Introduction
General anesthetic techniques that are divided into inhalation and intravenous (IV) anesthesia can affect postoperative recovery. The most well-known difference between the two techniques may be the decrease in postoperative nausea and vomiting (PONV) for propofol-based total intravenous anesthesia (TIVA) compared with inhalation anesthesia [1]. Previous studies have also reported that propofol-based TIVA yields better outcomes than inhalation anesthesia in terms of postoperative morbidity [2ŌĆō4]. Further, propofol-based TIVA may be associated with improvements in oncologic outcomes compared with inhalation anesthesia [5]. However, propofol-based TIVA has not yet been strongly recommended in perioperative guidelines due to the lack of strong evidence [6,7].
Standardized evidence-based anesthesia protocol can improve postoperative recovery and clinical outcomes [8]. However, with the introduction of minimally invasive surgery and advances in perioperative medicine, the incidence of postoperative morbidity and duration of hospital stay have decreased significantly. Therefore, it is becoming increasingly difficult to identify whether treatments significantly affect postoperative outcomes using these traditional variables [9]. Furthermore, these variables have been reported to deviate greatly from patient-perceived postoperative recovery [10]. In contrast, the Quality of Recovery-15 (QoR-15) questionnaire can provide a meaningful and overall assessment of patient-centered postoperative recovery [11] and has been recommended as an endpoint in clinical studies investigating postoperative recovery [12,13].
This randomized controlled trial (RCT) aimed to investigate differences in postoperative quality of recovery after minimally invasive nephrectomy between two main general anesthesia techniques using the Korean version of QoR-15 (QoR-15K) [9]. We hypothesized that propofol-based TIVA would improve early postoperative recovery compared to desflurane anesthesia.
Materials and Methods
This prospective, randomized, single-blinded trial was approved by the Institutional Review Board (IRB) of Seoul National University Hospital (2003-177-1113). Before patient enrollment, the study protocol was registered with ClinicalTrials.gov (NCT04447105). This study was performed in accordance with Good Clinical Practice Guidelines and Consolidated Standards of Reporting Trials (CONSORT) guidelines [14]. The study adhered to the tenets outlined in the 2013 Declaration of Helsinki, and all patients provided written informed consent. Enrollment occurred at the university teaching hospital in South Korea between June 2020 and July 2021.
Patient selection
We screened adult patients (age: 19 to 80 years) with renal cancer scheduled to undergo elective minimally invasive nephrectomy for study eligibility. Patients with the following features were excluded: 1) American Society of Anesthesiologists (ASA) physical status Ōēź III, 2) non-malignancy or receiving concurrent surgeries, 3) history of allergic reaction to anesthetics or analgesics included in the protocol of this study, 4) history of chronic pain defined as having taken analgesics or anticonvulsants for more than three months, 5) requirement of mechanical ventilation for Ōēź 2 h after surgery, 6) poorly controlled psychological diseases that precluded cooperation, and 7) difficulty understanding the informed consent process or questionnaires in the Korean language.
Randomization and blinding
After enrollment, block randomization (block size: 4 and 6) was used to randomly allocate patients to the propofol-based TIVA (TIVA group) or desflurane anesthesia (DES group) at a 1:1 ratio using R software (Version: 3.6.1, R Development Core Team). Randomization was conducted by an anesthesiologist who was not involved in this study. Patients and the outcome assessor were blinded to group assignments, but the attending anesthesiologists could not be blinded due to the differences in intraoperative anesthetic techniques between the groups. Information regarding the allocation order stored in an opaque envelope was delivered to the attending anesthesiologists on the day of surgery.
