Anesthesia and sedation outside of the operating room
Article information
Abstract
Due to rapid evolution and technological advancements, medical personnel now require special training outside of their safe zones. Anesthesiologists face challenges in practicing in locations beyond the operating room. New locations, inadequate monitoring devices, poor assisting staff, unfamiliarity of procedures, insufficient knowledge of basic standards, and lack of experience compromise the quality of patient care. Therefore, anesthesiologists must recognize possible risk factors during anesthesia in nonoperating rooms and familiarize themselves with standards to improve safe practice. This review article emphasizes the need for standardizing hospitals and facilities requiring nonoperating room anesthesia, and encourages anesthesiologists to take the lead in applying these practice guidelines to improve patient outcomes and reduce adverse events.
Introduction
Nonoperating room anesthesia (NORA) refers to administration of sedation/anesthesia outside the operating room to patients undergoing painful or uncomfortable procedures [1]. These procedures are increasing due to technological developments in medical equipment, proficiency of proceduralists, and medically challenging patients. Common procedures include radiology, gastrointestinal imaging, diagnostic/therapeutic interventions, pediatric cardiac catheterization, psychiatric treatment, and dentistry. Anesthesiologists are frequently asked to provide NORA in these remote locations, but sometimes fail to understand the importance of standards regarding equipment, personnel, and facilities associated with safety. Despite the many studies regarding anesthetic practice in remote locations, those of high quality are lacking.
To provide safe and qualified anesthetic care in the NORA, it is important for anesthesiologists to construct a systemic, uniform structure throughout an institute that contains all provisions of all categories of anesthetic care. Such criteria must be applied equally throughout the hospital, not only to ensure the patient's safety but also to guarantee the safety of health-care providers. Because anesthesiologists providing NORA are responsible for the safety of the patient as well as their own, these standards should not be neglected. This review discusses possible problems and risks associated with sedation and anesthesia when performing various procedures outside the operating room and suggests guidelines for provision of safe NORA.
Risk and Problems
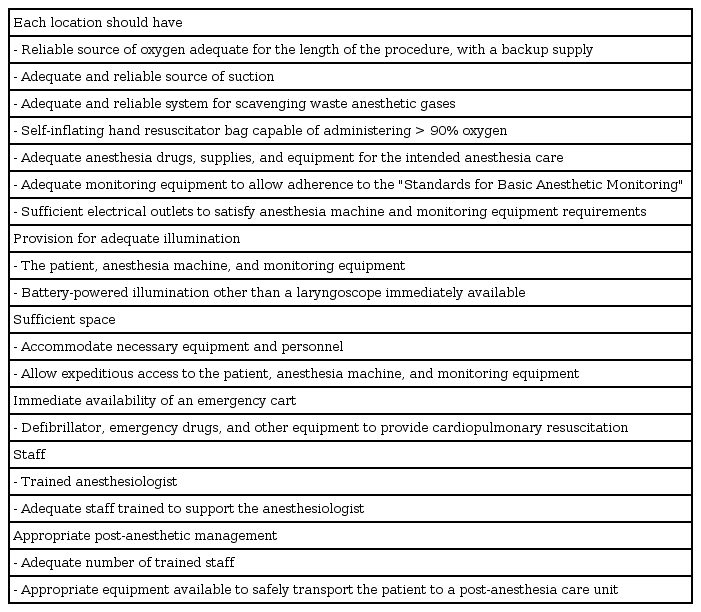
Major unique challenges with NORA include those related to the patient, procedure, and environment. Physicians who are unfamiliar with NORA typically underestimate the fact that patients undergoing procedures involving new and advanced technological equipment are at higher risk. These patients include pediatrics, geriatrics, and medically challenging patients who are too weak for surgical management but able to obtain some benefit from a procedure [2]. Whether the procedures (or surgeries) performed by NORA are simple or not, each patient should be prepared in accordance with general anesthesia because the sedation can be converted to general anesthesia at any time. The anesthesiologist must understand the nature of the procedure, including the position of the patient, how painful the procedure will be, and how long it will last. In addition, prior discussion with the proceduralist must include contingencies for emergencies and adverse outcomes. Other staff must be trained to assist or carry out immediate cardiopulmonary resuscitation. Unfamiliar locations, lack of monitoring devices, inadequately trained or insufficient staff, and unavailable medication or equipment in emergency situations places both patients and anesthesiologists at risk. Accordingly, the American Society of Anesthesiology (ASA) has provided minimal guidelines for anesthesia in the nonoperating room to improve the quality of patient care (Table 1) [3].
