muscle was performed, a local infiltration of 5 ml 1% lidocaine was injected to reduce the patient’s topical pain. Her intraoperative vital signs were stable. She was moved to the post-anesthesia care unit after surgery. She had no postoperative delirium or perioperative cardiopulmonary complications such as bradycardia or hypotension.
Patient-controlled analgesia (AutoSelectorⓇ; Acemedical, Korea) was initiated after termination of the surgery and maintained for three days. This was administered as 800 μg fentanyl in a total volume of 100 ml (continuous dose 1 cc/h, bolus 1 cc, and lock time 15 min). No rescue medication for pain was given for 24 h. The patient did not complain of postoperative pain at the surgical site. Her scale of pain at 6 and 12 h post-surgery was 0–1/10 on a numeric rating scale.
Discussion
This case demonstrated the use of serratus anterior plane block as primary anesthesia to avoid cardiopulmonary complications related to general anesthesia and control postoperative pain. Monitored anesthesia care was administrated to reduce the patient’s anxiety and prevent possible pain induced by an incomplete block.
Blanco et al. [2] first described the regional anesthetic technique of serratus anterior plane block injected above or below the space of the serratus anterior muscle. This method can block lateral cutaneous branches of T2–T9 intercostal and thoracodorsal nerves. The lateral cutaneous branch of the intercostal nerve is separated from the posterior part of the rib angle. It passes by the serratus anterior muscle. This nerve is divided into anterior and posterior branches. The anterior part of the nerve is responsible for cutaneous innervation up to the midclavicular line [3]. Serratus anterior plane block provides analgesia to the axillary fossa and lateral thorax. Analgesic effects of this method have been reported for breast surgery, thoracotomy, and multiple rib fractures [4–6]. In the present case, the lesion was located on the lateral side of the nipple. For this reason, we applied serratus anterior plane block. However, there were some disadvantages. The serratus anterior plane block alone was unable to anesthetize the entire hemithorax. It could not be used without ultrasound. Furthermore, there is a risk of failure or occurrence of pneumothorax depending on the skill of the administrator [1].
Other conventional techniques, such as thoracic epidural block, intercostal block, and paravertebral block have risks of spinal infection, epidural hematoma, major nerve damage, unintentional neuraxial injection, pneumothorax, epidural or intrathecal spread, and local anesthetic toxicity by vascular puncture [7,8]. In addition, local anesthetics are rapidly absorbed, resulting in relatively high plasma concentration in intercostal, interpleural, and paravertebral block, thus increasing the potential risk of local anesthetic systemic toxicity. The local anesthetic toxicity of serratus anterior plane block is probably lower than alternative techniques as mentioned above. Because this technique is performed under ultrasonic guidance into a less vascularized area [1].
There have been few reports on the use of serratus anterior plane block as primary anesthesia and to control postoperative pain. Bhoi et al. [9] have performed wire-guided excision using serratus anterior plane block with 30 ml 0.375% ropivacaine and light sedation with propofol. In their study, the location of the breast mass was not noted, and 1 g of paracetamol was used for postoperative analgesia after 6 h. Abdallah et al. [4] have compared three groups, namely general anesthesia alone, general anesthesia with Pecs I block, and general anesthesia with serratus anterior plane block in a cohort study. They found that Pecs I and the serratus anterior plane block groups had low rates of postoperative in-hospital opioid consumption and postoperative nausea and vomiting compared to the conventional opioid-based analgesia group after ambulatory breast cancer surgery.
Although there is no clear evidence that regional anesthesia has an advantage over general anesthesia in patient’s long-term outcome, it reduces irritation of the surgical region and stress reactions after surgery, thereby facilitating pain control and reducing opioid use [10].
Regional anesthesia with monitored anesthesia care confers advantages of safe sedation, anxiolysis, and effective pain control. Dexmedetomidine provides sedative and analgesic effects without respiratory depression [11]. It has been reported that using dexmedetomidine in single-injection peripheral nerve block can prolong analgesic duration and reduce opioid consumption without prolonging motor blockade [12]. Also, remifentanil provides analgesic effects during surgical procedures and maintains hemodynamic stability. However, dexmedetomidine is known to have side effects such as hypotension and bradycardia while remifentanil can cause respiratory depression. Therefore, when using additional intravenous anesthesia, an experienced anesthesiologist with continuous patient monitoring and emergency equipment are needed for airway assurance [11].
For the case presented, we performed only serratus anterior plane block and additional local infiltration during surgery. The pain during the dissection of the pectoralis major muscle might have resulted from not blocking both pectoral nerves that innervate this region. This could have been prevented if Pecs I block was additionally performed [13].
Based on our case and previous studies [2,3], it is possible to use serratus anterior plane block when a lesion is located on the lateral side of the nipple. For its application in extensive surgical procedures, further data and additional case reports are needed. Despite this limitation and the lack of many cases, we consider serratus anterior plane block a simple and effective technique that could be used as an alternative method of primary anesthesia in breast surgery.
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Hyeong-Seok Yoon (Conceptualization; Methodology; Resources; Writing–original draft)
Byoung-Woo Yu (Methodology)
Young-Mu Kim (Resources)
Jae-Ho Lee (Resources)
Won-Uk Koh (Writing–review & editing)
Hong-Seuk Yang (Supervision; Writing–review & editing)