Ultrasound guidance for neuraxial anesthesia has gained popularity over the last two decades [1]. This new application of technology also facilitates spinal anesthesia in patients with challenging anatomy, such as those with scoliosis or obesity, or elderly patients [2,3]. Infiniti PlusŌäó (CIVCO Medical Solutions, Kalona, IA, USA) is a needle-guidance system that was recently developed to assist clinicians in performing ultrasound-guided nerve blocks. A needle-guidance system allows efficient needle movement with improved needle shaft and tip visualization. A needle-guidance system has been used for peripheral nerve blocks with a high-frequency ultrasound probe [4]. We used the Infiniti Plus needle-guidance system with a low-frequency ultrasound probe in spinal anesthesia administered by a single physician to two patients with difficult spinal anesthesia.
A 62-year-old man was scheduled for left total hip replacement. He weighed 96 kg and had a body mass index of 30.4 kg/m2. The L3-L5 spinous processes were not palpable, and the precise neuraxial midline was difficult to determine clinically. After obtaining informed consent, standard American Society of Anesthesiologists monitors and intravenous access was established and premedication with midazolam 2 mg and fentanyl 50 ┬Ąg was given. He was positioned in the sitting position. Three trials of subarachnoid access without ultrasound guidance by an experienced anesthesiologist failed: bone was encountered in two trials, while in the third trial the cerebrospinal fluid (CSF) flow was not consistent (slow flow initially and no CSF was returned in the other three quadrants after turning the needle). Subsequently, spinal anesthesia was successful with an ultrasound-guided needle-guidance system at the first attempt.
The second case was a 62-year-old man who was scheduled for total hip replacement. Spinal anesthesia had been unsuccessful in the past. His medical history included kyphoscoliosis. No lumbar X-ray was available for a more detailed anatomical examination. On palpation, it was difficult to determine the midline. He initially refused spinal anesthesia, as his previous experience was traumatic, and he had back pain after the previous procedure. After discussion, he agreed to proceed with spinal anesthesia under ultrasound guidance. After obtaining informed consent, routine monitoring and intravenous access premedication was given for a spinal anesthesia procedure with an ultrasound-guided needle-guidance system, and spinal anesthesia was successful at the first attempt.
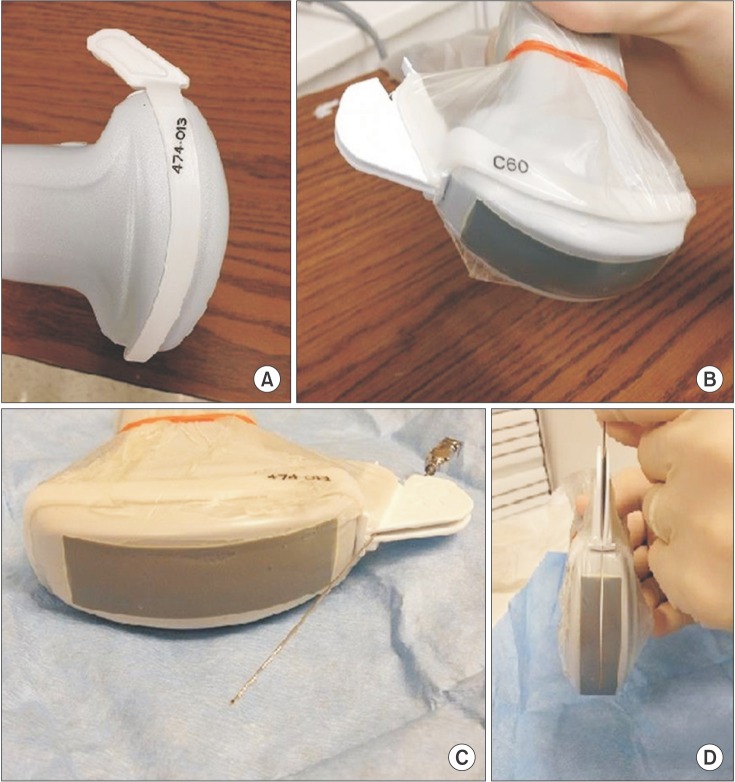
We used the SonoSite S nerve (SonoSite, Bothell, WA, USA) ultrasound machine with a low-frequency (2ŌĆō5 MHz) curvilinear transducer. The ultrasound probe was covered with a sterile sleeve with sterile gel applied on the probe of the Infiniti Plus needle-guidance system (Fig. 1). The ultrasound probe was held in the left hand and the needle in the right hand at the clinician's preference, while the ultrasound machine was across the table, in the line of sight of the clinician. Scanning started with the long axis view (paramedian sagittal oblique view) at the sacrum, and then moved cephalad to the lumbar spine to identify the paramedian sagittal oblique interlaminar view at the target lumbar level for the spinal block. We used a paramedian longitudinal oblique approach with needle insertion directed caudal to cephalad. Meticulous care was taken to ensure that the needle insertion site was free of gel. The skin and subcutaneous tissue were infiltrated with 2 ml of 2% lidocaine.
The intervertebral level used for the attempt was selected based on the relative ease of visualizing the ligamentum flavumŌĆōdura mater complex. The clinician selected L4-5 in the first case and L3-4 in the second. A 22-gauge, 90-mm-long echogenic spinal needle (Pajunk Medizintechnologie, Geisingen, Germany) was used in both cases. The spinal needle was guided in a caudal-to-cephalic direction via a paramedian oblique interlaminar approach, with the clinician holding both the probe and the needle. The clinician needs to make subtle adjustments in needle trajectory to improve the visualization of the needle while it is inside the needle guidance system. Additionally, the trajectory is changed while the needle is in the muscles to reach the interlaminar space.
When the needle tip reached the interlaminar space close to the posterior complex, the needle visualization deteriorated, while the clinician felt increased resistance. On advancing the needle a total of 4 cm, a sensation of giving was felt on entering the intrathecal space.
After confirming the flow of CSF in both cases, 15 mg bupivacaine was injected. Local anesthetic spread within the subarachnoid space was verified using ultrasound color Doppler images in the transverse interlaminar view.
Each patient required one needle insertion under ultrasound. The anesthesiologist rated the difficulty of insertion as moderate in both patients and both patients reported a very good satisfaction score with no complications. We were able to visualize the needle all the way to the interlaminar space, until the needle approached the posterior complex.
Both patients underwent successful surgery with spinal anesthesia and were discharged without any complications of spinal anesthesia.
To our knowledge, this is the first report on the use of low-frequency real-time ultrasound-guided spinal anesthesia with an echogenic spinal needle using needle guidance in clinical practice. We demonstrated that the needle-guidance system is practical, with improved visualization of the needle at depths greater than 4 cm in patients with a history of difficult spinal anesthesia. Future studies are needed to establish its utility with a larger number of patients and a wider variety of block techniques.