Guidelines for Non-operating Room Anesthesia
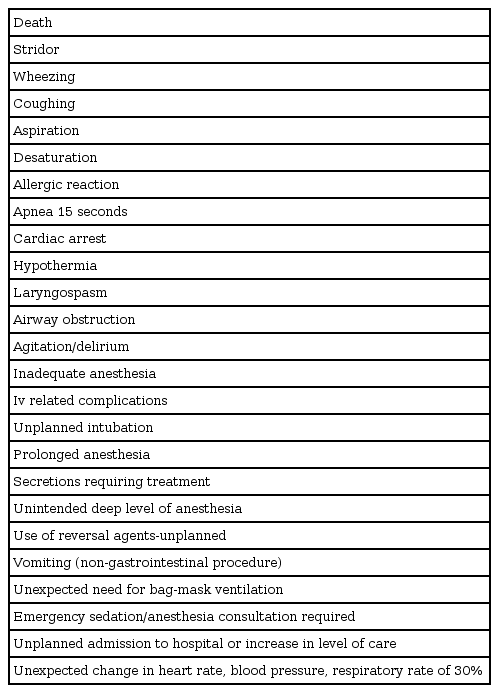
Studies dealing with errors contributing to anesthetic mortality have been performed. In 1961, Dripps et al. [4] reported that human errors accounted for 87% of 80 deaths due to anesthesia, while Edwards et al. [5] reported that human errors accounted for 83% of 589 deaths in 1956. Although anesthesiologists are aware of potential risks in most cases, the process has to be identified when hazardous results occur to decrease human error. In addition, due to the increase in NORA claims over the past decades, interpretation of data is critical. A modified critical-incident analysis by Cooper et al. [6] cited that inadequate total experience or familiarity with equipment/monitoring, poor communication with the team, haste, inattention/carelessness, and fatigue can contribute to critical incidents. Complications from NORA range from mild difficulties to death (Table 2). In a closed claims review by Robbertze et al. [7], half of NORA claims involved the gastrointestinal unit, while 25% involved diagnostic imaging and the other 25% involved cardiologic procedures. NORA also carries a higher severity of injury and mortality rate than that of conventional operating room anesthesia. Using the Korean Society of Anesthesiologists (KSA) database covering case files from July 2009 to June 2014, the KSA Legislation Committee analyzed all anesthesia cases to identify specific patterns of anesthesia-related injury [8]. Although cases related to general anesthesia were most common, sedation cases were similarly prevalent, accounting for 37.1% of all cases. Complications due to sedations were reported avoidable/possibly avoidable in 34 out of 39 cases. Results also showed that in 92.3% of sedation cases (36/39), sedation was provided simultaneously by non-anesthesiologist(s). These data reflect the importance of sedation training and management of adverse events during NORA.
Complications of Non-operating Room Anesthesia
Patients and Staff
Patients
NORA can be applied not only to the general population undergoing diagnostic procedures but also to patients who are too ill to be considered for surgery. Closed claims analysis of NORA reported that most of the patients were of extreme age [7]. Sixty-one percent were classified as ASA 3 to 5, and 38% of adults were older than 70 years. It is interesting that older and weaker patients were more closely associated with monitored anesthetic care claims compared with general anesthesia claims [9]. Another closed claims analysis of 13 patients suggested that the anesthetic risk may significantly increase in patients above the ASA classification 1 [10], indicating that patients requesting NORA should be fully assessed before administering anesthesia/sedation.
Staff
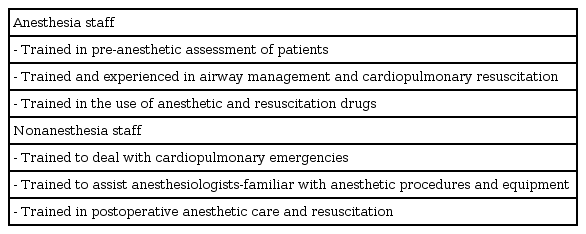
It is recommended that the anesthesiologist who delivers deep sedation or anesthesia should be trained in airway rescue and management [11] (Table 3). Complications from anesthesia have decreased significantly, and the presence of board-certified anesthesiologists have contributed to the decrease in death and disability caused by perioperative events [12]. Abenstein and Warner [13] reported that complication rates did not increase, but the rate of death and failure-to-rescue were greater when care was not directed by anesthesiologists, demonstrating that 30-day morbidity and mortality were lower when anesthesiologists directed anesthesia care.
