In spite of the many benefits of percutaneous lumbar sympathectomy (PLS) it also has several complications or side effects such as genitofemoral neuralgia, lumbar plexus damage or damages to organs and blood vessels. Among them, the damages on kidney or ureter are rare but serious complications [1,2]. Avoiding these complications, the needle entry point should not exceed a certain distance to the midline as cL shown in Fig. 1. At the same time, the entry point should also keep some distance to the midline to avoid a damage of the lumbar plexus cM as shown in Fig. 1.
Few studies have been conducted in order to find out this safe entry point on the skin [3,4,5]. These studies tried to find the relationship between the measurements and the characteristics of the patients also. However, its results showed some confusing outcomes. Koisuka et al. [3] did not directly mention the difference of a maximum lateral distance (same as cL in Fig. 1) between levels. They just respectively described the outcome of measurements at each different level and showed the correlation coefficient of each procedure-related distance for each covariate one by one. The correlation coefficient, however, is just a degree of the relationship. The investigators should have analyzed it with all the covariates together and should have shown the coefficients for each covariate. Weyland et al. [4] mentioned different cL between the levels. Kim et al. [5] said that the cL at each level were not different from each other. They also showed the measurements of cL separately according to each covariate such as lumbar level, gender and age. However, covariates should have been considered at the same time. For example, if there is a high aged patient of female gender who is scheduled to receive L3 PLS, which estimator should be used to perform PLS regarding high age, female and L3 estimator of cL? Therefore, the current study was conducted to investigate which covariates should be used with which influence on cL and other measurements.
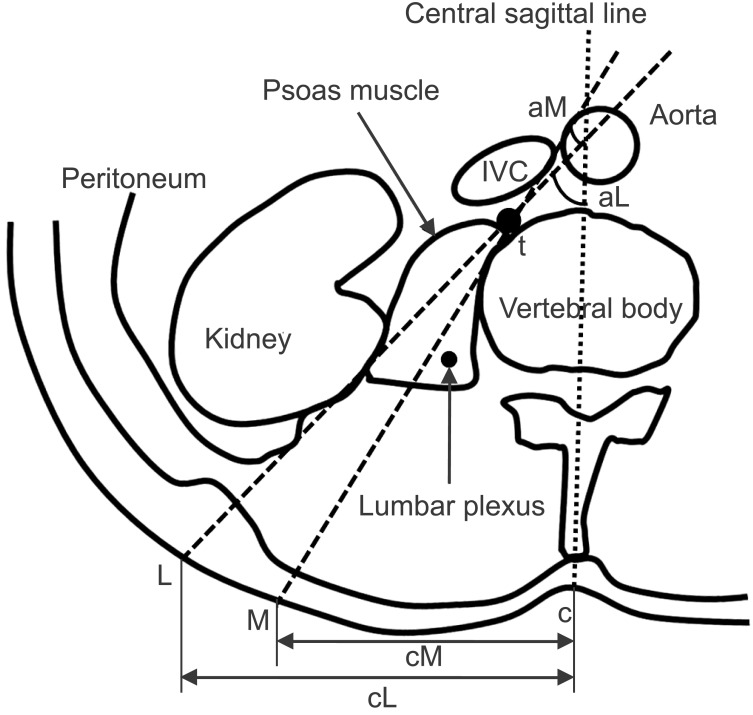
CT images of patients aged between 30 and 70 years were investigated from the data base of the patients' information center of the hospital. The study was approved by the Institutional Review Board. CT images were selected of patients without a severe disease such as abdominal parenchymal or peritoneal disease and musculoskeletal abnormalities around the lumbar region. Transverse section that crosses at the lower third of L2 or upper third of L3 vertebral body was selected. As shown in Fig. 1, c is the point where skin meets the central sagittal line. t is a junction of the anterolateral surfaces of the vertebral body and the psoas muscle where the lumbar sympathetic ganglion is supposed to be located. L is a maximum lateral skin point which meets the line drawn from t to the skin tangent to the parietal peritoneum. M is the most medial skin point that meets the line drawn from t to the skin as tangent as possible to the vertebral body and not to injure the lumbar plexus. The cL distance means the maximum lateral margin where the needle can enter the skin and reach the target point avoiding a kidney injury. cM indicates the medial margin for the needle where it can be inserted without obstacles such as the vertebral body itself or a lumbar plexus injury. The angles aM and aL were measured, build up between the central sagittal line and tM or tL lines.
To find out the relations between patients covariates and measured data, multiple linear mixed effect modeling was done on the measurements with NONMEM® (version 7.2, Icon Development Solutions, Ellicott City, MD, USA). The potential covariates affecting parameters were explored for age, body weight, height and body mass index (BMI). The minimal value of the NONMEM objective function value (OFV) and akaike information criteria were used to test the statistical significance of the additional parameter effects. An addition of parameter was determined by an OFV of at least 3.84 points.
CT scans of 40 patients were investigated. The averages (SD) were as follows: age 55.2 (┬▒ 12.7) years, weight 63.6 (┬▒ 9.9) kg, height 164.8 (┬▒ 8.2) kg and BMI 23.3 (┬▒ 2.5) m/kg2. The gender distribution was 20/20. The age covariate was modeled for the cL, cM, aL and aM measurements. BMI covariates were modeled for cL. The cL, cM, aL and aM of L2 or L3 were best described with gender, age or BMI covariates as follows:
The measurements of male were generally longer or wider than that of females. The Covariate modeling revealed a relation of cL is with gender, age and BMI of the patients. cL became shorter with increasing age. On the contrary, as larger the BMI, as longer was the cL. The negative coefficient of age covariate was assumed to be associated with a reducing muscular mass and subcutaneous fat during the aging process. Such simulation gives us a warning to be very cautious about patients with an extreme age and a lean body. cL showed a great difference if we compared a 30 years old male with BMI 30 and an 80 years female with BMI 18. The difference was as much as 53.3 mm (91.4 vs. 39.1). The safe angles that were defined as difference between aL and aM were 19o for young male and 9.2o for old female. So, as already mentioned, a very careful consideration should be done if a PLS is performed in a person with high age and lean body mass.
Even the number of subjects included in this study was small, the mixed effect modeling has been thought as an effective method to find out the interindividual variabilities. There might be a risk to apply resulted equations to subjects whose covariates are out of bound of this study. In the clinical reality, the outmost lateral point (cL) would be shorter than the value of this study, because the investigated images were filmed in a supine position while the PLS is usually done in a prone position.
Conclusively, this study could show quantitative relationships between the safety windows for PLS and covariates such as gender, BMI, age and vertebral levels at the same time.