Cardiac arrest due to coronary vasospasm after sugammadex administration -a case report-
Article information

Abstract
Background
Sugammadex is a widely used medication for the reversal of aminosteroid neuromuscular blockades. Although sugammadex is generally regarded to be safe, concerns about the risk of serious complications have emerged.
Case
A 57-year-old man without a history of coronary disease was scheduled for general anesthesia to undergo cardiac radiofrequency catheter ablation due to symptomatic persistent atrial fibrillation and flutter. At the end of the procedure, he was given 400 mg of sugammadex. A little later, the electrocardiogram showed a sudden ST elevation on the inferior leads, followed by cardiac arrest. The urgent coronary angiography demonstrated total collapse of the right coronary artery. After two injections of intra-coronary nitroglycerin, the vasospasm of the right coronary artery was completely resolved. The patient recovered without sequelae and was discharged on postoperative day 5.
Conclusions
Clinicians should pay close attention to the potential risk of coronary vasospasm, even cardiac arrest, after sugammadex administration.
Sugammadex, a modified gamma-cyclodextrin, is a widely used medication for the reversal of aminosteroid neuromuscular blockades including rocuronium and vecuronium. Although sugammadex is generally regarded to be relatively efficacious and safe, serious complications such as hypersensitivity reactions and severe bradycardia have been increasingly reported [1–4]. Recently, a few cases of coronary vasospasm after sugammadex administration were reported [5–8]. However, there is only one previous case in which the occurrence of coronary vasospasm was confirmed by coronary angiography [8]. Here, we present a case of cardiac arrest due to coronary vasospasm after sugammadex administration.
Case Report
This report was approved by the Institutional Review Board of the Jeju National University Hospital (IRB no. 2022-05-004), and the requirement for obtaining informed consent was waived.
A 57-year-old man, 173 cm tall and weighing 99 kg, was scheduled for general anesthesia to undergo cardiac radiofrequency catheter ablation (RFCA) due to symptomatic persistent atrial fibrillation and flutter. The patient was diagnosed with hypertension but had no history of chest pain to suspect coronary disease. The echocardiography showed normal wall motion and ejection fraction with concentric left ventricular hypertrophy and mild diastolic dysfunction. The patient had no history of allergies, and the other preoperative laboratory tests were normal.
When the patient entered the cardiac angiography room, routine monitoring systems including non-invasive blood pressure, pulse oximetry, and electrocardiogram (ECG) were implemented. His initial vital signs were a blood pressure of 138/76 mmHg, pulse oxygen saturation of 97%, and heart rate of 114 beats/min with atrial fibrillation. General anesthesia was induced with 400 mg of thiopental and 90 mg of rocuronium. Endotracheal intubation was done, and anesthesia was maintained with 2–3% sevoflurane in 50% oxygen/air. Invasive arterial blood pressure was monitored continuously at the femoral artery from the femoral sheath for RFCA. His vital signs were maintained within a systolic blood pressure of 80–120 mmHg, pulse oxygen saturation of 98–100%, and heart rate of 70–130 beats/min during the procedure. An additional 50 mg of rocuronium was administered to maintain muscle relaxation, so the total dose of rocuronium was 140 mg.
The RFCA was completed uneventfully and took 3 h and 15 min. The ECG and other vital signs were normal. We stopped sevoflurane administration and gave him 400 mg of sugammadex (BridionⓇ, Merck and Co., USA). Within two minutes of the sugammadex administration, the ECG suddenly demonstrated ST elevation on the inferior leads, so an occlusion of the right coronary artery was strongly suspected (Fig. 1). His vital signs included a blood pressure of 80/57 mmHg, pulse oxygen saturation of 100%, and heart rate of 77 beats/min. There were no signs of hypersensitivity reactions, such as urticaria, wheals, swelling, or increased airway pressure.
