Introduction
Interscalene brachial plexus block (ISBPB) has been widely used for surgical anesthesia in patients undergoing arthroscopic shoulder surgery [1,2]. However, ISBPB is not without side effects. Local anesthetic placed into the interscalene groove spills out of the groove and spreads along the prevertebral fascia toward the ipsilateral stellate ganglion [3]. Local anesthetic-induced stellate ganglion block (SGB) inhibits the oculosympathetic pathway, resulting in miosis of the ipsilateral pupil (Horner’s syndrome). Given that the stellate ganglion synapses with cardiac sympathetic postganglionic fibers [4], SGB also reduces cardiac sympathetic nervous activity (CSNA). Therefore, SGB has been used as one of the methods for cardiac sympathetic denervation to treat medically refractory arrhythmias driven by enhanced CSNA, such as refractory ventricular arrhythmia, long QT syndrome, and inappropriate sinus tachycardia [5–7]. Usually, arthroscopic shoulder surgery is performed with patients seated because the sitting position provides excellent intra-articular visualization, reduces intraoperative blood loss, decreases the incidence of traction neuropathy, and facilitates the conversion to an open procedure [8]. However, after a right SGB, the CSNA does not increase with positional changes from supine to sitting [9] or during head-up tilt [10], unlike normal physiologic conditions where a transition to sitting enhances sympathetic nervous activity (SNA) [9] to compensate for a reduction in the venous return to the heart [11]. Occasionally, a right SGB leads to cardiac arrest during a head-up tilt test [12]. Therefore, the measurement of CSNA is important after the transition to the sitting position when patients present with Horner’s syndrome after ISBPB. However, measurement of CSNA using conventional methods is impractical in intraoperative settings [13]. Alternatively, heart rate variability (HRV) is feasible to measure the autonomic nervous activity confined to the heart. Despite the unreliability of the low-frequency power (LF) of HRV, which is reported to represent cardiac autonomic outflow by baroreflexes rather than CSNA [14] and is significantly affected by heart rate [15], LF performs well to reflect changes in CSNA in response to a postural change maneuver or head-up tilt test, which consistently increases SNA [16,17]. Hence, LF is assumed to reliably represent CSNA in seated patients receiving arthroscopic shoulder surgery under ISBPB, similar to subjects undergoing a postural change maneuver or head-up tilt test, because they share the same physiological conditions (reduced venous return to the heart). However, the accurate calculation of LF requires a 4-minute-long electrocardiogram (ECG) waveform [18], so it cannot provide instantaneous information about CSNA. In addition, an ECG waveform is prone to artifacts from movement or electrocauterization, which require manual processing to remove, thereby preventing the automatic calculation of HRV parameters.
Pupil size is controlled by the interplay of the iris sphincter and dilator muscles, which are innervated by the parasympathetic and sympathetic nervous systems, respectively. Therefore, pupillometry is useful to evaluate autonomic nervous activity. Recently, owing to its easy applicability and low cost, pupillometry has been proposed as an alternative method for the assessment of cardiac autonomic nervous activity [19,20] after a significant correlation was found between pupil size and LF at rest in healthy subjects [21,22], during exercise in athletes [20], and during exercise in patients undergoing hemodialysis [19]. In particular, the measurement of pupil size would be useful to assess CSNA in patients receiving SGB to treat atrial fibrillation that prevents the analysis of HRV [23].
However, the relationship between the changes in pupil size and CSNA has not been investigated after transitioning to the sitting position under the influence of ISBPB-induced SGB. Therefore, the usefulness of pupillometry remains unclear for seated patients with ISBPB-induced SGB. In this study, we measured the pupil size and autonomic nervous activity (HRV parameters) of patients in the seated position after ISBPB to test the hypothesis that changes in pupil size are correlated with changes in CSNA before ISBPB and after the transition to sitting following ISBPB.
Materials and Methods
The protocol of this observational study was approved by the Institutional Review Board of Daegu Catholic University Medical Center (IRB no. CR-18-052). Written informed consent was obtained from all patients during their preoperative visits to the outpatient department. The study followed the Good Clinical Practice guidelines and the principles of the Declaration of Helsinki (2013).