Personnel Requirements for Non-operating Room Anesthesia
Anesthesiologists must be aware that conducting anesthesia or sedation outside the operating room increases the risk of adverse events. Most commonly, near miss or critical events occur due to operator error or lack of rescue systems [14]. Insufficient or inadequately trained staff can also cause critical complications in NORA settings. Even with an anesthesiologist present, the rate of morbidity and mortality will increase if personnel in the radiology or endoscopy department are unfamiliar with anesthesia or cardiovascular resuscitation. When performing NORA, the anesthesiologist must ensure that participating staff are adequately trained to assist in anesthesia as well as cardiopulmonary resuscitation.
Procedures
NORA is required for diagnostic imaging, invasive radiological procedures, cardiac catheterization, endoscopy, and various surgical procedures including endovascular aortic repair. Therefore, cooperation with many different specialists in various locations for NORA is required.
Neuroradiology procedures
Diagnostic and interventional radiology procedures include embolization of cerebral aneurysms and vascular malformation. These procedures are not typically painful, but general anesthesia is preferred for better outcomes in the event of an unexpected complication during the procedure [15]. It is the responsibility of the anesthesiologist to ensure that the patient does not move during the procedure, assist in treatment of unexpected complications, transport patients from the procedural room to the recovery room or intensive care unit, facilitate rapid awakening, optimize cerebral blood flow, control perfusion pressure, maintain intracranial pressure, monitor fluid status, monitor blood pressure, and monitor body temperature [1617]. It is important for the anesthesiologist to communicate with the radiologist or the neuro-interventionist regarding not only routine procedures but also disasters.
Cardiac catheterization procedures
Although there is no ideal anesthetic technique for cardiac catheterization laboratories, it is important for the anesthesiologist to minimize the effects of anesthetics on the cardiovascular system. Discussing with the cardiologist the type of anesthesia to be delivered may be helpful. When percutaneous coronary intervention is performed on patients who are in respiratory distress or hemodynamically unstable condition due to acute myocardial infarction, anesthesiologists are usually required [18]. Repair of atrial septal defects or ventricular septal defects require general anesthesia with endotracheal intubation and transesophageal echocardiography. Pediatric cardiac procedures differ from those performed in adults due to the type of disease and structure of the abnormal heart. The incidences of cardiac arrest and death have been reported as 0.49 and 0.08%, respectively [19], and even higher in patients with pulmonary hypertension [20].
Pediatric sedation and anesthesia
Pediatric NORA may require more immobility, deep sedation, and general anesthesia compared to adults. It is required for children who cannot endure the long and/or uncomfortable procedures [14]. These requests continue to increase as invasive surgical procedures are thought to be the last resort and noninvasive procedures are preferred. Using mainstream capnography, pediatric patients who require sedation for short procedures or imaging evaluation but do not require intubation can avoid undetected alveolar hypoventilation [21]. Another study reported that pulse oximetry could detect oxygen desaturation more sensitively compared to capnography [19]. However, current practice of monitoring ventilation with only pulse oximetry is becoming unreliable [20], and the use of both pulse oximetry and capnography is recommended. Withholding oxygen to detect hypoventilation is ill-advised [22], and anesthesiologists must not disregard using a capnometer or assisting supplemental oxygen.
Gastrointestinal endoscopy
Potential risks include hemodynamic instability due to limited cardiovascular reserve in the elderly population, dehydration resulting from bowel preparation, and vagal responses due to distention of the gastrointestinal tract. Patients are at risk of aspiration due to gastric bleeding or consumption of large amounts of bowel preparation agents, while access to the airway may be compromised due to prone positioning, dark rooms, or endoscopy itself, which blocks the airway [7].
The most common procedures include upper gastrointestinal endoscopy and endoscopic retrograde cholangiopancreatography. Cardiopulmonary complications predominate, while bleeding and perforations are relatively rare. Because these complications are strongly associated with intravenous administration of drugs [23], recommendations for standards of sedation and patient monitoring during GI endoscopy should be part of quality assurance in these units.