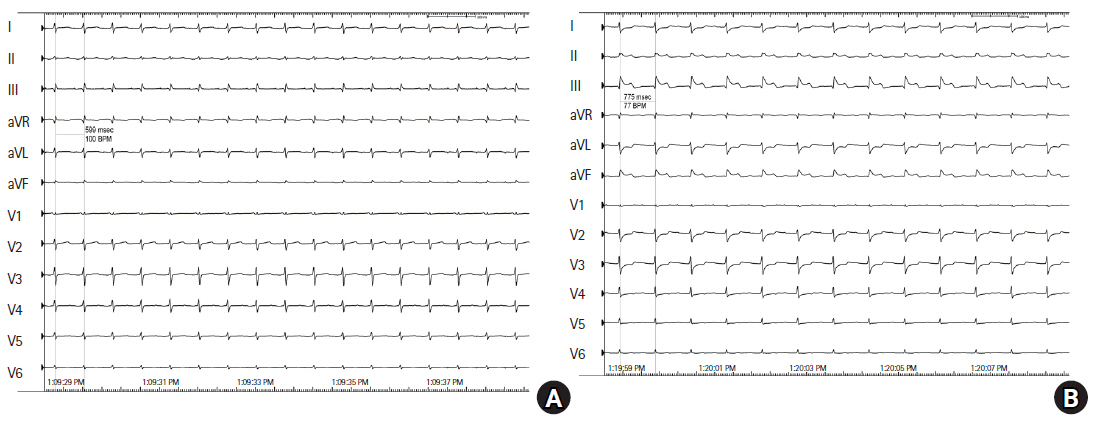
Electrocardiogram (ECG). (A) At the end of radiofrequency catheter ablation, the ECG showed normal. (B) After sugammadex administration, it suddenly demonstrated ST elevation on the inferior leads.
Coronary angiography was initiated immediately, simultaneously with the infusion of norepinephrine at 16 μg/min and dopamine at 20 μg/kg/min. A little later, the patient’s heart rate gradually decreased, and the ECG showed pulseless electrical activity. Cardiac movement was not identified on X-ray fluoroscopy, so chest compressions were started immediately. Epinephrine (1 mg) was injected, and an external pacemaker was applied, but he did not respond. Chest compression was continued and an additional 1 mg of epinephrine was injected. At that time, coronary angiography demonstrated total collapse of the right coronary artery, and 0.2 mg of intra-coronary nitroglycerin was injected. The right coronary artery was partially dilated, and the ECG showed ventricular fibrillation. Cardioversion with 200 J was done, and the ECG returned to normal sinus rhythm. Additional intra-coronary nitroglycerin was injected, and the vasospasm of the right coronary artery was completely resolved (Fig. 2). Afterward, the patient underwent a left coronary artery angiogram, which revealed a normal pattern. His blood pressure became normal with the infusion of norepinephrine at 8 μg/min, dopamine at 10 μg/kg/min, and nitroglycerin at 10 μg/kg/min. However, because the echocardiography showed abnormal wall motion and low ejection fraction, extracorporeal membrane oxygenation was applied, and he was transferred to the intensive care unit.
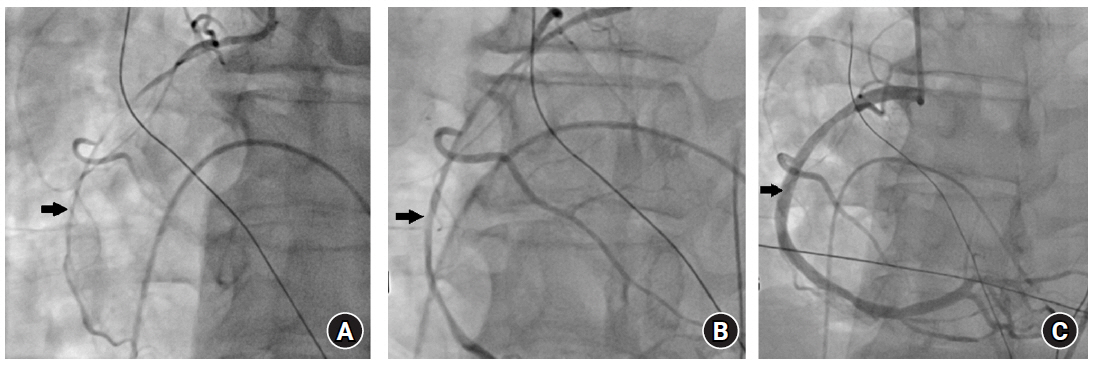
Left anterior oblique view on coronary angiography. (A) After cardiac arrest, the right coronary artery totally collapsed. (B) After the first injection of intra-coronary nitroglycerin, the right coronary artery was partially dilated. (C) After an additional injection of intra-coronary nitroglycerin, the vasospasm of the right coronary artery was completely resolved. Black arrow: right coronary artery.
On postoperative day 1, the patient’s trachea was extubated and extracorporeal membrane oxygenation was removed. On postoperative day 2, his vital signs remained stable without vasopressors and he was transferred to the general ward. There were no symptoms of chest pain, and there was no clinical basis to suspect coronary disease. The echocardiography showed normal wall motion and ejection fraction, and the ECG showed normal. He was discharged on postoperative day 5 without sequelae.