We enrolled patients aged 20–60 years with an American Society of Anesthesiologists physical status of 1 who were scheduled to undergo right arthroscopic shoulder surgery under ISBPB. The exclusion criteria were coagulopathy, infection at the ISBPB site, peripheral neuropathy or neurologic sequelae on the operative limb, allergy to local anesthetics or history of allergic shock, contralateral vocal cord palsy, contralateral hemidiaphragmatic paresis or paralysis, contralateral pneumothorax or hemothorax, physiologic anisocoria (a difference in the pupil diameter between both eyes of more than 0.5 mm), severe ptosis precluding measurement of the pupil diameter, arrhythmias, conduction abnormalities on ECG, use of medications that affect cardiac conduction, ischemic heart disease, hypertension, diabetes mellitus, thyroid dysfunction, electrolyte imbalance, psychiatric diseases, and difficulty communicating with the medical personnel.
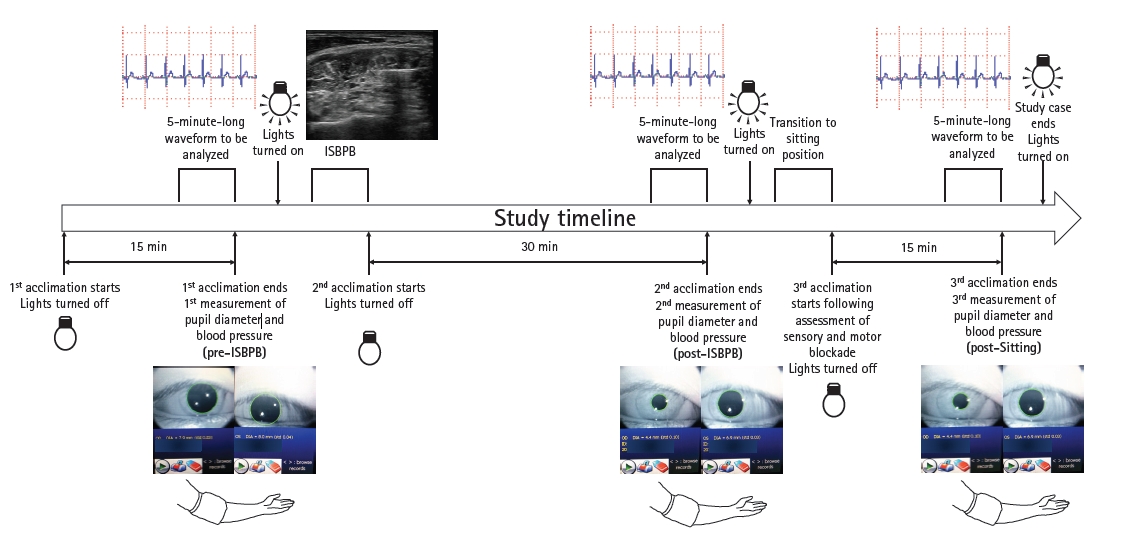
The patients abstained from alcohol and caffeine-containing products for at least 24 h before surgery. No premedication was administered to the patients. On arrival to the operating room, the patients were placed in a supine position on the operating table. A pulse oximeter sensor (TruSignalTM SpO2 Finger Sensor, TS-F-D, GE Healthcare Finland Oy, Finland) and a noninvasive blood pressure cuff were placed over the right index finger and on the left arm, respectively. Three ECG electrodes were placed on both the infraclavicular fossae and left anterior axillary line midway between the costal margin and the iliac crest. Once the ECG and photoplethysmographic (PPG) waveforms were displayed without artifacts on a patient monitor (CARESCPETM Monitor B650, GE Healthcare Finland Oy, Finland), all the lights in the operating room were turned off, the patient monitor was turned away from the patient, and acclimation commenced under quiet conditions at ambient temperature to stabilize the patients’ hemodynamics and autonomic nervous activity. In the low mesopic conditions, the patients were instructed not to talk, to remain as still as possible, and to breathe regularly without taking deep breaths. After 15 min of the acclimation period (pre-ISBPB), the pupil diameter was measured in the left eye and then in the right eye. Subsequently, the systolic, diastolic, and mean arterial blood pressures were measured. The measurements were followed by administration of the ISBPB with the lights on. The patients remained still in the supine position with the lights off for 30 min after the ISBPB. The pupil size and arterial blood pressure were measured (post-ISBPB), and then the lights were turned on. The patients were placed in the seated position with the back elevated to 70°–80°; the hips and knees flexed to 30° and 120°, respectively; and the knees rested on a pillow. Following evaluation of the sensory and motor blockade, the patients remained still in the seated position with the lights off for 15 min. The study session ended after the third measurement of the pupil diameter and the blood pressure were taken (post-sitting). The study timeline is illustrated in Fig. 1. All the study cases began and finished between 