Introduction
The bispectral index scale (BIS) and spectral entropy are commonly used to evaluate the depth of hypnosis. They are all electroencephalographic (EEG)-derived indices. BIS is composed of EEG parameters that integrates several disparate descriptors of the EEG into a single variable and is the most commonly used scale to judge and control hypnotic levels during general anesthesia and sedation [1]. On the other hand, spectral entropy reflects raw EEG and frontal electromyography (FEMG) data, resulting in two values, namely response entropy (RE) and state entropy (SE). SE, which is calculated over frequencies ranging from 0.8 to 37 Hz, is the entropy of the EEG signal reflecting the patient's cortical activity. RE includes additional higher frequencies up to 47 Hz, reflecting both EEG and FEMG activity.
Both BIS and spectral entropy may be influenced by several factors. Drugs and surgical stimulation can change values of BIS and spectral entropy [2,3]. Some reports showed that electromyography (EMG) activity has an effect on BIS and spectral entropy [4]. BIS and spectral entropy is calculated over frequencies that include EEG and EMG, so EMG activity may change values of BIS and spectral entropy.
Etomidate maintains cardiovascular stability during induction of general anesthesia, so it can be used relatively safely in patients with compromised myocardial contractility. But, it often causes myoclonus to affect EMG [5,6]. Accordingly, author hypothesized that EMG activity after etomidate injection would affect interpretation of hypnotic levels as determined by BIS and spectral entropy. This study was performed to compare the effect of etomidate on BIS, RE and SE during induction of anesthesia.
Materials and Methods
After approval from the regional hospital ethics committee and informed consent, authors studied 50 patients, American Society of Anesthesiologists class I-II, 20-69 years of age, undergoing elective surgery. Exclusion criteria included disease or injury affecting the central nervous system, recent use of psychoactive or analgesic medication, neurological disorders, alcohol, or drug abuse, and body weight below 70% or above 130% of the patient's ideal body weight.
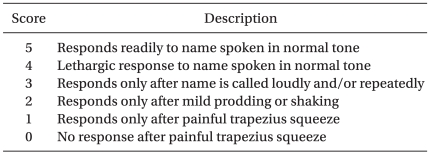
Patients arrived at the operating room after an overnight fast. Glycopyrrolate (0.2 mg) was given intramuscularly 1 hour before surgery as premedication. They were monitored with electrocardiography, pulse oximetry, end tidal carbon dioxide and non invasive blood pressure measurements. BIS was monitored with the A-3000 BIS monitor (Aspect Medicine system Inc., Norwood, USA). RE and SE were monitored with a Datex-Ohmeda Aestiva/5 Entropy Module (E-EntropyŌäó, GE Healthcare, Helsinki, Finland). Mean arterial pressure (MAP), heart rate (HR), Modified Observer's Assessment of Alertness/Sedation scale (MOAA/S) (Table 1), BIS, RE and SE were recorded every 5 min.
Anesthesia was induced with etomidate (0.3 mg/kg), then rocuronium (0.6 mg/kg) was injected in patients after loss of eyelash reflex and patients inhaled 100% oxygen. Ninety seconds after rocuronium injection, the patients inhaled 4 vol% sevoflurane and 100% oxygen, and then they were intubated.
BIS, RE, SE and MOAA/S were measured 4 times (before injecting etomidate [T0], after the loss of eyelash reflex [T1], 90 seconds after rocuronium injection [T2], and after intubation [T3]). In addition, authors checked whether myoclonus occurred during the induction period of anesthesia.
Data were expressed as means ┬▒ standard deviation (SD) and analyzed using a two-way mixed-designed analysis of variance (ANOVA) and Tukey's post hoc test for comparisons. Differences in BIS, RE, SE, MAP, and HR between group with myoclonus and group without myclonus were analyzed with two-way analysis of variance followed by paired t-test. The number of patients is indicated by n. Probability values of (P) < 0.05 were considered statistically significant. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) version 12.0 (SPSS Inc, Chicago, IL, USA).
Results
A total of 50 patients were included. Mean age, weight, height, MAP and HR were 37.4 ┬▒ 11.4 yrs (range 19-61), 64.0 ┬▒ 12.4 kg (range 47.0-110.0), 165.6 ┬▒ 9.0 cm (range 146.0-186.0), 98.0 ┬▒ 13.9 mmHg (range 73-132) and 76.8 ┬▒ 18.1 beats/min (range 50-119), respectively. Twenty-one patients (42%) were males and 29 were females (58%).
