Comparison of two topographical airway length measurements in adults
Article information
Abstract
Background
A correct estimate of the tracheal tube insertion depth can prevent complications, including endobronchial intubation and vocal cord trauma. We evaluated a new topographical method for endotracheal tube positioning relative to the carina, using a well-known prior topographical method for comparison.
Methods
One hundred adult (male 50, female 50) patients were studied. The comparison topographic length (in cm) was measured by adding the distance between the right mouth corner and the right mandibular angle to the distance between the right mandibular angle and the center of the sternal manubrium. The new endotracheal tube insertion depth (in cm) was determined by adding the distance between the right mouth corner and the vocal cords, measured with the endotracheal tube itself, to the distance between the thyroid prominence and the manubriosternal joint, and then subtracting 4 cm. After intubation, the endotracheal tube was positioned properly at the right mouth corner and the endotracheal tube tip was evaluated using a fiberoptic bronchoscope at the carina.
Results
The distances from the tip of the endotracheal tube to the carina were not significantly different between the methods in the same gender. However, our method allowed endotracheal tube tip placement between 3 cm and 5 cm, above the carina more frequently than the prior method in males.
Conclusions
The new topographical method can be used as a guide to positioning the endotracheal tubes.
Introduction
Malpositioning of the endotracheal tube (ETT), within the airway, can lead to serious complications including endobronchial intubation, vocal cord paralysis and accidental extubation [1-3].
The manubriosternal joint is typically on the same horizontal plane as the tracheal carina and has been used to estimate the airway length [4-6]. The laryngeal prominence is in the midline of the thyroid cartilage and results from the fusion of the anterior border of the laminae, at an angle of approximately 90° in male patients, and 120° in female patients. Topographic studies place the true vocal cords at a level corresponding to halfway up the thyroid cartilage [7].
We determined the airway length by adding the distance from the right mouth corner to the vocal cords, using the ETT itself [8] to the distance from the thyroid prominence to the center of the manubriosternal joint.
We compared our new method for estimating the insertion depth of ETT with the prior topographical method of Evron et al. [5], which also uses the manubriosternal joint in male and female adult patients, respectively.
Materials and Methods
The study was approved by the Institutional Review Board, and written informed consent was obtained from each patient. One hundred adult patients (male 50, female 50, American Society of Anesthesiologists physical status I or II) that were undergoing a routine elective surgery under general anesthesia were studied. Patients with anatomical defects of the face, neck, or upper airway were excluded from the study.
Patients were placed on the operation table with the head in the neutral position. Routine monitors were used. Induction of anesthesia was achieved with propofol 1.5 mg/kg, intravenously. Muscle relaxation was obtained with rocuronium 0.6 mg/kg, intravenously. Anesthesia was maintained with sevoflurane (2-3%).
First, Evron et al. [5] topographic length (in cm) was measured, by adding the distance measured from the right mouth corner to the right mandibular angle, and the distance measured from the right mandibular angle to the center of a line drawn transversally through the middle of the sternal manubrium.
Second, the distance from the thyroid prominence to the center of the manubriosternal joint (D1) was measured on the surface of the patient's chest (Fig. 1). After a loss of all four twitches from the train-of-four obtained by ulnar nerve stimulation, laryngoscopy was performed with a number 3 Macintosh blade of the laryngoscope (Heine Optotechnik, Herrsching, Germany). The distance from the right mouth corner to the vocal cords (D2) was measured by noting the measurement on the ETT, opposite to the right mouth corner when the tip of the tube reached the vocal cords [8]. The newly devised ETT insertion depth (in cm) was determined by calculating D1 + D2 - 4 (The number 4 was chosen because 4 cm is regarded as the best ETT tip-carina distance) [5].

Kang's topographic intubation method. D1: the distance from the thyroid prominence to the center of the manubriosternal joint on the surface of the patient's chest. D2: the distance from the right mouth corner to the vocal cords (D2) measured by noting the measurement on the ETT opposite the right mouth corner when the tip of the tube reached the vocal cords.