9:00 am and 12:00 pm. The anesthesiologist who performed the ISBPB was not involved in (and was blinded to) the data collection and analysis. One of the authors extracted and analyzed the PPG waveforms for the last 5 min before each of the first two measurements of the pupil diameter (pre-ISBPB and post-ISBPB) and analyzed the ECG waveforms for the last 5 min before each of the three measurements (pre-ISBPB, post-ISBPB, and post-sitting). Another author measured the pupil diameter, blood pressure, and degree of sensory and motor blockade. Both authors were blinded to each other’s data.
At the end of the experiment, the patient was prepared for surgery, and the surgery proceeded with the patient seated. Intraoperatively, ECG and pulse oximetry were monitored continuously. The patient’s arterial blood pressure was monitored using a noninvasive blood pressure cuff at 5-min intervals. However, the blood pressure could be measured at any time within the 5-min interval at the discretion of the attending anesthesiologist, who was not involved in the study.
For the placement of ISBPB, a 5- to 13-MHz linear phased array transducer (UST-5413, Hitachi Aloka Medical, Ltd., Japan) equipped in an ultrasound machine (ProsoundTM α6, Hitachi Aloka Medical, Ltd., Japan) was used to visualize the 5th, 6th, and 7th cervical nerve roots (C5, C6, and C7 nerve roots) [2]. A 50-mm, 22-gauge block needle (SonoPlex STIM, Pajunk® GmbH, Germany) was introduced lateral to the transducer using an in-plane technique and was advanced in a lateromedial direction. Each nerve root and the supraclavicular nerve located between the middle scalene muscle and the posterior border of the sternocleidomastoid muscle [24] were blocked with 25–30 ml of 0.75% ropivacaine.
Following the adaptation to low mesopic conditions [25], the patients were instructed to keep their head and eyes facing forward and their eyes wide open without blinking during the targeting and measurements. The eyecup of an automated monocular infrared pupillometer (VIPTM-200 pupillometer, NeurOptics Inc., USA) was placed around the eye being tested and parallel to the axis of vision. The tilt of the instrument was minimized to ensure the best alignment (right angle) between the instrument and the axis of vision. The pupil diameter was measured at 30 Hz for 2 s. Its average and standard deviation were calculated from the 60 measurement data (Supplementary Fig. 1) [1]. If the standard deviation was more than 0.1 mm, the measured value was discarded, and a new measurement was performed. The pupil diameter contralateral to the ISBPB was measured first, and then the ipsilateral diameter was measured.
Between the beginning and end of vital sign monitoring, the ECG and PPG waveforms were continuously recorded at a sampling rate of 300 Hz using S5 collect software (GE Healthcare Finland Oy, Finland) installed in a laptop computer connected to a patient monitor via a UPI-PI Serial Cable (GE Healthcare Finland Oy, Finland). The pulse oximeter sensor was placed on the index finger ipsilateral to the ISBPB before the patients had transitioned from the supine to seated position; afterward, the sensor was placed on the contralateral index finger.
