Introduction
Airway management of infants and neonates is challenging because of the higher difficulty of intubation and high susceptibility to hypoxemia [1]. Owing to their small size, relatively difficult airway intubation, high oxygen consumption per unit of body weight, and small functional residual capacity, these patients are associated with an increased risk of airway management with several complications [2]. Anesthesiologists encounter hypoxemia much faster in neonates and infants than adults, even during a brief period of apnea during intubation [2,3]. Moreover, multiple consecutive intubation attempts may contribute to increased morbidity [1]. Therefore, the identification of an optimal regimen for successful intubation in the minimum time for small children is of paramount importance [4].
According to a recent large-scale multicenter randomized controlled trial, the use of a videolaryngoscope improved the first-attempt success rate and reduced complications, such as hypoxemia, airway trauma, laryngospasm, and esophageal intubation, in infants weighing Ōēż 6.5 kg [5]. The C-MAC┬« (Karl Storz, Germany) is a widely used videolaryngoscope with standard Miller blade sizes #0 and #1, suitable for use in neonates and infants [5ŌĆō7]. Compared to the McGrathTM MAC size #1 blade and direct laryngoscopy, the C-MAC┬« Miller blade provides superior-quality glottis view in neonates and infants [7].
Despite the improved laryngeal view, endotracheal tube (ETT) delivery to the laryngeal inlet and ETT passage into the glottis remain challenging in infants and neonates as the ETT tip gets lodged against the anterior tracheal wall because of the anatomical features of an angled vocal cord, relatively small oropharynx, and large tongue [1,8]. Furthermore, even a small motion generated by the operator makes the ETT move significantly in the glottis view of the device. Therefore, optimizing the ETT shape to facilitate operator handling constitutes an important factor for successful tracheal intubation over a short time [4,8]. In adult patients, a 90┬░-angled hockey-stick-shaped stylet could facilitate successful intubation using a videolaryngoscope. McElwain et al. [9] demonstrated that a hockey-stick stylet configuration significantly reduces intubation time compared to other stylet shapes, including a C-curved shape, when using a C-MAC videolaryngoscope with a standard MAC blade. Nevertheless, there has been limited data regarding the ideal ETT stylet shape for neonates and infants [8].
Considering the limited size of the oropharyngeal cavity in neonates and infants, we assumed that a C-curve-shaped stylet resembling the natural ETT curve could facilitate ETT handling than a hockey-stick-shaped stylet. Therefore, this prospective randomized controlled study was conducted to compare the time to target till delivery of the ETT tip to the glottis with the C-curve-shaped and conventional hockey stick-shaped stylet using a C-MAC® video laryngoscope in neonates and infants.
Materials and Methods
Study population
This prospective randomized controlled study was approved by the institutional research ethics committee of Seoul National University Hospital (No. H2011-196-1178), registered at http://clinicaltrial.gov (No. NCT04745936, principal investigator: L.J.H., date of registration: February 4, 2021) before patient enrollment, and performed at our institution between March 2021 and April 2022. The study protocol was thoroughly explained to the parents, and written informed consent was obtained from the parents of all patients prior to the surgery. This study was performed in accordance with the tenets elucidated in the Declaration of Helsinki (2013) and its amendments.
Children less than 12 months scheduled for elective surgery requiring endotracheal intubation under general anesthesia at a single tertiary referral center were enrolled. Patients with upper respiratory tract infection symptoms, abnormal airways, or severe uncompensated cardiopulmonary diseases as well as those classified as the American Society of Anesthesiologists grade IV and V were excluded from this study.
Randomization and ETT preparation
Patients were randomly assigned to either the hockey stick-curved stylet group (group H) or the C-curved stylet group (group C). For randomization, an online response system (http://www.randomizer.org) was used with a 1 : 1 allocation ratio. Sequentially numbered opaque sealed envelopes were prepared by a researcher not involved in this study to conceal group allocation. The operator identified the allocated group by opening the envelope immediately before induction.
