Unilateral laryngeal hematoma after combined carotid endarterectomy and off-pump coronary artery bypass grafting surgery
Article information
Airway injuries are potentially serious and costly adverse events of anesthesia care. Although the majority of airway injuries are not serious; 5% of the injuries are permanent and disabling, with 8% of those resulting in death [1]. According to an epidemiological study involving 563,190 patients, the risk of airway injury for patients undergoing major surgical procedures was approximately 1 in 500 [2]. We present a case in which laryngeal hematoma developed postoperatively after simultaneous carotid endarterectomy (CEA) and off-pump coronary artery bypass graft (OPCAB) surgery.
A 75-year-old male was scheduled for concurrent left CEA and OPCAB, under general anesthesia. His medical history included diabetes mellitus, hypertension, and lower extremity vascular occlusive disease. He was taking aspirin and clopidogrel for anticoagulation medication. He was 163 cm in height and 61 kg in weight. There were no physical signs predicting difficulties in airway management.
General anesthesia was induced with midazolam, etomidate, sufentanil and rocuronium. Orotracheal intubation was successfully done in a single attempt with a Macintosh laryngoscope. His airway showed Mallampati class I and Cormack-Lehane grade I under direct laryngoscopy. A size 8.0 mm cuffed endotracheal tube (Hi-Lo™, Mallinckrodt Medical, Athlone, Ireland) was used and fixed on the right side of the mouth.
First, left carotid endarterectomy was started by a vascular surgeon. After the carotid vessel identified, 4,000 units of heparin were administered intravenously. The CEA procedure took an hour. After the vascular surgery was finished, an adult multiplane 7 to 2 MHz transesophageal echocardiography (TEE) probe (Philips iE33 × 7-2t xMATRIX array, Tip; 1.7 × 3.8 cm WxL, Shaft; 1 cm diameter, 1 m length) lubricated with lidocaine jelly (Arlico Lidocaine HCI Jelly 2%) was placed gently into the esophagus. When the TEE probe was first inserted, there was a little resistance. However, the insertion proceeded easily after elevation of the mandible. There was no evidence of oropharyngeal mucosal bleeding. Another bolus of 9,000 units of heparin was injected during the OPCAB after dissecting the internal mammary artery, and activated clotting time (ACT) was 445 seconds. At the end of the surgery, 50 mg of protamine was given to reverse the heparin and the ACT was 103 seconds. The TEE was removed 7 hours after its insertion. There was no blood at the tip of the TEE probe when it was removed. The total anesthesia duration was 10.5 hours.
After successful the operation, he was transferred to an intensive care unit and enoxaparin 30 mg was subcutaneously injected. The next morning, he was extubated without any further complications. Total intubation time was 24 hours. Aspirin 100 mg and clopidogrel 75 mg was orally taken and enoxaparin 30 mg was subcutaneously injected on postoperative day (POD) 1. No further coagulation chemistry exam was done after the surgery. After an uneventful ICU care, he was transferred to the general ward, on POD3. However, on POD 7, the patient complained about hoarseness, sustained dysphagia and blunting of tongue movement. Consequently, he was referred to an otolaryngologist. He underwent flexible nasopharyngolaryngoscopy, which detected an arytenoid submucosal hematoma on the left side of the larynx, around a vestibular fold and cuneiform cartilage (Fig. 1A). However, both vocal cords were mobile, and oxygen saturation was maintained within normal range (around 97%). Bedside intubation and a tracheostomy set were prepared for a possible emergent situation. Careful observation was continued and anticoagulantion therapy including aspirin and clopidogrel was discontinued for 3 days. On POD 10, a subsequent flexible endoscopic examination was performed again (Fig. 1B). It revealed that the hematoma was slightly decreased and the subjective symptoms of the patient were somewhat resolved. The patient was discharged on that day. The patient visited the outpatient clinic for routine follow up on POD 20. Fortunately, his laryngeal symptoms were all relieved.
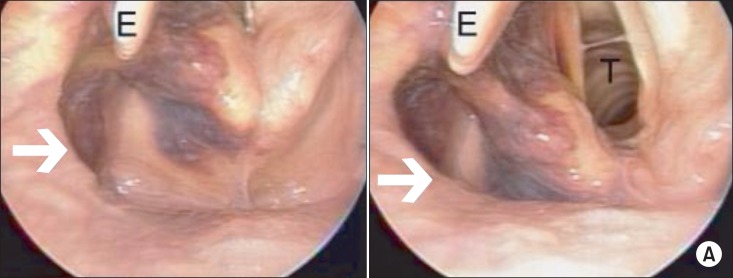
Endoscopic view of the larynx demonstrating extensive submucosal hematoma (arrow) on the left side of the larynx on the postoperative 7th day. Epiglottis (E), vocal cords and trachea (T) are visualized.
In this case, the laryngeal hematoma could be related to all the above mentioned situations, such as the endotracheal intubation, intravenous heparinization, TEE instrumentation and anticoagulant medication. Although intubation trauma accounts for most cases of internal laryngeal injury, this alone does not fully demonstrate the laryngeal trauma. And besides, in our case, the airway of the patient was Mallampati class I, thus he was easily intubated without difficulties.
Moreover, the traumatized area followed the same direction as that of the TEE. And there was a little resistance during TEE insertion which was relieved after elevation of the mandible. This resistance could be related to the laryngeal damage. All things considered, we retrospectively deduced that the association between the laryngeal hematoma and intravenous heparin injection, along with TEE instrumentation, rather than the endotracheal intubation was responsible for the hematoma. In addition, anticoagulation could be linked to hematoma formation. Laing et al. [3] reported spontaneous vocal cord hematoma after thrombolytic therapy with 10,000 units of intravenous heparin.
In conclusion, this case reports a laryngeal hematoma, following a concurrent CEA and OPCAB surgery, with intravenous heparin injection and TEE instrumentation during the operation. Careful instrumentation and a thorough understanding of the consequences of the operation are certainly necessary to reduce possible complications. When there is resistance from inserting a TEE probe in an anesthetized patient, it is important to avoid forcing the TEE.
We have reviewed our experience to emphasize the importance of a meticulous observation of postoperative airway complications as well as a careful practice of endotracheal intubation and TEE instrumentation after systemic heparinization. In addition, if patients complain of laryngeal or pharyngeal symptoms, a thorough early exam should be done especially when anticoagulation therapies are being used.