Anesthetic management
Without premedication, anesthesia was induced with a 1.0ŌĆō2.0 mg/kg bolus dose of propofol (Fresofol MCT 1%, Fresenius Kabi Korea Ltd.) and maintained with desflurane (Suprane, Baxter Healthcare) in the DES group. In the TIVA group, anesthesia was induced and maintained with a target-controlled infusion (TCI) of propofol (Fresofol MCT 2%, Fresenius Kabi Korea Ltd.) using an infusion pump (Orchestra┬«; Fresenius Vial) using the Marsh pharmacokinetic model. Other than the anesthetics used to maintain general anesthesia, the following anesthetic management procedure was identical in both groups. During induction, 5 mg of dexamethasone and 0.075 mg of palonosetron were administered for PONV prophylaxis. Remifentanil was started using a TCI using the Minto pharmacokinetic model with a target of effect-site concentration of 3.0 ng/ml, then was adjusted to maintain arterial pressure within 20% of baseline ward pressure. Rocuronium was used to maintain deep neuromuscular block under monitoring with acceleromyography. The bispectral index and mean arterial blood pressure were maintained within 40ŌĆō60 and 60ŌĆō90 mmHg, respectively. For early postoperative pain control, 1 g of IV acetaminophen was injected over 30 min at the point of insertion of the JacksonŌĆōPratt drains. A loading dose of IV fentanyl (50 ┬Ąg) was administered following skin closure for IV patient-controlled analgesia (IV-PCA). Patients were extubated after administration of sugammadex for the reversal of neuromuscular blockade, following which they were transferred to the post-anesthesia care unit (PACU).
Postoperative management in the PACU and ward
Patients in the PACU were permitted to utilize IV-PCA delivered via a semi-electronic infusion pump (AutoMed 3200┬«, ACE Medical). The bolus dose of fentanyl and lockout interval were 20 ╬╝g and 10 min, respectively, and there was no basal infusion. Patients were instructed to use IV-PCA when they had a numeric rating scale (NRS) pain score Ōēź 3. At the PACU, patients who reported a pain level of NRS Ōēź 7 were given 50 ╬╝g of IV fentanyl, regardless of whether they were using IV-PCA or not. PONV was categorized into four groups: no symptoms, mild (occasional symptoms but tolerable without medication), moderate (frequent or persistent symptoms requiring medication), and severe (vomiting). Rescue antiemetics were administered upon the patientŌĆÖs request or when they reported moderate to severe PONV. Such treatment involved the administration of 10 mg of metoclopramide in the PACU. In the ward, initial rescue antiemesis treatment involved the administration of 0.3 mg of ramosetron, followed by 10 mg of metoclopramide as the second rescue treatment when necessary. Water sips were permitted on the morning of the postoperative day (POD) 1, and a liquid and soft-blended diet were initiated in stages on the same day. An oral extended-release tramadol 37.5 mg/acetaminophen 325 mg combination tablet was routinely administered at 12-h intervals from the morning of POD 1 until discharge. If a patientŌĆÖs pain persisted at a rating of NRS Ōēź 7 despite active use of IV-PCA (four times/h), a rescue analgesic was administered. During the first 8 h postoperatively, the initial rescue analgesic was 50 ╬╝g of IV fentanyl and then 1 g of IV acetaminophen. After taking a routine oral analgesic (the morning of POD 1), the initial rescue analgesic was 650 mg of oral acetaminophen, and an alternative rescue analgesic was 50 ╬╝g of IV fentanyl. However, when the patient complained of PONV, 1 g of IV acetaminophen was administered at the discretion of the attending physicians. Ward ambulation was also initiated on the morning of POD 1 after radical nephrectomy and 24 h after partial nephrectomy. The Foley catheter was removed at the start of ward ambulation. During the follow-up period (until POD 3), transdermal analgesic patches, IV opioids other than fentanyl, and oral analgesics other than the tramadol/acetaminophen combination tablet were not allowed.