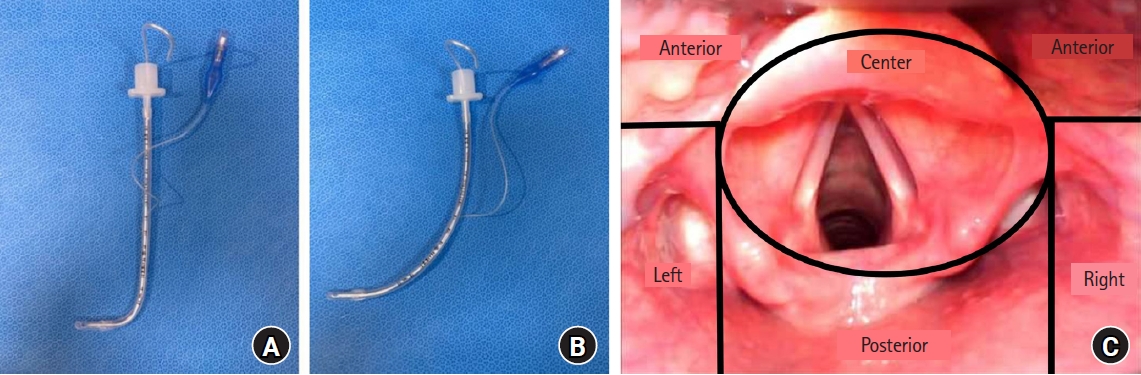
All patients were intubated with a cuffed ETT, in accordance with the institutional standard of care. Tube size was determined as described by Salgo et al. [10]. ETT curvature (ShileyTM, Hi-Contour Oral/Nasal Tracheal Tube, Covidien, Germany) was prepared according to its designated group by using Flexible Stylet (2 mm PORTEX┬« stylet; Smiths Medical International Ltd., UK). In the hockey stick-curved stylet group (group H), the configuration of the distal tube tip was angled to resemble a ŌĆśhockey stickŌĆÖ; its shaft remained straight as in the manufactured state (Fig. 1A). In the C-curved stylet group (group C), the distal tube tip was angled in a large C-shape to maintain the original tube curvature (Fig. 1B). We prepared ETT templates for both the hockey stick-curved and C-curved ETTs to maintain the consistency of the ETT angle throughout the study.
Anesthesia and outcome variables
Routine monitoring was initiated immediately after the patient was admitted to the operating room. After pre-oxygenation, atropine (0.2 mg/kg) and thiopental sodium (5ŌĆō6 mg/kg) were administered intravenously. Rocuronium bromide (0.6ŌĆō1.2 mg/kg) was used for neuromuscular blockade. Facial mask ventilation was performed with sevoflurane and 100% oxygen. After disappearance of the single twitch response, the patients were intubated using a C-MAC┬« videolaryngoscope with a Miller blade size #0 or #1 and a predetermined ETT with a loaded stylet. While maintaining the patientŌĆÖs head in the neutral position, the operator inserted the tube after securing the best glottic view through a C-MAC┬« videolaryngoscope. All intubation attempts were performed by anesthesiology residents with experience of Ōēź 30 direct laryngoscopies in infants and neonates. To reduce errors when measuring the recordings, all procedures from insertion to videolaryngoscope withdrawal were video-recorded.
When the patientŌĆÖs oxygen saturation decreased to less than 95%, the intubation procedure was suspended, and manual ventilation with 100% oxygen was initiated to restore oxygen saturation to 98%ŌĆō100% before any further intubation attempt. Each intubation attempt included from ETT insertion into the patientŌĆÖs oropharynx till its withdrawal from the oral cavity. When the operators failed to advance the ETT through the glottis during the first attempt, they were allowed to either change the stylet curvature or maintain the original stylet curvature. However, when the stylet curvature changed or after more than two attempts, such cases were defined as failed intubations.
