Central venous catheterization is performed in the operating room, intensive care unit and emergency room for various reasons. Internal jugular vein is preferred in the operating room due to little chance of pneumothorax and straight route for catheterization to the right atrium. We experienced a case of central venous catheter malposition to cephalad in the right internal jugular vein.
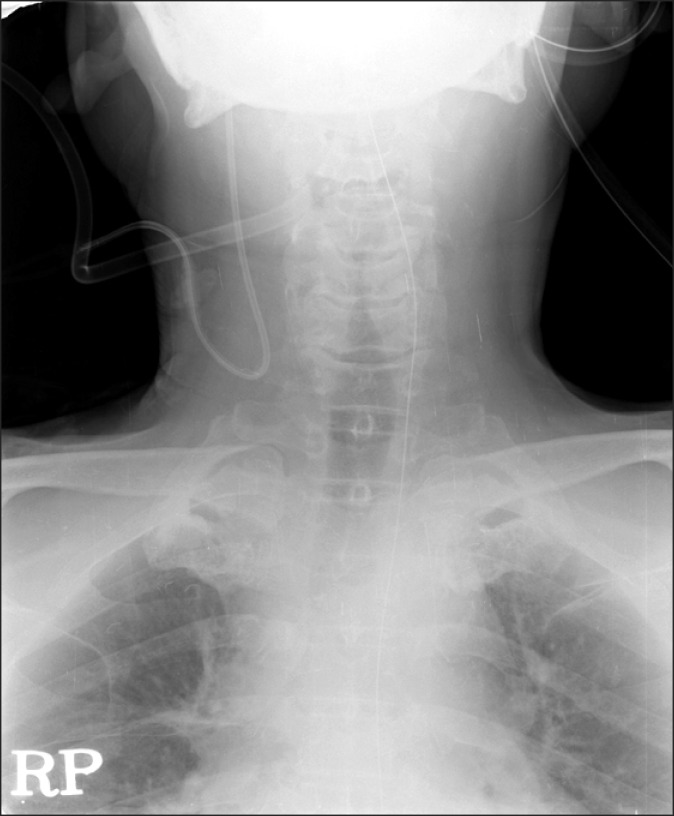
A 60-year-old man, 176 cm in height and 82 kg in weight, was presented for Whipple's operation due to the bile duct cancer. After completion of anesthesia induction and intubation, patient's head was turned left in Trendelenburg position. After skin disinfection, 18 guage, 2 inch thin-walled needle was inserted at the point of sternocleidomastoid (SCM) muscle apex along with medial border of lateral head of SCM muscle about angle of 45 degree to skin without using the finder needle. At the same time, anesthesiologist's left 2nd, 3rd, and 4th fingers palpated the patient's right carotid artery for avoiding arterial puncture. However, blood was not aspirated, needle was reinserted more medial direction about angle of 70 degree to skin. After aspiration of venous blood from needle, the J shape guide wire was introduced via the guiding needle using Seldinger technique. Introduction of 20 cm of J-shaped wire was done without any problem, except some resistance at 5 cm depth of the internal jugural vein. Seven Fr double lumen catheter (Prime-S®, Sungwon medical, Cheongju, Korea) was advanced to the following J-shaped wire. Blood aspiration was done to remove the air in catheter without any resistance. Catheter was sutured at the proper site and surgery was done as planned. After the operation, the patient was transferred to an intensive care unit. Head and neck antero-posterior view X-ray was checked because the central venous catheter was not seen on chest X-ray. Antero-posterior view of the head and neck showed that central venous catheter was bent sharply to the cephalad in the right internal jugular vein (Fig. 1). We removed malpositioned catheter and reinserted central venous catheter via the same side subclavian vein. The proper position of subcalvian catheter was confirmed by a chest X-ray and the patient discharged at postoperative day 13.
As one of the various complications, catheter malposition via Internal jugular vein (IJV) can be associated with central venous catheterization via IJV (5.3%) [1]. There are many case reports of malpositioning central venous catheter that were positioned in the jugular venous arch via the right subclavian vein [2], in the internal thoracic vein via the internal jugular vein [3] etc. However, this is the first case of malposition of the catheter, which was bent upward. Bending the catheter is very rare because the right internal jugular vein is the straight route for catheterization to the right atrium. Although there was some resistance during introduction of the J-shaped wire, blood aspiration via catheter was normal, dripping of the fluid seemed normal and central venous pressure curve showed no other abnormal findings. We postulate that the J-shaped wire was bent in the cephalad direction at the moment of resistance. The other postulated cause is an acute angle of the introducing needle when it punctured the internal jugular vein. We cannot rule out the anatomical variation of the external jugular vein and internal jugular vein. Deslaugiers et al. [4] reported that 60% of the external jugular vein is drained to junction of the internal jugular vein and subclavian vein, drained to the subclavian vein in 36%, and drained to the internal jugular vein in 4%. However, we did not confirm the anatomical variation with venous angiogram. It seems that we should be careful when we introduce the wire with some resistance. Malpositioning of the catheter results in monitoring inaccurate central venous pressure, damage to vascular wall, and forming the thrombus. However, the chance of thrombus formation is very low since the blood flow velocity is very fast in the internal jugular vein. In addition, it is impossible that the infused drug inflows to the brain. Although, the most precise method to confirm the complications is examination of the X-ray after the catheterization, ultrasono-guided central venous catheter placement is increasing the success rate, shortening the procedure time, decreasing the complication and the easiest method for acknowledging the direction of catheter, needle and guide wire during the entire catheterization process [5].
In summary, if there is any problem during the central venous catheterization, ultrasonography can be used for optimal catheter placement, and prevention of complications. Additionally, X-ray must be examined to confirm the position of the catheter and incidental complication.