Five-minute-long ECG waveforms for each study time point were loaded onto the WinDaq Waveform Browser (DATAQ Instruments, USA). The R peaks of the ECG signal were automatically detected using Advanced CODAS analysis software (DATAQ Instruments). Undetected or erroneously detected peaks were identified by manual inspection and then manually replaced with new correct peaks or discarded.
The beat-to-beat RR intervals were calculated using Advanced CODAS analysis software. The RR intervals from ectopic beats were defined as those 20% shorter or longer than the previous interval. They were replaced with adjacent normal RR intervals. ECG waveform segments with more than three ectopic beats were excluded from the final analysis. In a tachogram, the abscissa and ordinate represent the time in seconds and RR interval in milliseconds, respectively. Each data point was linearly interpolated, and then new discrete-time equidistant data were generated by resampling at 4 Hz from the interpolated line. By creating a residual plot from the simple linear regression model built with time (independent variable) and corresponding RR interval (dependent variable) resampled at 4 Hz, the tachogram was detrended. The 300-second-long detrended data were split into five segments of 100 s in length with two adjacent segments overlapping by 50% (50 s). Each segment was Hamming windowed [26] and submitted to fast Fourier transform to generate five periodograms. The values of the spectral power corresponding to each frequency from the five periodograms were averaged (Welch method of power spectral density estimation) [27]. The frequency resolution was 0.01 Hz, and the highest frequency of the power spectrum was 2 Hz (Nyquist frequency).
The areas from 0.04 to 0.15 Hz, from 0.15 to 0.4 Hz, and from 0 to 0.4 Hz were integrated to obtain the LF, high-frequency power (HF), and total power of HRV, which represent the combined sympathetic and parasympathetic modulation of the heart rate via baroreceptor reflexes, parasympathetic modulation of heart rate in response to spontaneous respiration, and the overall activity of the autonomic nervous system [28]. Because LF is mainly modulated by SNA [16,17], the LF to HF ratio (LF/HF) represents the sympathovagal balance [28]. Its increase indicates a shift in the sympathovagal balance toward sympathetic predominance, and vice versa. The power spectral density was calculated using the advanced DSP module of DADiSP software version 6.7 (DSP Development Corp., USA). The LF, HF, and total power were natural-log-transformed due to their skewed distribution. Descriptions of the spectrogram, time domain and nonlinear HRV parameters, and sample and approximate entropy are provided in the Supplementary Material 1.
As with the analysis of ECG waveforms, the systolic peaks of the PPG signal were detected using Advanced CODAS analysis software (DATAQ instrument) in the 5-minute-long PPG waveforms for each study time point, which were loaded onto the WinDaq Waveform Browser (DATAQ Instruments). The missing or spurious peaks detected under visual inspection were replaced with new ones or deleted, respectively.
Pulse wave transit time was defined as the time interval between an R peak of the ECG signal and the foot of the PPG wave corresponding to the R peak (the maximum of the second derivative of the PPG wave) [29]. Erroneously detected or undetected maximum peaks of the second derivative were manually deleted or added, respectively. The surgical pleth index (SPI) displayed on the patient monitor was also recorded [30].
A hypotensive bradycardic event (HBE) was determined to occur 1) if the heart rate decreased by more than 30 beats/min from the pre-ISBPB rate within a 5-min interval or decreased to less than 50 beats/min at any time and/or 2) if the systolic blood pressure decreased by more than 30 mmHg from the pre-ISBPB blood pressure within the 5-min interval or decreased to less than 90 mmHg at any time. However, the presence of signs and symptoms of an HBE (lightheadedness, nausea, vomiting, and cold sweats) were not mandatory for its diagnosis [31]. HBEs were managed with 5–10 mg of ephedrine, the administration of which could be repeated up to three times.