A single investigator blinded to group allocation reviewed the videos and collected the data for analysis. We divided the total intubation time into three epochs: (1) time to glottis visualization after C-MAC┬« videolaryngoscope insertion (T0), (2) time to approach the ETT tip to the glottis after glottis visualization (T1), and (3) time to advance the ETT cuff fully through the glottis after inserting the ETT tip into the glottis (T2). The time required for each step was recorded. The primary outcome was tube handling time (T1 + T2). The secondary outcomes included the total intubation time (T0 + T1 + T2), T1 and T2, the initial location of the ETT tip on the monitor of the C-MAC┬« videolaryngoscope, the modified Cormack and Lehane grade, the incidence of successful intubation in the first attempt within 30 s, the number of intubation attempts, and the need for any optimization techniques such as external laryngeal manipulation, head extension, or stylet curvature change. The operators rated subjective intubation difficulty on a 10-point numerical rating scale (0 = extremely easy, 10 = extremely difficult) [11]. The initial ETT tip location at the laryngeal inlet and the locational changes of the tip after redirection were recorded regardless of its position in the center. The space around the laryngeal inlet on the monitor of the videolaryngoscope was divided and named, as shown in Fig. 1C. The ŌĆścenterŌĆÖ was defined as the space along the upper border of the epiglottis to the lower border of the cuneiform cartilage and corniculate cartilage. The upper part of the epiglottis was defined as the ŌĆśanteriorŌĆÖ region and the lower part of the center and anterior space were divided into three divisions. The ŌĆśposteriorŌĆÖ region was defined as the division just below the center and ŌĆśLeftŌĆÖ and ŌĆśRightŌĆÖ as the division located on either side of the posterior division. All positional changes in the ETT tip were recorded before intubation. Information on patient characteristics, such as age, sex, height, and weight, and type of surgery were collected from the patientsŌĆÖ electronic medical records.
Statistical analysis
The sample size was calculated based on a previous study comparing two stylet curvatures during intubation using a videolaryngoscope in infants [12]. Accordingly, the tube insertion time was significantly higher in the hockey stick-curved stylet group than in the spiral-shaped stylet group (18.2 ┬▒ 5.3 s vs. 15.4 ┬▒ 4.7 s, P = 0.012). Using these values as reference, 52 patients per group were required to detect a difference of 2.8 s in the tube insertion time between groups using a two-sided StudentŌĆÖs t-test with an ╬▒ error of 0.05 and a power of 80%. Considering a dropout rate of 10%, the minimum participant number was calculated as 114 patients (57 patients per group).
Normality was assessed using the ShapiroŌĆōWilk W-test. Data are expressed as the mean and standard deviation or median and interquartile range for parametric variables, and as frequencies/percentages for nonparametric variables. Categorical variables were compared using PearsonŌĆÖs chi-square test and FischerŌĆÖs exact test when more than 20% of the cells had expected frequencies of less than five. Continuous data were compared using StudentŌĆÖs t-test or MannŌĆōWhitney rank-sum test. Statistical analyzes were performed using the SPSS (ver. 23.0; IBM Inc., USA). Statistical significance was set at P < 0.05.
Results
A total of 114 participants were enrolled in the present study and four were excluded after enrollment due to changes in their surgical plans that did not necessitate endotracheal intubation. Therefore, the data of 53 children in group H and 57 children in group C were analyzed (Fig. 2). Baseline patient characteristics are shown in Table 1. Patient characteristics, including age, height, weight, sex, and type of surgery, were comparable between the two groups.
Table 2 shows the data on the intubation process between the two groups. The tube handling time after glottis visualization (T1 + T2) was significantly shorter in group C than in group H (13.3 ┬▒ 8.9 s vs. 25.1 ┬▒ 27.0 s, respectively; mean difference [MD]: ŌłÆ11.8 s, 95% CI [ŌłÆ19.3, ŌłÆ4.3], P = 0.002). Although the time to glottis visualization (T0) was comparable between groups, the total intubation time (T0 + T1 + T2) in group C (19.9 ┬▒ 9.4 s) was significantly shorter than that in group H (32.8 ┬▒ 27.1 s, MD: ŌłÆ13.0 s, 95% CI [ŌłÆ20.5, ŌłÆ5.4], P = 0.001). However, there was no difference in the distribution of operatorsŌĆÖ residency years between the two groups. As the modified Cormack and Lehane grade was Ōēż 2a in all patients, no additional maneuvers to improve the glottis views, such as the use of cricoid pressure or laryngeal manipulation, were performed.