Intubation was performed with the head and neck in a neutral position. Adult male patients were intubated with 7.5 mm internal diameter (ID) plain tubes (Covidien, Mansfield, USA), and 7.0 mm ID plain tubes were used in adult female patients. Following intubation, the ETT was positioned properly at the right mouth corner, with our method (Kang's method), and was secured to the upper lip. Neutral position was obtained by maintaining the patient flat on the operation table without head extension or neck flexion [9]. The tip-carina distance was measured on a printed scale in millimeters, attached to the fiberoptic bronchoscope (Olympus LF-GP, Olympus Optical Co., Tokyo, Japan) through a modified right-angle connector (Mallinckrodt Medical, Athlone, Ireland), which allowed a bronchoscopic examination during the manual ventilation [5]. No patient experienced oxygen desaturation. The following equation can be assumed to be right.
Airway length from right mouth corner to the carina with fiberoptic bronchoscope through the ETT = Evron's tip-carina distance + Evron's topographic length = our tip-carina distance + our ETT insertion depth
Therefore, the tip-carina distance of Evron et al.'s method could be determined by the calculation, shown below, without a second intubation.
Evron's tip-carina distance (cm) = our tip-carina distance (cm) + our ETT insertion depth (cm) - Evron's topographic length (cm)
The formula was so obvious that we did not measure, but calculated the Evron's tip-carina length, to avoid another unnecessary intubation and fiberoptic bronchoscopy.
A pilot study of 10 patients demonstrated the mean (SD) of 3.4 (1.2) cm for the Evron's tip-carina distance and 3.9 (0.8) cm for our tip-carina distance. A sample size of 44 was calculated for a Type I error (two-sided) of 0.05 and a power of 0.8. Therefore, 50 patients in each gender were enrolled to compensate for the possible dropouts.
Independent t-test or Fisher's exact test (SPSS for Windows version 15.0) was used for statistical analysis, comparing the characteristics between the genders. A paired t-test or McNemar's test (SPSS for Windows version 15.0) was performed for statistical analysis comparing the two methods. A P value of less than 0.05 was considered statistically significant.
Results
The details of the patients studied are provided in Table 1.
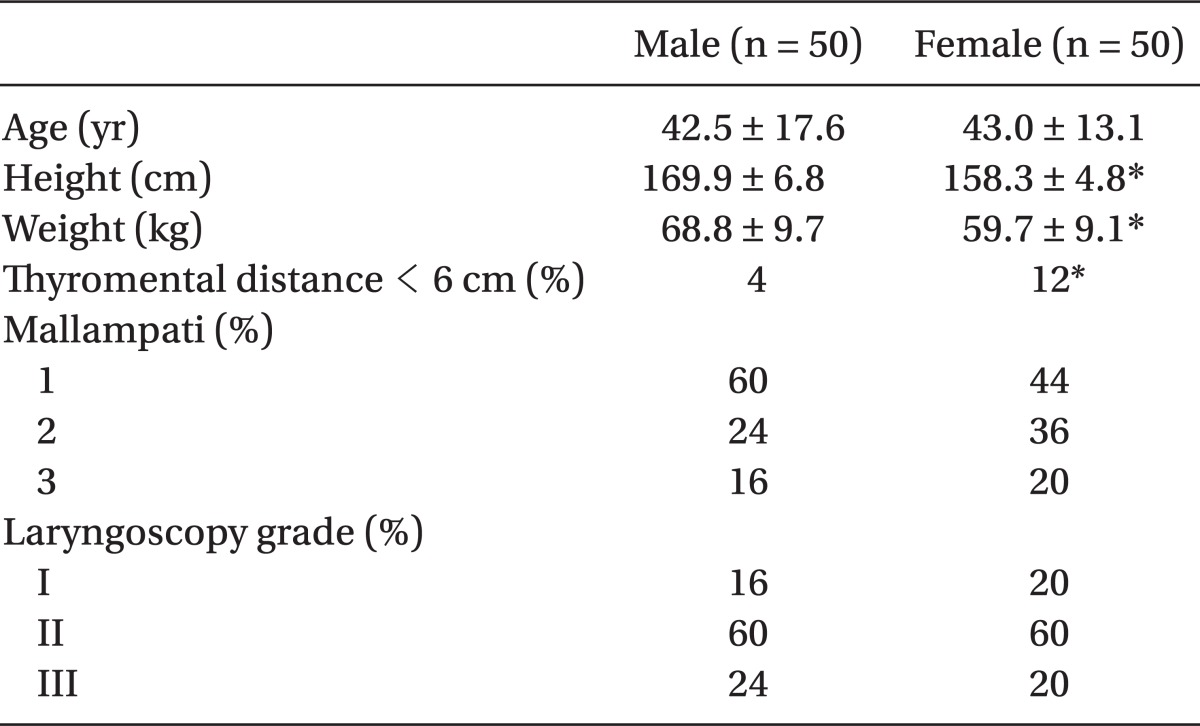
Baseline Characteristics of Patients
There were no statistical difference between the Evron's topographic airway length and our newly devised ETT insertion depth. The distances from the tip of the ETT to the carina were not significantly different between the methods of the same gender. However, our method allowed ETT tip placement between 3 cm and 5 cm above the carina more frequently than the Evron's method in males (Table 2). There were no endobronchial intubations in this study.

Comparisons of Variables between the Two Topographic Methods
Discussion
