Point-of-care ultrasonography as rescue for popliteal artery cannulation in prone position
Article information

The prone position is among the many positions used during various neurosurgical and orthopedic surgeries (posterior fossa tumors and spine). Complications associated with prone positioning include stroke, upper airway obstruction, endotracheal tube dislodgement and brachial plexus injury, among others. Arterial cannula displacement during positioning or in the middle of an ongoing major surgery is a nightmare to anesthesiologists, due to difficulties of accessing commonly used arteries for arterial cannulation. It becomes even more challenging when the extremities are not available for cannulation in patients with polytrauma. The popliteal artery can be a very useful option in this situation. Point-of-care ultrasonography (POCUS) has made vascular structures easily accessible for diagnostic and therapeutic purposes, which were previously impossible with blind techniques [1,2]. POCUS can be an invaluable tool for popliteal artery cannulation due to its deeper location and presence of the popliteal vein above it [3].
Written informed consent obtained from the patient. A 60-year-old woman with history of fall from a 6-m height was scheduled for pedicle screw fixation of L1 vertebral fracture. She also had bilateral upper limb fractures along with right metatarsal fracture. She was known to be diabetic and hypertensive with irregular medications. Due to intraoperative hemodynamic instability and difficulty of measuring noninvasive blood pressure, arterial cannulation (over the needle technique) was performed in the left dorsalis pedis artery. During the intraoperative period, the arterial cannula was displaced, as indicated by damping in the arterial wave tracing. After repeated failed attempts to cannulate the left posterior tibial artery, we decided to cannulate the left popliteal artery. The left popliteal fossa was cleaned and draped. An ultrasound image of the popliteal artery with the vein lying above and the nerve bundle below was obtained (Fig. 1A). Colored Doppler was used to improve identification of the artery. The artery was found just below the vein from the roof of the popliteal fossa. Hence, it could not be punctured perpendicularly. The vein was to be bypassed by puncturing the artery from the medial or lateral side using the Seldinger technique (Fig. 1B).
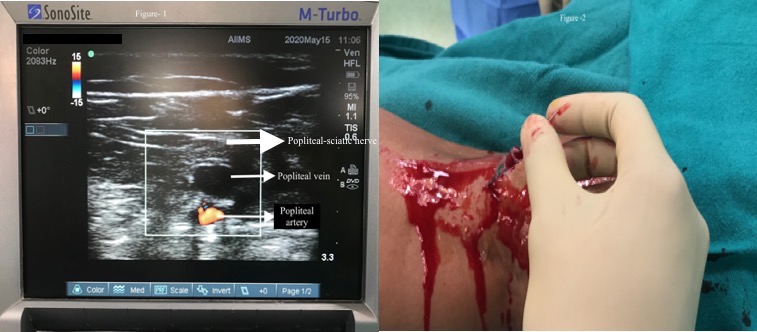
(A) Ultrasound image depicting the popliteal artery anatomy (colored Doppler) and (B) the popliteal artery cannulation with guidewire in situ.
The popliteal artery is accessed in the popliteal fossa, which is bound by the biceps femoris, plantaris, and lateral head of the gastrocnemius laterally and by the semitendinosus, semimembranosus, and medial head of the gastrocnemius medially. The floor is formed by the knee joint, and the roof is formed by the skin, subcutaneous, and fascia lata [2]. The popliteal artery has an average diameter of 7.4–9.5 mm [3]. The popliteal artery and vein are present in the common sheath, and the vein crosses the artery from the lateral to medial as we move from above to below. Easy accessibility in the prone position, reliable anatomy, and large diameter were advantages of popliteal artery cannulation. However, because of its deep location and adjacent placement to the popliteal vein, only ultrasound-guided placement is feasible, and the Seldinger technique is a better option than the over-the-needle technique.
A paucity of published literature regarding the popliteal artery cannulation has been observed. Villelli et al. [4] reported the popliteal artery cannulation for digital subtraction angiography in the prone position in three patients without any complications. Bala et al. [5] performed popliteal artery cannulation in a patient with severe ARDS in the intensive care unit. Our patient was followed up in the postoperative period after the arterial cannula removal with ultrasonography for the popliteal artery patency. No thrombus or hematoma was detected around the popliteal artery. We suggest further studies on cannulation of popliteal artery required to establish the safety and feasibility for invasive blood pressure monitoring.
Notes
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Chitta Ranjan Mohanty (Conceptualization; Validation; Visualization; Writing – original draft; Writing – review & editing)
Snigdha Ranjan Bellapukonda (Supervision; Visualization; Writing – review & editing)
Nitish Topono (Writing – review & editing)
Satyaki Sarkar (Supervision; Writing – review & editing)
Priyank Tapuria (Writing – review & editing)