Diagnostic imaging procedures
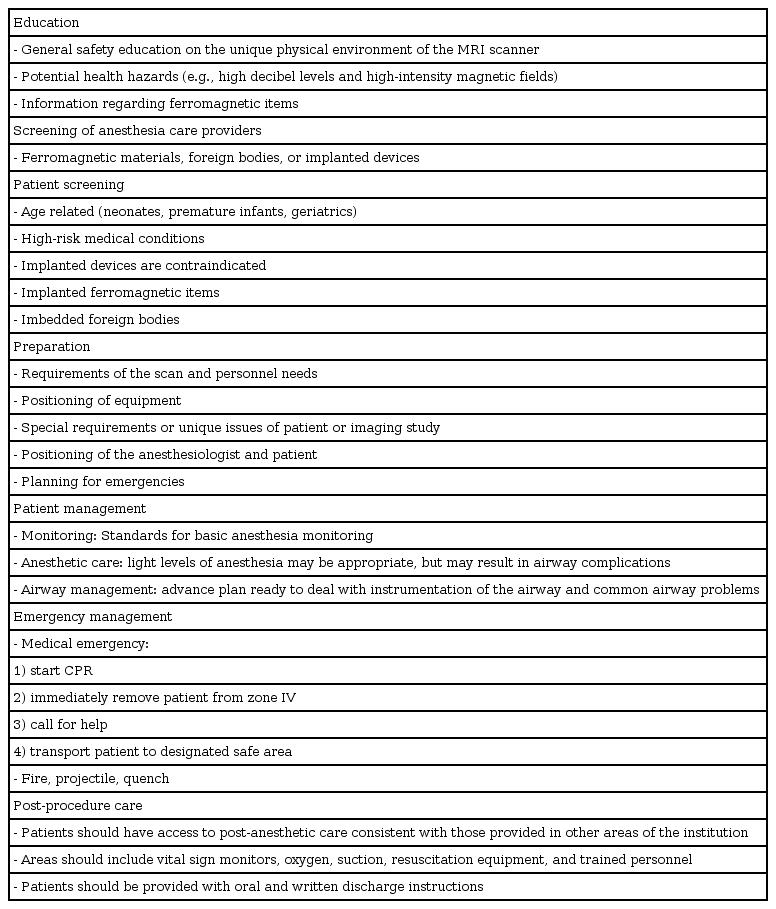
The magnetic resonance imaging (MRI) environment is different from other remote locations providing anesthesia. It possesses strong static and dynamic magnetic fields, high-frequency electromagnetic waves, and a pulsed magnetic field. Other distractions include darkened rooms, high level of noise, heating due to machines, and unintended projectiles. The ASA practice advisory suggests that prior guidelines be supplemented with additional information from the recent scientific literature (Table 4) [24]. Although potential health hazards are lacking in evidence published to date, it is strongly advised that all anesthesiologists are educated on the unique environment of the MRI suite and screened for the presence of ferromagnetic materials, foreign materials, or implanted devices. Patients should also be screened for potential risks, age (neonates, premature infants, or geriatric), medical conditions (impaired respiratory function, hemodynamic instability, obesity, etc.), insertion of foreign materials (eyeliner tattoos, metallic intraocular fragments, piercings), or implanted items (aneurysm clips, prosthetic heart valves, or coronary stents). MRI is contraindicated in patients with implanted electronic devices such as pacemakers, cardioversion defibrillators, or nerve stimulators. All anesthetic plans should be individualized before the procedure to prevent misinformation causing death and select an optimal location for patient observation during anesthetic care. In addition, a backup plan to telephone someone in case of an emergency situation is essential. Monitoring should adhere to the ASA guideline "Standards for Basic Anesthesia Monitoring", and anesthetic equipment and drugs consistent with those in the OR should be available. Because imaging evaluation is not a noxious procedure, light levels of anesthesia may be appropriate, but backup plans for addressing airway complications (obstruction, secretions, laryngospasm, apnea, and hypoventilation) must be made in advance, and suction equipment should be immediately accessible at all times.