Tracheal intubation was successful in all patients in group C after a single attempt. However, more than two intubation attempts were required for six patients (11.3%) in group H; in five of them the ETT curvature changed to a C curve for successful tracheal intubation. In group C, 87.7% of patients were intubated within 30 s whereas in group H, 69.8% of patients were intubated within 30 s (MD: 18.7%, 95% CI [2.4, 34.5], P = 0.029).
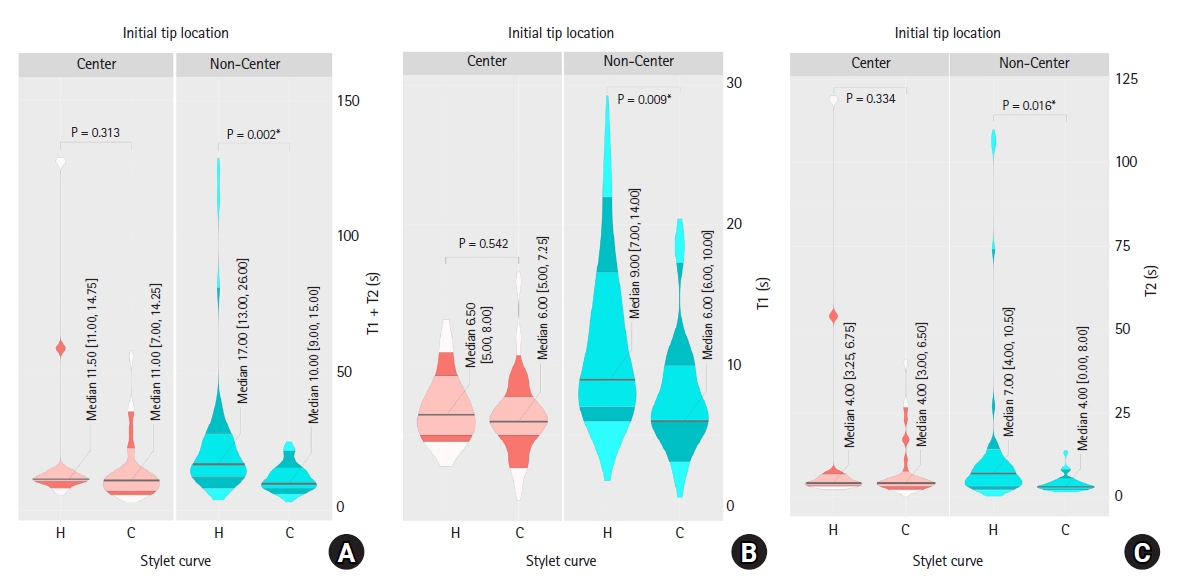
The initial tube tip location on the videolaryngoscope monitor was at the center in 34 children in group C (59.6%) and 12 children in group H (26.1%; MD: 33.5%, 95% CI [13.9, 50.4], P < 0.001). If the initial tip location was placed in the center, the tube handling time (T1 + T2) did not significantly differ between the groups (median [Q1, Q3]); 11.00 s (7.00, 14.25) vs. 11.50 s (11.00, 14.75); effect size: 0.40, 95% CI [ŌłÆ32.5, 12.0], P = 0.334) (Fig. 3). In addition, both the time required to approach the ETT tip to the glottis (T1) and that required for tube advancement (T2) showed no statistical intergroup difference (P = 0.542 and P = 0.334, respectively). However, in patients in whom the tube tip was not initially centered at the laryngeal inlet, the T1 + T2 was significantly shorter in group C (4.0 ┬▒ 2.6 s vs. 13.6 ┬▒ 24.2 s; MD: ŌłÆ9.61 s, 95% CI [ŌłÆ17.314, ŌłÆ1.905], P = 0.016). Furthermore, the patients in group H required more time to approach (T1) and advance the ETT into the vocal cords (T2) (P = 0.009 and P = 0.016, respectively).
