Falls from a height commonly involve concomitant fractures of the superior rib, scapula, clavicle, or proximal humerus or shoulder luxation. Cervical spinal lesions and brain trauma also occur frequently and require neurological evaluation [1]. Considering the need for a continuous regional analgesia technique using a single catheter that covers multiple regions and given the concerns related to previously described techniques, we propose the novel sub-splenius plane (SSP) block. The SSP block is administered through catheterization of the plane between the splenius cervicis and the longissimus cervicis/capitis muscles.
Two cases of the SSP block are reported. Written informed conset was obtained from the patients. The first case is a previously healthy male patient aged 57 years who suffered a fall from a height resulting in right shoulder joint dislocation and clavicular, scapular, and rib fractures (second to sixth). The second case is a male patient aged 66 years who suffered blunt thoracic trauma after falling from a height, presenting with right rib fractures (second to fifth), an upper humerus fracture, and shoulder joint dislocation.
Both patients had a pain numeric rating scale (NPRS) score of 10/10, significant respiratory distress, dyspnea, and fatigue. A continuous novel SSP block was performed in both patients one day after the trauma. Pre-block IV analgesia for both patients consisted of 1 g paracetamol every 8 h, 400 mg/day continuous tramadol infusion, 30 mg ketorolac every 8 h, and 2 g metamizole every 12 h.
An initial bolus of ropivacaine 0.5% was administered through a 21-gauge 100-mm block needle (Contiplex, B. Braun, Germany) and, after threading the catheter 4 cm in the SSP, a continuous infusion of ropivacaine 0.375% at 5 ml/h was initiated. After the initial bolus, both patients had an NPRS score of 1/10 for each trauma region. No rescue boluses of local anesthetic (LA) were needed to maintain the NPRS score < 2.
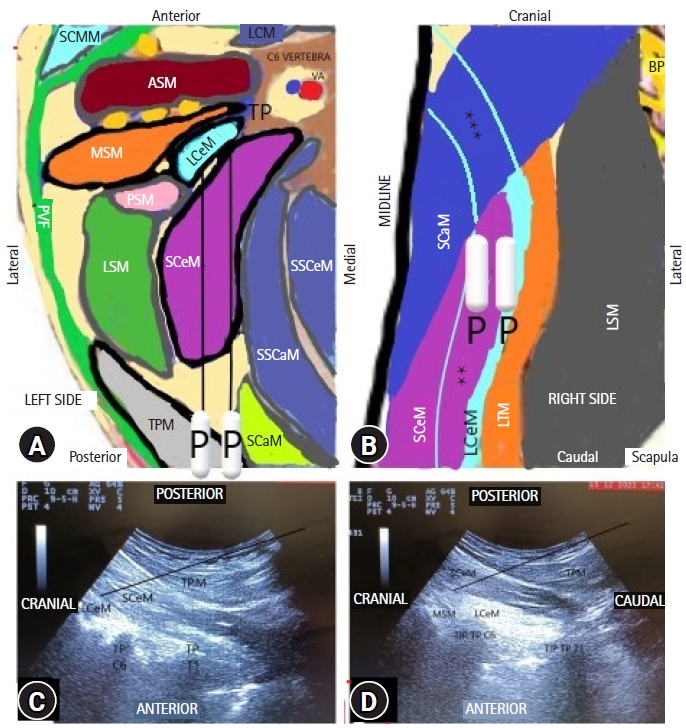
The catheters were removed 7 days after the trauma (NPRS scores increased to 3/10), and the patients were discharged 9 and 10 days after the trauma. Both patients reported a discrete reduction in thermal sensation between the T2 and T5 dermatomes in the posterior and lateral thorax and between the C5 and C8 dermatomes in the upper limb. Both patients were able to ambulate after the block and respiratory function improved significantly. This technique is described in detail in Figs. 1A-D.
The high thoracic erector spinae plane (ESP) block is effective for rib fracture analgesia and is performed at T2–T3 for painful shoulder conditions or during surgery [2–4]. With the high thoracic ESP block, the LA spreads cranially within the prevertebral compartment up to C4 and distally in the ESP, as demonstrated by magnetic resonance imaging (MRI) and cadaveric studies [2,3]. Forero et al. [2] performed an ESP block at the T2 level in a patient with chronic shoulder pain and reported effective treatment of pain, with MRI showing LA spread over the C3–C7 region. Diwan and Nair [3] also described a successful ESP block at the T2–T3 levels for shoulder surgery analgesia in five patients. Based on the results in these reports, the high thoracic ESP injectate spreads by following the orientation of the splenius cervicis and capitis muscles in the cranial/lateral oblique direction. The injectate spreads around the scalene muscles but not on the anterior surface, potentially limiting anesthesia of the phrenic nerve.
The LA spreads mostly between the levator scapulae, splenius capitis, and splenius cervicis muscles, which are located posterior to the longissimus cervicis, longissimus capitis, and cervical semispinalis muscles (Fig. 1) [2,3,5].
Based on the cadaveric study conducted by Elsharkawy et al. [5], the cervical ESP block has the potential to spread to the region of the brachial plexus, and is likely also highly phrenic sparing. This block was found to act on the dorsal rami of the cervical spinal nerves but may spread towards the neuraxial region in the context of anatomical traumatic disruption, which can complicate neurological checks and potentially produce devastating complications.
With the SSP block, the LA spreads within the prevertebral compartment, likely laterally to the transverse process, with the semispinalis capitis and cervicis and longissimus capitis and cervicis muscles located medial to the injection point as a potential anatomical barrier limiting spread towards the epidural and paravertebral space.
The anterior surface of the anterior scalene muscle is in close contact with the prevertebral fascia, only forming a virtual space for the phrenic nerve to travel and making anesthesia difficult whenever injections are performed in a distant plane [2,3].
The contrast spread of the T2 ESP block [2,3] disperses distally in the ESP and cranially mostly between the middle scalene and levator scapulae muscle (LSM) into the immediate vicinity of the neural foramina and spinal nerve roots, where the splenii muscles form the posterior barrier for the LA track. MRI studies have shown that the injectate diffuses anteriorly through the erector spinae muscle and over its surface, in the plane created by the adjacent LSM, to reach the vicinity of the cervical neural foramina and exiting nerve roots, where the LA presumably exerts its effect [2,3].
Whenever concomitant superior chest and shoulder region trauma is present, the volume of the LA used to reach the cervical region should be minimized to avoid unnecessary distal thoracic neuromuscular block (due to caudal spread), which can aggravate respiratory dysfunction. In this context, we propose the SSP block as an alternative to the high thoracic ESP block [2,3] to potentiate shoulder, thoracic, scapular, or proximal humeral analgesia through injection in the lower cervical region in the plane that is secondarily dissected by the LA with the high thoracic ESP block. Compared to the cervical ESP block, neuraxial spread of the SSP block is limited due to the lateral and posterior injection point.
The presence of the longissimus cervicis muscle beneath the splenius cervicis and splenius capitis muscles determinant because caudally, the SSP injection mimics the action of a superficial ESP block [2,3].
Further studies on the SSP block are necessary to confirm its advantages.