Outcome measures
The day before surgery, the investigators asked the patients to complete the QoR-15K and the EuroQoL 5-dimension 5-level scale (EQ-5D-5L) to measure baseline status [15]. The QoR-15K consists of 15 short-form instrument items, and these items can be classified into the following five categories: physical comfort (five items), emotional state (four items), psychological support (two items), physical independence (two items), and pain (two items). Each item is evaluated using an 11-point numerical rating scale (0ŌĆō10), and a higher score means a better recovery. The following baseline and intraoperative variables were recorded: sex, age, body mass index, the Physiological and Operative Severity Score for the enUmeration of Mortality and Morbidity (POSSUM score) [16], ASA physical status, Apfel score [17], type of surgery (radical vs. partial), type of approach (laparoscopic vs. robot-assisted), estimated blood loss (ml), intraoperative crystalloid and colloid administration (ml/kg), intraoperative transfusion, operative time (min), and intraoperative remifentanil consumption (╬╝g). The primary outcome was the QoR-15K score measured at 24 h postoperatively. Secondary outcomes included the QoR-15K score measured at 48 h and 72 h postoperatively; the interval of fentanyl consumption during the first 24 h and 24ŌĆō48 h postoperatively; resting and movement-evoked pain intensity using an 11-point NRS at 24, 48, and 72 h postoperatively; the occurrence of PONV at 24, 48, and 72 h postoperatively; and quality of life at three weeks after discharge as measured using the EQ-5D-5L in the outpatient clinic. Considering the confusion caused by certain points of the QoR-15K for respondents [9], all QoR-15K questionnaires were completed under the two experienced investigatorŌĆÖs guidance. In addition, because we determined that the QoR-15K was not suitable for evaluating the quality of recovery after discharge, we opted to use the EQ-5D-5L questionnaire to evaluate the quality of recovery at the outpatient clinic three weeks after discharge. Patients completed the questionnaire after discharge independently without assistance from the investigators. We also compared the administration of rescue analgesics other than fentanyl, serum high-sensitivity C-reactive protein on POD 3 as a systemic inflammatory marker, postoperative complications classified using the ClavienŌĆōDindo classification during hospitalization evaluated at the time of discharge [18], acute kidney injury diagnosed based on Kidney Disease: Improving Global Outcomes criteria [19], and length of hospital stay between the two groups. All outcomes were evaluated by physicians that were not involved in this study and were blinded to the group assignment.
Statistical analysis
Based on our previous study [9], we assumed a QoR-15K score of 95 ┬▒ 20 at 24 h after minimally invasive nephrectomy under inhalation anesthesia. Although we planned to investigate a QoR-15K at 48 and 72 h postoperatively, we could not consider it in the sample size calculation due to the lack of relevant data. Considering a QoR-15K score of 10 as the minimal clinically important difference (MCID) at 24 h postoperatively [20], the sample size calculation using G*Power (version 3.1.9; Franz Faul, University of Kiel) yielded 64 patients per group to achieve a two-tailed significance of 0.05 and a power of 80%. Considering the dropout rate of 15%, a total of 150 patients were required for enrolment.
Continuous variables are reported as the mean ┬▒ standard deviation or median [interquartile range (IQR)] and were compared using StudentŌĆÖs t-test or the Mann-Whitney U test according to the normality of the data. Categorical variables are reported as frequencies or percentages and were compared using the chi-square or FisherŌĆÖs exact test based on their expected frequencies. The effect size and 95% CI were also calculated.
To compare the differences in QoR-15K scores at each time point, including the primary outcome (QoR-15K score at 24 h postoperatively), we used the MannŌĆōWhitney U test. We also performed a generalized estimating equation (GEE) that is more flexible than repeated-measures analysis of variance to analyze repeated QoR-15K score measurements [21]. If there was no significant interaction between the group and time in the GEE, we calculated the adjusted mean difference of the QoR-15K score between the two groups, excluding the interaction term from the model. If a significant interaction between group and time was observed in the GEE, then post hoc pairwise multiple comparisons using least squares mean with the Bonferroni correction were performed to calculate the adjusted mean difference of QoR-15K score between the two groups at each time point. The GEE analysis was also performed, with Bonferroni correction, for each dimension of the QoR-15K.
All tests were two-sided, and the level of statistical significance was set at P < 0.05. All statistical analyses were conducted using R software (Version: 3.6.1, R Development Core Team).
Results
Among 246 eligible patients, 96 were excluded, following which the remaining 150 patients were randomly allocated to the TIVA or DES group (Fig. 1). During the study period, ten patients were additionally excluded due to the cancellation of the operation on the day of surgery (n = 4), ASA Physical Status of III on the day of surgery (n = 1), requirement of mechanical ventilation after massive intraoperative bleeding (n = 1), refusal to complete the questionnaire after surgery (n = 3), and postoperative cognitive dysfunction (n = 1). In total, 140 patients were included in the final analysis. Table 1 summarizes the baseline characteristics of the included participants that did not significantly differ between the TIVA and DES groups, except for the amount of remifentanil administered intraoperatively (median difference: 270 [169, 376] ╬╝g, P < 0.001).