Operators rated intubation as easier when using a C-curved ETT (Table 2). Hypoxemia (SpO2 < 90%) occurred in two patients in group H whereas none of the patients in group C experienced desaturation.
Discussion
In this prospective randomized controlled study, the use of a C-curved ETT significantly decreased the time to target and deliver the tip of the ETT to the glottis compared with the hockey stick-shaped ETT for intubation with the C-MAC® Miller videolaryngoscope in infants and neonates. In addition, the C-shaped stylet facilitated ETT placement in the center, thereby shortening the tracheal intubation time.
Considering the small-sized airways, small functional residual capacity, increased oxygen consumption, and technical issues, airway management in neonates and infants is challenging [1,13]. Furthermore, several anatomical features of the pediatric airway such as the large tongue relative to the mandible and mouth size, long floppy, omega-shaped epiglottis, cephalad larynx, and anterior vocal cords make ETT manipulation in infants and neonates more difficult [13,14]. Therefore, it is essential to devise a method to quickly and accurately perform endotracheal intubation in infants and neonates on the first attempt.
According to previous studies, the C-MAC® videolaryngoscope using a Miller blade is useful in providing an improved glottic view in pediatric patients [6,15,16]. In the present study, no patients were classified as Cormack-Lehane grade III or IV with the C-MAC® videolaryngoscope with Miller blade. Furthermore, the time to glottis visualization was significantly shortened in neonates undergoing intubation with the C-MAC videolaryngoscope (7.7 ± 0.1 s) compared to the Miller direct laryngoscope (11.3 ± 0.1 s) according to a recent pediatric study [17]. However, improved glottis visualization does not guarantee easy intubation. According to a recent large-scale multicenter study performed in infants, despite the high success rate of first-attempt intubation using a C-MAC videolaryngoscope, it did not guarantee a 100% success rate [5]. Therefore, videolaryngoscope devices usually require intubation adjuncts such as a stylet or a bougie to make the ETT shape more feasible for easy targeting and advancement through the glottis [8]. Furthermore, a dynamic interplay of hand-eye coordination and visuospatial coordination is required for the successful manipulation of the ETT under indirect observation through a videolaryngoscope [17]. To overcome the technical difficulty and guarantee the successful intubation, identifying the optimal shape of the ETT is essential [1,4,12].
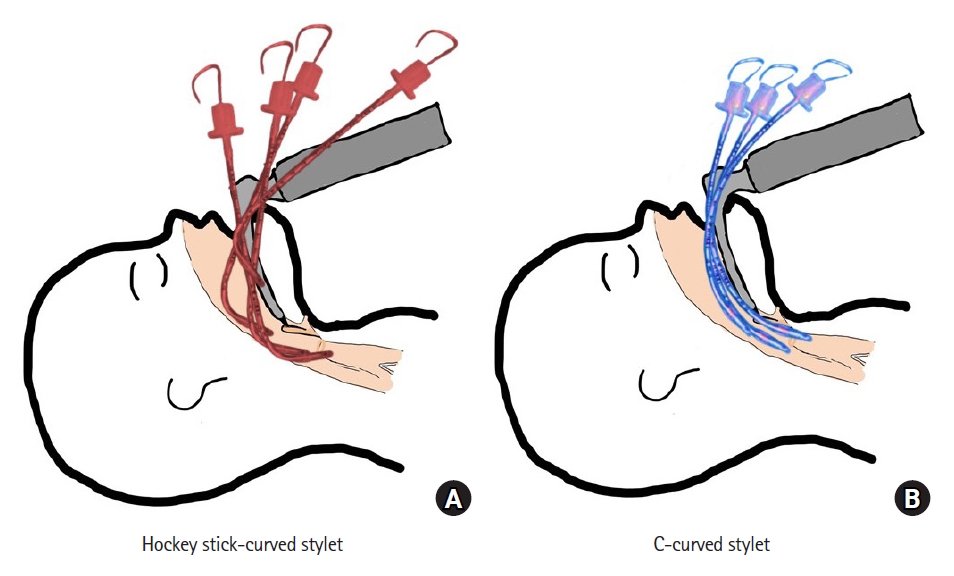
In this study, the use of the C-curved ETT resulted in a significant reduction in tube handling time after glottis visualization to 11.8 s and in the time required for tube advancement by 3.5 s, compared to the hockey stick-shaped ETT. In addition, the total intubation time was 19 s in group C, 8 s less than the time reported by Gupta et al. [7] that compared the C-MAC Miller blade and the McGrath MAC blade. Furthermore, during neonatal resuscitation, the safety window for intubation attempts is limited to 30 s [18,19]. Saving 11 s in an intubation trial may be a crucial factor in determining patient prognosis considering the rapid desaturation during apnea in neonates and infants. We speculated that the acute ETT angle in group H might prevent smooth ETT advancement, facing multiple obstacles within the narrow oropharyngeal cavity. Moreover, this required more additional manipulation while targeting the ETT to the glottis, when compared to a C-curved ETT (Fig. 4).
