Pleural effusion due to intraoperative rupture of an infected renal cyst
Article information
Pleural effusion can occur after complicated renal cyst operations. Rupture of the cyst into the retroperitoneal space and diffusion of cyst content through diaphragmatic pores is an unusual cause of pleural effusion. Reports about pleural effusion after renal cyst operation are rare in the literature while the diaphragm is intact. Here we report a case of renal cyst operation complicated with intraoperative cyst rupture and ipsilateral pleural effusion postoperatively. The culture of the cyst and the pleural fluid showed the same organism: Klebsiella pneumonia.
A 57-year-old male patient was admitted to the emergency department. His complaints were right flank pain, high fever and poor health. Urosepsis was diagnosed after routine tests and the patient was referred to the urology department. In his history there was right nephrolithotomy due to kidney stones and stenting during angiography due to coronary heart disease.
After tests for diagnosis of multiple kidney stones, pyonephrosis and a renal cyst approximately 13 cm in size were identified in the non-functional right kidney. Before nephrectomy and cyst excision, a nephrostomy catheter was inserted into the right kidney with intravenous antibiotic therapy for the treatment of pyonephrosis.
After preoxygenation with 100% oxygen, anesthesia was induced with thiopental 400 mg and rocuronium 50 mg and maintained with sevoflurane 1.5% in N2O : O2 (50% : 50%). Endotracheal intubation was performed with an 8.0 mm inner diameter (ID) endotracheal tube.
The nephrectomy operation was started under laparoscopy, but later was converted to open surgery because of very adherent tissues. The kidney tissue and the cyst were totally removed, but in the 50th minute of the operation the cyst ruptured due to adhesions. After the rupture, the content of the cyst diffused to the retroperitoneal area, and the surgeon aspirated and irrigated the area many times. The operation continued for 40 minutes after the rupture of the cyst. The duration of anaesthesia was 100 minutes.
Hemodynamic parameters were stable throughout the operation. The patient was extubated at the end of the surgery but nearly 15 minutes after extubation the patient had difficulty in breathing and he was agitated. Blood gas analysis, which was taken 18 minutes after extubation, showed hypoxaemia; pH: 7.49; pO2: 54 mmHg; pCO2: 30 mmHg; HCO3: 23, SpO2: 88 (with an O2 mask). The patient was taken to the intensive care unit because of respiratory distress.
The patient was conscious in the ICU. But on auscultation the right lung sounds were decreased and a serious respiratory distress was present. Chest X-ray revealed a pleural effusion (Fig. 1). The patient's respiratory distress decreased after thoracentesis and chest tube insertion. Cultures of the pleural effusion and of cyst fluid taken during the operation were the same: Klebsiella pneumoniae. Imipenem 500 mg qid, linezolid 600 mg bid and metronidazole 500 mg tid were administered.
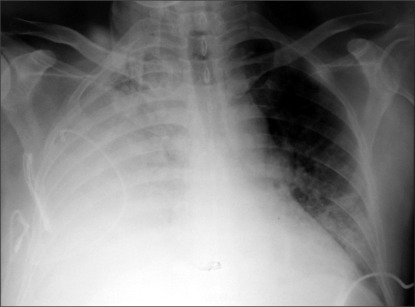
Pleural effusion was detected on the chest AP X-ray which was taken during respiratory distress.
The diaphragm was intact during surgery and there was no defect on CT. We thought that there was retroperitoneal fluid transition through the diaphragmatic pores during the operation. The patient's general condition improved with antibiotic therapy and drainage of the pleural fluid. The pathology report indicated chronic pyelonephritis. The patient was referred to the urology department 4 days after surgery, showing improvement in blood gas values, (pH: 7.35, pO2: 88 mmHg, pCO2: 36 mmHg, HCO3: 24, SpO2: 96), respiratory parameters and chest radiography. The chest tube was removed twelve days later and the patient was discharged as healthy.
Pleural effusion may occur for a wide variety of reasons. Commonly, it can be a reactive response to infections, malignancies and heart failure. Pseudochylothorax and urinothorax are uncommon causes of pleural effusion. Also chylothorax is a rare cause of pleural effusion and occurs as a leakage of thoracic duct lymph [1]. Pseudochylothorax is a clinical condition characterized by asymptomatic and usually unilateral pleural effusion. In one case report, bilateral pleural effusion was reported after a percutaneous nephrolithotomy operation [2].
Urinothorax is the other rare cause of pleural effusion; it is detection of the urine in the pleura. Urinothorax occurs when there is diffusion of urine through the pleura due to extravasation of a urinoma and urinary tract obstruction [3]. In our patient, none of the above was the cause of his pleural effusion. The cause was cyst fluid transition through the diaphragmatic pores after rupture of the cyst.
Complications due to infection or renal hydatid cyst rupture have been reported before [4] and there are many cases of intraperitoneal and retroperitoneal renal cyst rupture. But there are only a few reports of cyst rupture causing pleural effusion.
A post-traumatic renal cyst rupture can drain to the peritoneal cavity, retroperitoneum, pelvicalyceal system, and perinephric and subcapsular areas [5]. In our case, the fluid diffused through the diaphragmatic pores during the operation.
In conclusion the anesthesia team should always be careful about pulmonary complications during perioperative periods of renal cyst surgery.