Because the purpose of this study was to assess the usefulness of pupillometry to predict the changes in CSNA following ISBPB, the primary endpoint was the change in pupil diameter from the baseline (pre-ISBPB) to the sitting position (post-sitting), which were adjusted for the baseline difference between the bilateral eyes ([right pupil diameter for post-sitting – left pupil diameter for post-sitting] – [right pupil diameter for pre-ISBPB – left pupil diameter for pre-ISBPB]). The secondary outcome variables were the changes in CSNA from pre-ISBPB to post-sitting (natural-log-transformed LF [lnLF] for post-sitting – lnLF for pre-ISBPB); the right and left pupil diameters; the HRV parameters from the frequency domain, the time domain, and nonlinear analyses; the arterial blood pressure at the three time points; the PPG parameters at the first two time points; the incidence of HBE; and the incidence of Horner’s syndrome, which was diagnosed if the adjusted pupil diameter was less than –0.5 mm [32].
Sample size calculation
According to the results of the pilot study using 10 patients, the standard deviation of the changes in pupil diameter adjusted for the baseline differences was 0.4 mm. The regression coefficient and coefficient of determination (R2) of the linear regression model between the changes in pupil diameter (independent variable) and the changes in lnLF (dependent variable) were 0.5 and 0.21, respectively. A sample size of 42 was required to achieve 90% statistical power at a two-sided significance level of 0.05 for the detection of a change in the regression coefficient from 0 under the null hypothesis to 0.5 under the alternative hypothesis when the coefficient of determination and standard deviation of the independent variable were 0.21 and 0.4 mm, respectively. Considering a drop-out rate of 10%, a total of 48 patients were required in this study. The sample size was calculated using PASS 15 Power Analysis and Sample Size Software (2017) (NCSS, LLC, USA, ncss.com/software/pass).
Statistical analysis
The normality assumption was tested using the Shapiro–Wilk test. Normally and nonnormally distributed data are presented as the mean ± SD and median (Q1, Q3), respectively. Categorical data are presented as the number of patients (percentage). A simple linear regression analysis was performed to investigate the linear relationship between the changes in pupil diameter and the changes in lnLF from baseline to when the patient was in the sitting position. We used a linear mixed-effects model to assess the fixed effects of the side of an eye, three time points, and the interaction between them on the pupil diameter, taking into account the random effects of each subject. The longitudinal changes in the difference in the pupil diameters between bilateral eyes, the HRV parameters, and the arterial blood pressure during the three time points were analyzed using a repeated-measures analysis of variance (for normally distributed data) or Friedman’s test (for nonnormally distributed data), with paired t test or Dunn’s test used for the post hoc pairwise multiple comparisons, respectively. To compensate for an α error inflation resulting from multiple pairwise comparisons, the probability values were adjusted using the Bonferroni correction. The changes in the PPG parameters during the first two time points were assessed by a paired t test. A two-sided probability value < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows (Version 20.0.0, IBM Corp., USA).
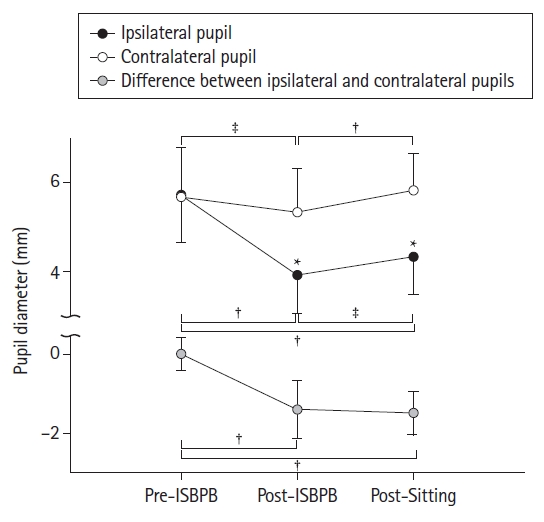
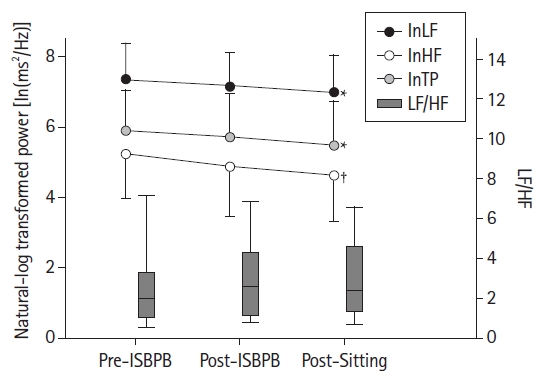
Results