Practice Parameters for Magnetic Resonance Imaging
Environment
Demand to cut health care costs has resulted in substitution of invasive for noninvasive surgical procedures, requiring anesthesiologists to work in new locations in the hospital [25]. Because the majority of anesthesia training takes place in the OR, it is important for anesthesiologists to care for patients outside their safe zone. However, without supportive systems and standards, the anesthesiologist must be able to refuse to perform anesthesia or sedation in locations where safety is not guaranteed. Standards regarding basic monitoring and equipment for NORA are outlined in Table 5 [14].
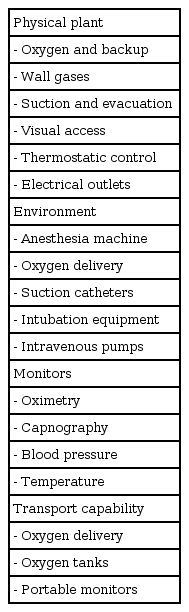
Monitors and Equipment for Non-operating Room Anesthesia
Physical environment
The physical environment of the nonoperating room itself, with unfamiliar equipment and monitors located in remote sites from the OR, restricts patient visualization and accessibility. Sometimes, because the frequency of NORA is lower than that of operating room anesthesia, these locations are equipped with older or malfunctioning machines and resuscitation tools. Limiting access to the patient due to crowding of such bulky machines and equipment is dangerous, so active participation of anesthesiologists during construction or remodeling of a facility is critical.
Monitoring and equipment
Basic monitoring for NORA does not differ from anesthetic monitoring in the operating room. Closed claims are frequently judged as having substandard care and being preventable by better monitoring [7]. The anesthetic machine is by far the most important monitoring machine with which the anesthesiologist must be familiar. Most malpractice is caused not by the skill of the anesthesiologist but because of malfunctioning of ventilators due to negligent checkup, causing patient death. Because the functional life of an anesthesia machine depends on the manufacturer's ability to supply replacement parts, the biomedical department and facility administrator should plan a budget to replace machines nearing the end of their 10-year life cycle [26]. Maintenance and repair should also be performed by a qualified medical service company and not by the biomedical department of the institution because the personnel in these departments may not have the proper education, training, or service experience to repair and maintain such critical equipment [26].
Lighting
Lighting is also a problem, because most rooms are dimly lit to provide a better view of the procedure on screen. Cable wires and dimly lit rooms can result in accidents. Potentially dark areas must be equipped with supplemental lighting to ensure that the anesthesiologist or other staff working in that area, or even a patient, does not trip and suffer a leg fracture. Alternative power supplies should be sought and the possibility of electrical interference investigated to address interruptions in the principal electrical supply.
Radiation exposure
The anesthesiologist is exposed to high levels of radiation in the radiology intervention room [27] during fluoroscopy and must wear proper protective lead aprons and thyroid shields throughout the procedure [28]. Szarmach et al. [29] reported that radiation safety among medical staff was lowest in the surgical ward. Physicians as well as trainees and students should be equipped with dosimeters where there is evident radiation exposure, despite their low radiation exposure. Further protection for the patient from radiation exposure is also warranted. Because the risk of prenatal radiation exposure is also of concern, effective protection for pregnant or lactating staff is essential [30].
Waste gas
In locations in which inhalation agents are used, gas-scavenging systems must be installed to prevent air contamination and further exposure of personnel. Trace amounts of waste anesthetic gas cannot be eliminated, but can be controlled by measuring exposure levels on a yearly basis to be congruent with Occupational Safety and Health Administration standards [26]. A survey comparing obstetric complications between pediatric and non-pediatric anesthesiologists suggested that the prevalence of spontaneous abortion was higher in anesthesiologists with a proportion of pediatric patients of >75% [31]. Plausible explanations included increased exposure to anesthetic gas during induction and the use of uncuffed endotracheal tubes. Since the first report of increased spontaneous abortion (18 of 31 pregnancies) in the Soviet Union in 1967 [32], a 1974 study in the United States supported by the ASA suggested that female operating-room personnel were at increased risk not only of spontaneous abortion but also of congenital anomalies [33]. However, after the 1970s, studies regarding increased risks of miscarriage, congenital abnormalities, or preterm deliveries reported no effects, possibly due to the implementation of waste anesthetic gas (WAG) scavenging systems [34] and introduction of new gases such as sevoflurane and desflurane, which are less toxic and explosive than chloroform or cyclopropane. As the number of female anesthesiologists increases, exposure to anesthetic gases and the risk of obstetric complications will also increase. Therefore, female anesthesiologists must be aware of relevant information for their protection and find ways to minimize exposure or practice good anesthetic techniques, such as the use of cuffed endotracheal tubes in place of uncuffed tubes, in terms of planning of or during pregnancy. WAG-scavenging systems should be provided in areas involving exposure to anesthetic gases to protect not only the anesthesiologist but also other personnel working in the area.