Our new topographical method allowed ETT tip placement at a safe distance above the carina, more frequently than that of the Evron's method in males.
Proper positioning of the ETT tip remains a matter of concern in anesthetic practice, emergency medicine and critical care medicine. There are many methods of estimating the optimal ETT length in orotracheally intubated patients, including auscultation of bilateral breath sounds, symmetric chest expansion, palpation of the ETT cuff in the suprasternal notch [10,11], using age, height, weight, foot length or an arbitrarily determined length [1,8,12,13], positioning of the ETT in relation to the vocal cords [12,14], use of chest radiograph or fiberoptic bronchoscopic examination [15], and topographic measurements [5,6]. However, these methods are not always evidence-based, cost-effective or appropriately individualized to the patient.
The angle of Louis can be easily palpated near the second rib insertion to the manubriosternal joint. The plane of division into the upper and lower mediastinum traverses the manubriosternal joint and the lower surface of the fourth thoracic vertebra, and the plane passes horizontally through the sternal angle, and also the bifurcation of the trachea [4,16].
Evron et al. [5] showed that their simple topographic measure allowed proper ETT tip placement more frequently, compared with that of the 21/23 cm method. Our results confirmed, once again, that the Evron's method is excellent. However, two measurement lines, drawn from the mouth angle to the jaw angle and from there to the midline of the sternal manubrium in Evron's method, appear somewhat arbitrary. We devised our new method based on the actual insertion course of the ETT into the airway.
Topographical methods can be difficult to apply in extremely obese patients. However, the manubriosternal joint can be identified by palpating the second rib or can be roughly measured as the junction of 1/4 and 3/4 of the total sternal length [17]. In women, the thyroid cartilage may not be prominent and palpation of the tracheal cartilage, starting at the sternal notch, may help identify the cricoid cartilage and then the thyroid prominence [18]. However, difficulty in palpation of the thyroid prominence seems to have caused failure in differentiating the two methods in women.
Our method can be simply adjusted in clinical situation like this: First, measure D1 (the distance from the thyroid prominence to the center of the manubriosternal joint) and subtract 4 from D1 and then memorize the value (D1 - 4) cm. Second, just when the tip of the ETT reaches the vocal cords during intubation, the tube is inserted through the glottis as long as (D1 - 4) cm.
In conclusion, this study demonstrated that our method allowed ETT tip placement at a proper distance, above the carina, more frequently than the Evron's method in males, even though the distances measured from the tip of the ETT to the carina were not significantly different between the methods in the same gender.