Out of 48 recruited patients, six patients were excluded from the analysis due to the development of arrhythmia despite a normal preoperative ECG (n = 1); the presence of severe preoperative ptosis in both eyes, which precluded appropriate measurement of the pupil diameter (n = 1); intolerance to the nearly upright seated position (n = 1); the inability to visualize the C7 nerve root under ultrasound guidance (n = 1); protocol violation (n = 1); and an intolerance to the subjective dyspnea caused by ipsilateral diaphragmatic paralysis, leading to conversion to general anesthesia (n = 1). Table 1 shows the characteristics of the 42 patients whose data were analyzed. Out of the 42 patients, 41 (97.6%) developed Horner’s syndrome. The ipsilateral (right) pupil diameter was significantly decreased; the absolute difference in the pupil diameter between ipsilateral (right) and contralateral (left) eyes was significantly increased post-ISBPB and post-sitting compared to pre-ISBPB (Fig. 2). The lnLF, natural-log-transformed HF (lnHF), and natural-log-transformed total power (lnTP) were significantly reduced from baseline (pre-ISBPB) to the sitting position (post-sitting), while the LF/HF did not change over the three time points (Fig. 3). However, no significant changes in HRV parameters were observed between pre-ISBPB and post-ISBPB or between post-ISBPB and post-sitting. A positive linear relationship was found between the adjusted changes in the pupil diameter and the changes in lnLF from pre-ISBPB to post-sitting (Fig. 4). A one-unit decrease (1 mm) in the change in pupil diameter contributed to a 0.659 ln(ms2/Hz) decrease in the change in lnLF (95% CI [0.090, 1.228], R2 = 0.242, P = 0.001).
From pre-ISBPB to post-sitting, there were significant reductions in 1) the proportion of the number of interval differences of successive RR intervals greater than 50 msec in the total number of RR intervals (pNN50); 2) standard deviation of the successive differences of the RR intervals (SDSD); 3) root mean square of the successive differences of the RR intervals (rMSSD); 4) difference between the first and the third quartiles of the successive differences in the RR intervals (IRRR); 5) median of the absolute values of the successive differences in the RR intervals (MADRR); 6) the baseline width of the triangular interpolation of the NN (RR) interval histogram (TINN); 7) ratio of total number of RR intervals to the number of RR intervals in a 7.8125 msec-long bin with the most RR intervals (HRV index); and 8) standard deviation of the points perpendicular to the line of identity in the Poincaré plot (SD1) (Table 2). The standard deviation of the NN (RR) interval (SDNN), IRRR, TINN, HRV index, and standard deviation along the line of identity in the Poincaré plot (SD2) decreased significantly from pre-ISBPB to post-ISBPB. Although the mean arterial blood pressure and diastolic blood pressure increased significantly from baseline (pre-ISBPB), the heart rate did not change over the three time points. Pulse wave transit time, SPI, and peripheral oxygen saturation were significantly reduced from pre-ISBPB to post-ISBPB, while the PPG amplitude significantly increased (Table 3).
Three patients (7.1%), who included a 46-year-old male, a 58-year-old female, and a 52-year-old female, experienced HBEs 27, 96, and 63 min after the beginning of surgery (72, 146, and 163 min after transitioning to the seated position) and were treated with 10, 10, and 20 mg of ephedrine, respectively. As indicated by the three red circles in Fig. 4, the three patients’ absolute differences in lnLF and pupil diameter between pre-ISBPB and post-sitting were greater than their mean differences — 0.413 ln(ms2/Hz) for lnLF and 1.51 mm for pupil diameter. The spectrogram from one of these patients is presented in Supplementary Fig. 2.