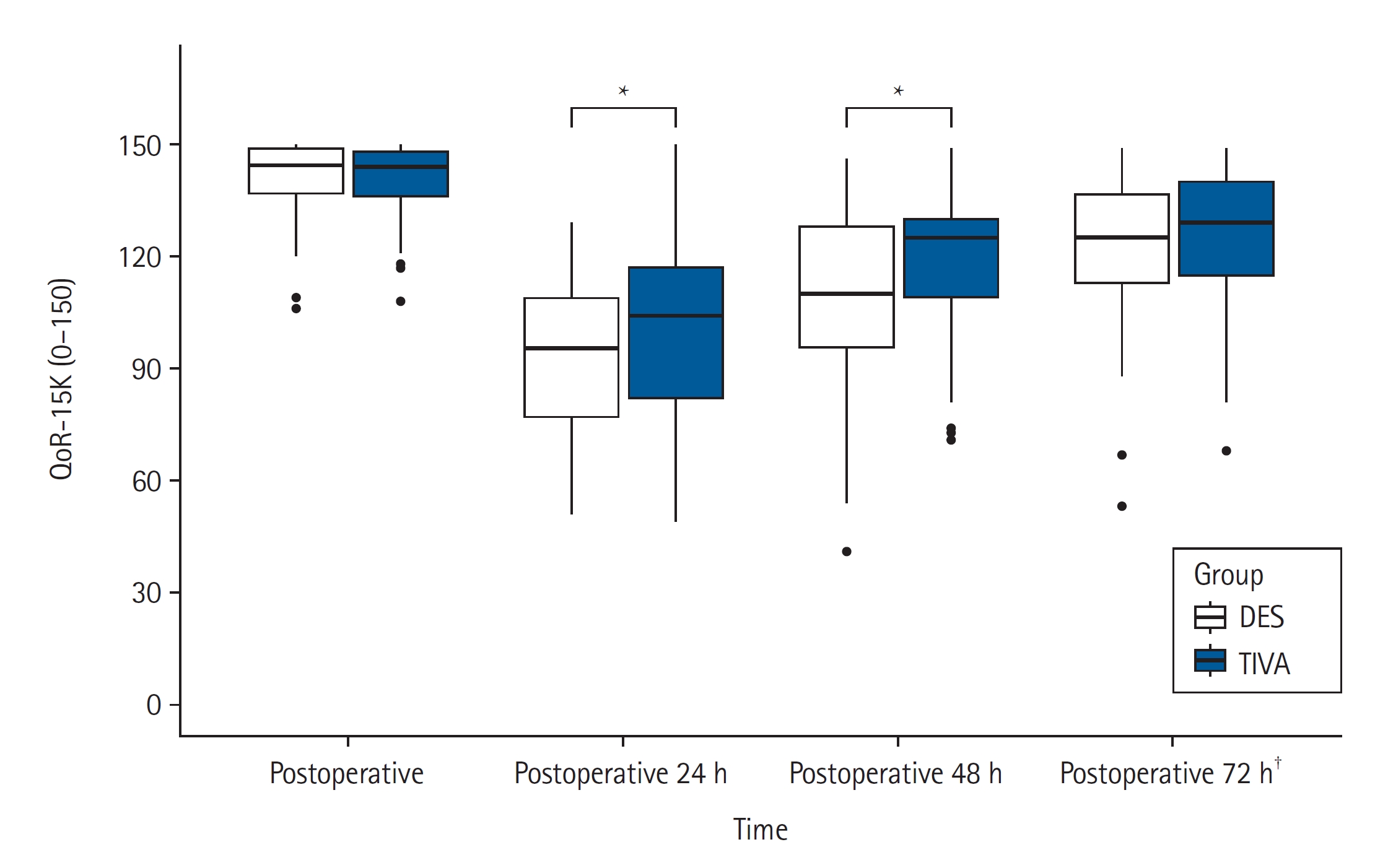
Fig. 2 and Supplementary Tables 1ŌĆō4 show the comparisons of QoR-15K scores between the two groups. Eight patients (TIVA group: n = 5, DES group: n = 3) were discharged before 72 h postoperatively; thus, they could not complete the QoR-15K at that point. The TIVA group showed significantly higher QoR-15K scores at 24 and 48 h postoperatively (24 h: DES, 96 [77, 109] vs. TIVA, 104 [82, 117], median difference 8 [95% CI: 1, 15], P = 0.029; 48 h: DES, 110 [95, 128] vs. TIVA, 125 [109, 130], median difference 8 [95% CI: 1, 15], P = 0.022), however not at 72 h (DES group, 125 [113, 137] vs. TIVA group, 129 [115, 140], median difference 3 [95% CI: ŌłÆ3, 8], P = 0.400). During the entire study period, the GEE revealed significant effects of group (adjusted mean difference 6.2, [95% CI: 0.39, 12.1], P = 0.037) and time (P < 0.001) on postoperative QoR-15K scores, without group-time interaction (P = 0.051). Among the five dimensions of the QoR-15K, only the pain dimension was significantly better in the TIVA group than in the DES group during the study period (Table 2). A significant interaction was observed between time and group in the psychological support and physical independence dimensions, leading to a post hoc analysis. The analysis revealed a significant difference between the two groups only in the physical independence dimension at 24 h postoperatively and in the psychological support dimension at 48 h postoperatively.
