Klippel-Treanunay syndrome (KTS) is a rare congenital overgrowth disorder associated with vascular anomalies first described by Paul Treanunay in 1900 [1]. It is usually associated with complex vascular malformations such as cutaneous hemangiomas and varicosities in extremities. Such lesions tend to bleed easily because of the fragility of the blood vessels [2]. We present a case of a massive bleeding during the surgery of correction of femur shaft fracture in a patient with KTS.
A 36-year-old man was diagnosed with a fracture of the right femur shaft and scheduled for close reduction and internal fixation. He had visited a hospital in the United States about 2 years ago for the evaluation of the varicose vein in his right lower leg and diagnosed as KTS at that time.
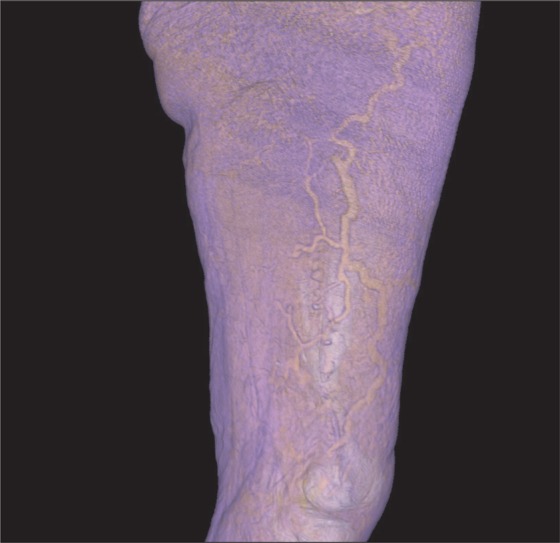
There were no abnormal findings on preoperative laboratory examination. Magnetic resonance angiography of the brain for the evaluation of the vascular abnormalities did not showed any abnormal findings and the airway examination was also normal. The computed tomographic angiography of the lower limb demonstrated the prominent varicosity in the subcutaneous layer and the vastus muscles in the right thigh (Fig. 1).
On the day of surgery, the general anesthesia was applied in the standard manner without premedication. Anesthesia was induced with 1.5 mg/kg of propofol and 1.0 µg/kg of fentanyl. Rocuronium was given at a dose of 0.6 mg/kg to facilitate endotracheal intubation. The lung was ventilated with a mixture of oxygen and air (FiO2 0.4) and desflurane to adjust normocapnia. The central venous catheter was inserted via the right internal jugular vein after induction of general anesthesia.
After the closed reduction under fluoroscopy guidance was done, the skin incision of about one-inch was applied. After evacuation of the hematoma, sudden spurt of bleeding was encountered and immediate hemostasis was nearly impossible. Bleeding of more than 2,000 ml occurred within the 5 minutes after the skin incision. The blood pressure was continued to drop about 60/40 mmHg and heart rate was increased up to 130 beats/min. As rapid intravenous infusion was required, the triple lumen hemodialysis catheter (Arrow-Howes™ multi-lumen catheter, Arrow International, Inc., Reading, PA, USA) was inserted via left internal jugular catheter and FMS 2000 (Belmont Instrument Corp., Billerica, MA, USA) was connected after priming. Intravenous solutions, packed red cells, fresh frozen plasma and various medication including vasopressors and inotropics were administered via internal jugular vein catheter. Arterial line was also cannulated via right radial artery for the continuous monitoring of blood pressure and laboratory exam. After blunt vessel ligation was done by vascular surgeon, major bleeding was halted and vital signs were become stable (blood pressure, 103/66 mmHg; heart rate, 96 beats/min; body temperature 36.1℃). The hemoglobin and hematocrit examed at that time was 10.1 mg/dl and 29.4%. A total of ten units of packed red cell, 3 units of fresh frozen plasma, 1,800 ml of colloid solution (Voluven™, Fresenius Kabi, Bad Homberg, Germany) and 2,000 ml of crystalloid solution were administered during operation. The estimated blood loss was approximately 5,000 ml and urine output was 850 ml.
The patient was transferred to intensive care unit for closed observation but the hemoglobin still continued to drop. His postoperative labs showed: hemoglobin 7.9 mg/dl, platelets 88,000/mm3, PT and aPTT were 13.8 sec and 32.9 sec. Additional 2 units of packed red cells were transfused. On the third postoperative day, he transferred to the surgical ward. One month after the operation, he was discharged without any specific problems except difficulty in ambulation.
Usually, the diagnosis of KTWS can be made when any two of the triad of features: capillary malformations (port wine stain), hypertrophy of soft tissue or bone, varicose veins. Abnormalities in vessels can occur either superficially or deeply and even perforating vessels can be affected [2]. Management of disease itself is mostly conservative but a multidisciplinary approach is required to treat and prevent of associated complications. When surgical management is needed, the use of minimal invasive techniques is recommended.
Although there have been no established strategies in the anesthetic management of the patients with KTS undergoing surgery, some preoperative evaluations for KTS patients were previously recommended. First, anesthesiologist should be considered about potentially difficult airway management because KTS patients often present soft tissue hypertrophy in the mouth, hypopharynx and facial anomalies [1]. Second, neuraxial anesthesia in these patients was considered contraindicated because of potential neurovascular malformations in spinal cord and surrounding structures [3]. Third, the possibility of excessive intraoperative blood loss should be always considered even in minor surgery because of widespread varicosities and venous malformations [2]. Forth, the risk of venous thrombosis and pulmonary thromboembolism is relatively high in KTS patients. Chronic coagulopathy such as disseminated intravascular coagulation also can be encountered in these patients [4]. Finally, intracerebral aneurysm can be present in KTS patients and it can be ruptured during perioperative period [5].
In our patient, the airway examination and magnetic resonance angiography of the brain was performed before surgery and cannot find any abnormalities. The computed tomographic angiography of the lower limb was also done and revealed relatively low varicosities around the condyle of femur. Anticoagulation was done at 8 hours before surgey using low molecular weight heparin and the operation was closed reduction of femur shaft. However, the bleeding was more extensive than we expected and very hard to manage. In our opinion, unrecognized vessel injuries during the closed reduction of femur shaft may aggravate the amount of bleeding than we expected in our patient.
In conclusion, we present a case of massive bleeding in KTS patient who undergoing close reduction and internal fixation for correction of the femur shaft fracture. Physicians should always aware of unexpected bleeding in KTS patients even in minimal invasive surgery and prepare inadvertent events during perioperative period.