Discussion
In the present case, the patient had sudden ST elevation on the inferior leads after sugammadex administration, followed by cardiac arrest. Since he had undergone RFCA in the cardiac angiography room, coronary angiography could be initiated immediately and confirmed the total collapse of the right coronary artery. After two injections of intra-coronary nitroglycerin, the vasospasm of the right coronary artery was completely resolved, and the patient recovered. Because coronary vasospasms related to RFCA mostly occur during the main procedure, especially after transseptal puncture [9], we do not believe that this case was related to RFCA complications. In addition, considering the timing between coronary vasospasm and sugammadex administration, it would be appropriate to suspect that sugammadex was the cause of the event.
Sugammadex, a modified gamma-cyclodextrin, is a widely used medication for the reversal of aminosteroid neuromuscular blockades including rocuronium and vecuronium. Although sugammadex is generally regarded to be relatively efficacious and safe, serious complications have been increasingly reported. Hypersensitivity reaction is a well-known complication of sugammadex, with varying degrees of severity. The most frequent signs and symptoms are skin rash, swelling, and bronchospasm, with or without severe hypotension and tachycardia [1,2]. Hypersensitivity reactions can occur without a history of previous sugammadex exposure [10]. Miyazaki et al. [11] reported that the incidence of intraoperative anaphylaxis associated with sugammadex was 0.039%.
Another serious complication is profound bradycardia with a heart rate of 20–30 beats/min with or without hypotension, which can be treated with repeated injections of atropine and ephedrine [12,13]. However, some patients developed cardiac arrest wherein cardiopulmonary resuscitation was needed, and some resulted in death [3,4,14]. While cardiovascular collapse after sugammadex administration has been thought to be a result of anaphylaxis, these recent reports suggested that this can occur due to unknown mechanisms without evidence of anaphylaxis.
Recently, four cases of coronary vasospasm after sugammadex administration were reported. Two papers suggested the direct effect of sugammadex on the coronary vasospasm. Ko et al. [7] reported the case of a 76-year-old man who had ventricular premature contraction bigeminy, followed by cardiac arrest after sugammadex administration. He was postoperatively diagnosed with variant angina, and a skin allergy test showed negative results, so the authors suggested that sugammadex could directly cause coronary vasospasm. Hoshino et al. [5] also reported the case of a patient who had ST depression, followed by cardiac arrest after sugammadex administration. The patient was postoperatively diagnosed with variant angina, and sugammadex was considered to be the direct cause of the coronary vasospasm.
Other two papers reported cases of coronary vasospasm caused by Kounis syndrome. These patients developed ST elevation/depression after sugammadex administration, and skin allergy tests showed positive results for sugammadex or rocuronium-sugammadex complex [6,8]. Kounis syndrome is a rare, acute coronary syndrome associated with hypersensitivity reactions. During an allergic event, activated mast cells release inflammatory mediators such as histamine, tryptase, and a variety of cytokines. These mediators impact hemodynamic functions, resulting in generalized vasodilation and coronary vasospasm [15].
Our patient developed cardiac arrest following sudden ST elevation after sugammadex administration, and the total collapse of the right coronary artery was confirmed by urgent coronary angiography. There were no signs of hypersensitivity reactions such as urticaria, wheals, swelling, or increased airway pressure. Therefore, a direct effect of sugammadex was thought to be the most probable cause of coronary vasospasm.
However, Kounis syndrome might occur in the absence of typical skin rash or other hypersensitivity symptoms [8]. Therefore, it would be better to check the levels of inflammatory mediators or perform a skin prick test to accurately determine the cause. In the present case, we failed to check the levels of inflammatory mediators at the time of the event. Afterward, we recommended a skin prick test, but the patient refused. Therefore, we cannot completely rule out the possibility of Kounis syndrome. However, the important point is that whatever the cause might be, there is a possibility of coronary vasospasm after sugammadex administration. And, if the degree of coronary vasospasm is severe enough to lead to cardiovascular collapse, the current acute coronary event protocol, including cardiopulmonary resuscitation, should be initiated immediately. Additionally, if Kounis syndrome is suspected, the use of corticosteroids and antihistamines with mast-cell stabilizers may help to relieve the symptoms [15].
In conclusion, the present case demonstrated cardiac arrest due to coronary vasospasm in a patient who received sugammadex. Therefore, clinicians should pay close attention to the potential risk of coronary vasospasm, even cardiac arrest, after sugammadex administration.
Notes
Funding
None.
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Data Availability
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Author Contributions
Ki Yung Boo (Data curation; Writing – review & editing)
Sang Hyun Park (Conceptualization; Writing – review & editing)
Sun Kyung Park (Writing – review & editing)
Changrock Na (Writing – review & editing)
Hyun Jung Kim (Conceptualization; Writing – original draft)