Table 3 and Supplementary Table 5 show the comparison of other postoperative outcomes between the two groups. Fentanyl consumption during the first 24 h postoperatively was significantly lower in the TIVA group than in the DES group (adjusted median difference ŌłÆ40 ╬╝g, [corrected 95% CI: ŌłÆ250, ŌłÆ30 ╬╝g], Bonferroni corrected P = 0.008). However, no other postoperative outcomes differed between the two groups. One hundred and four patients (74.3%) completed the EQ-5D-5L questionnaire three weeks after hospital discharge (Supplementary Table 6). There was no significant difference in any item of the EQ-5D-5L before surgery and after hospital discharge between the two groups.
Discussion
The difference in the postoperative quality of recovery between the two groups varied depending on the time after surgery. Although propofol-based TIVA significantly improved the quality of recovery at 24 and 48 h after minimally invasive nephrectomy compared with desflurane anesthesia, their effect size was smaller than the predefined MCID. Furthermore, this difference did not remain at 72 h postoperatively. There was no significant difference between the two groups in any other postoperative clinical outcomes, including quality of life, at three weeks after discharge.
Several studies have investigated the effect of general anesthetic techniques on postoperative recovery using the QoR-40 [22ŌĆō28]. An RCT including female patients undergoing thyroid surgery reported the superiority of propofol-based TIVA for early postoperative recovery, mainly due to the reduction in PONV [22]. However, differences in patient characteristics and insufficient PONV prophylaxis made this result difficult to apply to other surgeries, and subsequent RCTs have yielded conflicting results [23ŌĆō28]. Moreover, in most previous studies, outcomes were assessed only within POD 1, except in two recently published RCTs [27,28]. One involving patients undergoing pancreatectomy reported that postoperative recovery was significantly better on POD 3 in the propofol-based TIVA group than in the DES group [27]. However, the clinical implications of a significant difference only on POD 3 may be debatable, considering the relatively long length of hospital stay following pancreatectomy. Rather, this difference seen only on POD 3 might have resulted from the transient effect of type of general anesthetic techniques, similar to our result. Another recent RCT for laparoscopic hysterectomy reported no significant difference between the two techniques in terms of postoperative recovery [28]. However, the study only included relatively young female patients, making the results difficult to generalize. Additionally, unlike this study, our study found a transient but significant improvement in early postoperative recovery in the TIVA group, consistent with several previous studies [22ŌĆō25].
Our study differs from previous investigations in that we aimed to mitigate the impact of the antiemetic effect of propofol-based TIVA by implementing multimodal PONV prophylaxis in both groups in accordance with recent guidelines [1]. Furthermore, we included patients undergoing minimally invasive cancer surgeries. Given the growing interest in the effects of anesthetic type on oncologic outcomes [5,29,30], our study may provide additional meaningful information regarding anesthetic selection in patients undergoing cancer surgeries. We also reduced the impact of confounding factors on postoperative recovery using a homogeneous sample of patients and a standardized perioperative protocol. Lastly, we used the QoR-15, which has higher clinical feasibility than the QoR-40 [31] and was the first validated measurement for postoperative recovery under the standardized criteria [13]. Therefore, our results may provide more reliable information regarding the effect of general anesthetic techniques on postoperative recovery.