Discussion
According to the results of our study, transitioning to the sitting position following right ISBPB reduced the baseline ipsilateral pupil size, CSNA, and parasympathetic nervous activity but did not change the sympathovagal balance. The extent of the changes in pupil size was positively correlated with that of the changes in SNA before ISBPB and after transition to the seated position following ISBPB.
The ISBPB-induced reduction in pupil size (miosis is one of the clinical signs of Horner’s syndrome) is attributed to the blockade of the stellate ganglion, to which local anesthetic placed around the brachial plexus spreads from the interscalene groove along the prevertebral fascia [3]. Because the stellate ganglion is a part of the second-order (preganglionic) neuron of the oculosympathetic pathway, its blockade blocks the terminal branches (the long ciliary nerves) of the third-order neuron at the anterior segment of the ipsilateral eye. As a result, the iris dilator muscle is relaxed by the unopposed parasympathetic action on the iris sphincter muscle, consequently leading to miosis of the pupil (anisocoria) [33].
The stellate ganglion also gives off the postganglionic fibers that travel to the heart via the cardiac sympathetic pathways [4]. The inferior cervical and 1st thoracic (T1) ganglia from the stellate ganglion form synapses with the inferior cervical and T1 cardiac nerves, respectively. The two sympathetic postganglionic fibers form the cardiac plexuses with other sympathetic postganglionic fibers from the superior and middle cervical ganglia and the 2nd to 5th thoracic paravertebral ganglia, as well as parasympathetic preganglionic fibers (branches of the vagal and recurrent laryngeal nerves) [4]. In particular, sympathetic neurons project from the craniomedial aspect of the right stellate ganglion and travel to the sinoatrial node, which regulates the heart rate [34]. Because periodic impulse formations by the sinoatrial node contribute to the HRV derived from RR intervals (heart rate) [35,36], a right SGB causes specific changes in the HRV parameters.
In the current study, the incidence of Horner’s syndrome was 97.6%, and lnLF, lnHF, and lnTP were decreased with no change in LF/HF after transitioning to the sitting position following a right ISBPB, which was similar to the results in a previous study where the incidence of Horner’s syndrome was not reported [31]. However, when the patients were in the supine position 30 min after the placement of the right ISBPB (prior to the sitting position), the decreases in the spectral power of HRV were not statistically significant. In another previous study, the incidence of Horner’s syndrome was 35.7%, and that study reported significant decreases in lnLF and lnHF in patients in the supine position [37]. Regrettably, the two abovementioned studies [31,37] did not use objective tools to determine the development of Horner’s syndrome. Hence, the incidence might be underestimated, so the effects of ISBPB-induced SGB on the HRV parameters are unclear. In contrast, we quantitatively measured the pupil diameter using pupillometry to determine if the patient developed Horner’s syndrome and found that most patients developed Horner’s syndrome. Therefore, we could measure the changes in autonomic nervous activity according to the various degrees of Horner’s syndrome.
lnLF, lnHF, and lnTP were reduced 30 min after a direct block of the right stellate ganglion using 8 ml of 1% mepivacaine in supine patients [38]. In contrast, our study showed no significant changes in those spectral domain HRV parameters, with some decreases in the time domain HRV parameters, which represent both SNA and parasympathetic nervous activity, between 25 and 30 min after ISBPB in the supine position. We assume that the indeterminate amount of a local anesthetic with a slow onset (ropivacaine) leaking outside the interscalene groove to the stellate ganglion and to the adjacent vagal nerve [39] produced a combined sympathetic and parasympathetic blockade, albeit incompletely.
Head-up tilt or the change from the supine to the sitting position after a right SGB caused no significant changes in the HRV parameters, unlike the normal physiologic response of autonomic nervous activity to positional changes (a reduction in HF and an increase in LF/HF) [9,10]. In our study, a change from the supine to the sitting position even reduced both the lnLF and lnHF from baseline without changing the LF/HF, possibly indicating that the incomplete sympathetic and parasympathetic blockade (30 min after ISBPB placement) became more intense more than 40 min after ISBPB placement (far past the onset of ropivacaine).