Positioning the ETT tip in the center of the videolaryngoscope screen facilitates tracheal intubation and helps reduce intubation time [12]. If the ETT tip points in an undesirable direction, additional handling for directing the ETT tip to the glottis is required. Owing to the structural differences in infantsŌĆÖ airways, the range of motion in the videolaryngoscope screen is relatively large, even with a small ETT movement, making its manipulation difficult. In this study, when the initial ETT tip position was placed at the center of the glottis, the median time for tube handling during tracheal intubation was similar between groups C (11 s) and H (11.5 s). However, this only occurred in approximately 26% of patients in group HŌĆöa significantly lower incidence than in group C.
Additionally, the use of the C-curved stylet demonstrated a higher first-attempt success rate (100% vs. 88.7%) and a higher successful intubation rate within 30 s (87.7% vs. 69.8%) than the hockey stick-shaped stylet group when performed by less-experienced clinicians. Five patients in the hockey stick group were successfully intubated after curvature change in the second tracheal intubation attempt. The reported success rate in the first attempt using the C-MAC video laryngoscope Miller blade in neonates and infants was 93%ŌĆō95.7% [5,7], but there was no information regarding stylet shape. Considering our first-attempt success rate, we concluded that C-curved ETT preparation helps improve intubation safety in infants and neonates.
Our study has several limitations. First, the operators were not blinded to stylet allocation during intubation. However, an investigator blinded to group allocation reviewed the records and analyzed the video data. As the length of the ETT visible through the screen until the tube tip reaches the glottis was too short to identify the ETT shape, we assumed that the investigator was blinded to group allocation based on recorded videos. Additionally, operators were provided with a preformed tube immediately before intubation to reduce bias. Second, we did not count the number of advancement maneuvers, such as withdrawing the ETT [5] or reverse ETT loading [4] to improve advancement through the vocal cords. However, we speculated that adding these maneuvers would be associated with increased time for successful completion of intubation, which was the main outcome of this study. Third, we did not control the operatorsŌĆÖ previous experience in videolaryngoscopy but we considered that this might be reflected in operatorsŌĆÖ grades; we found no difference in distribution of operatorsŌĆÖ grades between groups. In addition, the number of operatorsŌĆÖ participation in the study was not restricted. A total of 27 operators participated in the study, and the median value of participation of each operator was 2 (interquartile ranges 2ŌĆō6), assigned more than once to each group and less than 5 times in each group. Finally, infants suspected to have a difficult or abnormal airway were excluded from the study. Further research should focus on the effect of different ETT shapes on successful intubation using various videolaryngoscopes in children with difficult airways.
In conclusion, the use of a C-curved stylet could reduce tube handling time and total intubation time compared with a hockey stick-shaped stylet using a C-MAC® videolaryngoscope in neonates and infants. Moreover, it improved the rate of successful intubation within 30 s and the positioning of the initial ETT tip to the center of the laryngeal inlet. Further research is needed to evaluate the effect of different stylet shapes on the intubation success rate using various videolaryngoscopes for difficult airway management in children.