In this study, the main perceived advantages of propofol-based TIVA compared to desflurane anesthesia were its opioid-sparing effect and improvement of pain dimension in the QoR-15K. Propofol may improve postoperative pain through its anti-inflammatory and antioxidant effects and antagonistic effects at NMDA receptors that can play an important role in pain signaling [2,32]. Several meta-analyses have supported the superiority of propofol-based TIVA for improving postoperative pain compared with inhalation anesthesia [2,33,34]. However, since the analgesic effect of propofol-based TIVA can vary depending on the degree of surgical trauma and postoperative pain management, our results should be interpreted cautiously. In an aforementioned RCT that addressed laparoscopic hysterectomy outcomes, no differences in postoperative recovery were observed between propofol-based TIVA and sevoflurane anesthesia [28]. In this study, postoperative pain intensity was low, indicating that propofol-based TIVA may not have induced a significant difference in postoperative pain outcomes. Additionally, regional analgesiaŌĆönot included in our studyŌĆöcan negate the analgesic and opioid-sparing effects of propofol-based TIVA [35], which may further contribute to insignificant differences in QoR-15 scores between the two groups.
Our findings suggested that propofol-based TIVA improved postoperative recovery during the early postoperative period, which is also in line with the opinion of anesthesiologists who participated in a relevant survey (79% somewhat to strongly agreed that TIVA leads to the superior quality of recovery) [36]. However, considering its transient and marginal effect during hospitalization and the time course of postoperative recovery in our patients, it may be difficult to show that propofol-based TIVA leads to significant improvements in other postoperative outcomes.
Our study has several limitations. First, as this study was a single-blinded RCT, some biases may have influenced our results. However, although attending anesthesiologists could not be blinded, the investigator who evaluated postoperative outcomes was completely blinded to the group allocation. Second, the sample size was calculated based on the QoR-15K score at 24 h postoperatively, according to our previous study [9], although this was not sufficiently powered to detect significant differences in other outcomes. Additionally, we considered a QoR-15K score of 10 as the MCID, greater than the previously reported MCID of 8 for the QoR-15 [37]. In the planning stage of this study, we initially considered a QoR-15K score of 8 to be MCID based on the previous study [37]. However, considering that the difference in the QoR-15K scores between the two groups may decrease over time after surgery [22], we had set the MCID of 10 at 24 h postoperatively as the primary outcome that was a greater value than 8. Thus, we recalculated the sample size before patient enrollment after the approval of IRB. Third, our study was conducted at a single tertiary university hospital and thus may not reflect perioperative management at other institutions. Fourth, there was a significant difference in the total amount of intraoperative remifentanil used between the two groups. The type of general anesthesia technique and amount of intraoperative remifentanil could have affected postoperative pain severity and opioid consumption [32]. Although we assumed that this difference would have been due to the vasodilatory or analgesic effect of desflurane [38,39], we found it difficult to explain the mechanism behind this difference from our results. However, since there was no significant difference in postoperative pain severity, but rather, less postoperative opioid consumption in the TIVA group, the difference in intraoperative remifentanil amount would not have had a significant effect on our primary and secondary outcomes. Lastly, since we followed the conventional discharge criteria determined by attending surgeons, this may explain why a significant difference in postoperative recovery during the early postoperative period did not lead to a significant difference in the length of hospital stay. Further research is required to investigate the clinical impact of these two anesthetic techniques under a discharge protocol adjusted according to the degree of postoperative recovery. Despite these limitations, to our best knowledge, this is the first study to evaluate the impact of general anesthetic techniques on the quality of postoperative recovery, as measured using the QoR-15K in patients undergoing minimally invasive cancer surgeries.
In conclusion, our findings indicate that propofol-based TIVA provides better early postoperative recovery at 24 and 48 h postoperatively than desflurane anesthesia. However, this transient and marginal improvement did not last until 72 h postoperatively. Additionally, this transient and slight improvement led to no significant differences in other postoperative outcomes, including quality of life, at the early discharge phase of our study. However, considering our modest sample size, further studies with sufficient power are needed to establish a standardized anesthetic technique to improve postoperative recovery.