Because the reduction in CSNA by ISBPB-induced SGB has been assumed to be associated with the development of HBEs in the sitting position [31,40,41], an immediate measurement of CSNA is of utmost importance for patient safety. However, the conventional methods for the measurement of SNA require expensive equipment and technical support and therefore are not useful in intraoperative settings [13]. As one of the intraoperative standard monitoring parameters, ECG can be used for HRV analysis to noninvasively measure cardiac autonomic nervous activity. However, HRV analysis cannot provide instantaneous information about CSNA because at least 4 min are required to obtain LF values [18]. In addition, at least 10 min of acclimation time stabilizing the patients’ autonomic nervous activity is required to obtain reliable HRV parameters [31]. Furthermore, ECG waveforms are prone to artifacts that are caused by patient movement [42] or the use of electrocauterization to prevent bleeding [43]. The calculation of HRV variables with preprocessing of ECG waveforms is also time consuming. In contrast, the measurement of pupil diameter using a pupillometer is more feasible because it requires only 2 s (in this study) and is resistant to artifacts [19]. In addition, because pupil size reaches a plateau within seconds in a dark condition, its measurements require a few seconds of adaptation [44]. Given that SGB acts on both the oculosympathetic and cardiac sympathetic pathways, we expected that the changes in the pupil diameter reflected those in CSNA and found a significant linear correlation between them. Therefore, as an alternative to LF, pupillometry can be useful to assess the changes in CSNA after assuming the sitting position under the influence of an ISBPB-induced SGB.
An increase in the PPG amplitude is consistent with an increase in the blood flow of the ipsilateral upper limb after ISBPB [45,46]. However, because SGB alone can also increase the blood flow of the ipsilateral upper limb [47], we could not differentiate the effects of ISBPB and SGB on blood flow. In addition, the pulse wave transit time was reduced after ISBPB, which is contrary to the results of previous studies that showed that it increased after axillary brachial plexus block [48] and SGB [49]. Therefore, further studies are warranted to investigate the difference in the results between the previous study and ours.
Some limitations should be considered in this study. First, the pupil sizes were not measured while recording the ECG waveforms because the placement of a pupillometer on the eye would affect cardiac autonomic nervous activity by making the patients nervous, leading to ineffective assessments of the effects of ISBPB on cardiac autonomic nervous activity. Second, HRV analysis cannot assess the authentic effects of ISBPB-induced SGB on cardiac autonomic nervous activity because, in addition to the stellate ganglion, the superior and middle cervical ganglia and the 2nd to 5th thoracic paravertebral ganglia also contribute to CSNA. Therefore, the effects of ganglia other than the stellate ganglion on CSNA might have generated some significant errors that reduced the predictability of the regression model derived from the pupil size and lnLF changes. In this regard, the use of pupil size is limited in the assessment of how CSNA is affected by ISBPB-induced SGB. Nonetheless, we tried to exclude the effects of the abovementioned ganglia by giving patients sufficient acclimation time to stabilize their autonomic nervous activity. However, further studies are warranted to exclude the effects of ganglia other than the stellate ganglion and inconsistencies in the timing of measurement between pupil size and HRV. Third, due to the low incidence of HBEs in this study (3 out of 42 patients), the clinical usefulness of pupillometry to detect the development of HBEs could not be assessed. However, all three patients who developed HBEs had relatively large reductions in both the pupil size and lnLF. We hope that these three cases inspire further studies to investigate the usefulness of pupillometry to detect the development of HBEs. Last, a Bland–Altman agreement analysis could not be used to determine the agreement between the two methods (HRV and pupillometry) that measured the CSNA because they have different units — ln(ms2/Hz) versus mm. Therefore, we alternatively performed a simple linear regression to compare the two methods [50].
Our results showed that the changes in pupil size were linearly proportional to the changes in CSNA before ISBPB and after sitting following ISBPB. In conclusion, as an alternative to HRV, pupillometry can be used to measure the changes in CSNA after patients are placed in a sitting position after ISBPB.