Complications Regarding Patient Management
Respiratory complications
A closed claims report by Caplan et al. [35] emphasized the need for a thorough evaluation of the airway, based on claims for difficult tracheal intubation preventable with better monitoring. It is evident that respiratory depression is more frequent during sedation or anesthesia outside the OR, so anesthesiologists must be familiar with the difficult airway algorithm [36]. Respiratory complications are associated with nonvigilance, choice of an inappropriate anesthetic technique, use of nonanesthesia staff in complex medical cases, esophageal intubation, and unexplained bradycardia [7]. A survey carried out in the Oxford region to determine the preferred technique for the management of unanticipated difficult intubation reported that 10% of anesthesiologists had no backup plan [37]. The most common specific damaging event in NORA claims were inadequate oxygenation/ventilation [7], which are preventable with better monitoring, such as pulse oximetry and capnography. Because anesthesiological skills such as endotracheal intubation require much training, each procedure must be continuously rehearsed to achieve a reasonable success rate [38]. Techniques in reducing deoxygenation due to apnea and/or difficult airways such as preoxygenation should be performed [39], especially in patients with severe diffuse emphysema [40] or the elderly [41]. Maintaining an appropriate seal between the face mask and face is also important in oxygen delivery [42].
Hypothermia
Hypothermia occurs frequently in areas heavily air-conditioned to avoid equipment overheating. Pediatric patients are vulnerable to hypothermia when exposed for prolonged periods, which may cause dangerous side effects [43]. Methods of reducing hypothermia include warming blankets with surface heating, administering heated fluids, and preemptive warming in volunteers [44] and patients [45]. Although massive bleeding is rare in the NORA setting, mild hypothermia is known to increase surgical blood loss and the risk of transfusion [46], emphasizing the importance of maintaining normothermia in anesthetized patients.
Aspiration
Aspiration of gastric contents is an issue when administering sedatives, hypnotics, or anesthetics because protective airway reflexes are blunted. Preoperative fasting is as important as in patients preparing for elective surgery. However, prolonged fasting can cause dehydration and hypocalcemia in children [47], so fluid therapy should be performed according to the current practice guidelines [48]. Clear fluids are allowed 2 hours before induction, whereas solids regarded as a meals are withheld for at least 8 hours.
Hypovolemia
Patients preparing for colonoscopy on fluid restriction and a strict diet to prevent aspiration are at risk of dehydration, hypovolemia, and may show vigorous responses to vasodilating or cardiac depressant drugs. Thus, maintenance of a sufficient volume status before the procedure by prehydration and slow injection of drugs may prevent adverse events [12].
Postoperative nausea and vomiting (PONV)
Postoperative nausea and vomiting is one of the primary causes of unplanned hospitalization, and is easily recognizable and preventable. Although Apfel's simplified risk score for predicting PONV [49] is imperfect [50], it is effective [51] in discriminating susceptible patients. An experimental study by Sarin et al. [52] improved preexisting scores for predicting PONV in ambulatory surgery patients.
Postoperative Care
Postoperative or post-sedation care similar to that after general anesthesia must be provided in a standardized manner. Preventable adverse respiratory events occur during the recovery or postoperative periods, so strict surveillance is necessary until full recovery [53]. A post-anesthetic or post-sedation score must be given unless the patient is taken directly to an intensive care unit, where intensive monitoring takes place.
Conclusion
The proceduralist and anesthesiologist will have a general idea of the important aspects that should be considered while performing NORA to decrease complications associated with the procedure and anesthesia. However, because each procedure is different, additional standards according to specific procedures should be implemented. Anesthesiologists must acknowledge malpractice or negligence in the past and cooperate to develop guidelines for future safe practice of anesthesia outside the operating room. This does not necessarily require remodeling diagnostic or intervention rooms or GI suits, or purchasing new and expensive monitoring machines and equipment. Above all, involvement of a dedicated and vigilant anesthesiologist is the best way of preventing adverse events.