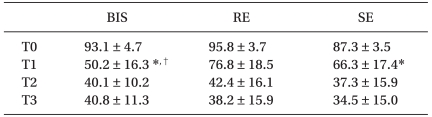
BIS, RE and SE values at baseline (T0) and the values after injection of etomidate (T1, T2, T3) are summarized in Table 2. Compared with T0, the T1 values for BIS 50.2 ┬▒ 16.3, RE 76.8 ┬▒ 18.5, and SE 66.3 ┬▒ 17.4 decreased (P < 0.05). There were no significant differences among BIS, RE and SE at T2 and T3. All MOAA/S scale at T1, T2, and T3 were below 2.
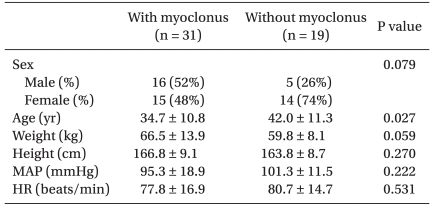
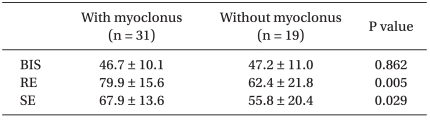
Among a total 50 patients, 31 patients had myoclonus. There were no statistically significant differences in the gender, weight, height, MAP and HR between patients with or without myoclonus (Table 3). On the other hand, younger age was significantly associated with myoclonus (Table 3). RE and SE values in the myoclonus group were significantly higher than those without myoclonus at T1, but BIS was similar, whether myoclonus occurred or not (Table 4).
Discussion
The main finding of this study was that BIS was lower than RE and SE at the point of immediate loss of consciousness after etomidate injection. BIS score was under 60 regardless of myoclonus at loss of eyelash reflex, whereas RE and SE were over 60. Moreover, RE and SE in patients with myoclonus were higher than those of patients without myoclonus, but BIS was not different.
Etomidate is often used for inducing anesthesia in patients who have limited hemodynamic reserve. But, it has several disadvantages like dose-dependent adrenocortical suppression, possible inhibition of platelet function, and involuntary skeletal muscle contractions (myoclonus). Involuntary skeletal movement characterized as myoclonus occurred more than 50% of patients receiving etomidate [7], and when myoclonus occurs, EMG readings may change. EMG activity may influence BIS and spectral entropy [4], by interrupting the interpretation of hypnotic levels after etomidate injection.
According to this study, RE and SE did not decrease the same as BIS at loss of consciousness during induction of anesthesia with etomidate. Values were 50.2 ┬▒ 16.3 (BIS), 76.8 ┬▒ 18.5 (RE), 66.3 ┬▒ 17.4 (SE) at T1. Among them, RE and SE values were over 60 at T1, which are regarded as inappropriate hypnotic levels for intubation. It is thought that RE and SE values of patients with myoclonus increased their mean values, compared with BIS. The appropriate hypnotic level for intubation is known to be below 60 for BIS or spectral entropy, in general [8].
Spectral entropy consists of RE and SE. RE is calculated over frequencies in the range 0.8-47 Hz including EMG, where frequencies in the range 32-47 reflect EMG; therefore, RE is dominantly influenced by EMG. SE, which is calculated over frequencies ranging from 0.8 to 37 Hz, is the entropy of the EEG signal. In this frequency range, most EMG activity is eliminated and SE commonly is not affected. But sometimes EMG can affect SE, because the power spectrum of EMG overlaps that of EEG, and strong EMG impact may change the spectrum at 20 Hz [9].
The BIS calculates three sub parameters including the burst suppression ratio, the beta ratio and SynchFastSlow. The burst suppression ratio is the proportion of the suppressed EEG (isoelectric) in an epoch, the beta ratio is the log ratio of the power in two empirically derived frequency bands (high- and medium-frequency ranges), and SynchFastSlow is the relative bispectral power in the 40-47 Hz frequency band [10]. The bispectral analysis examines the relationship between the sinusoids at two primary frequencies, f1 and f2, and a modulation component of the frequency f1 + f2.
Bruhn et al. [4] reported two cases of BIS increase by EMG activity in anesthetized patients. Another case where BIS increased by myoclonus during etomidate injection was also reported [11]. It is supposed that calculation of BIS requires inclusion of frequencies above 40 Hz, and approaching frequencies generated by muscle activity on EMG, such as SynchFastSlow.
In some studies, noxious pain like tracheal intubation increases spectral entropy, especially RE rather than BIS [12,13], since noxious pain is relevant to increases EMG activity [14]. By comparison, we investigated BIS, RE and SE values during induction of anesthesia, and not in anesthetized patients. In this case, BIS decreased significantly rather than entropy when the level of consciousness is decreased. When myoclonus occurred, differences between BIS and spectral entropy were larger and RE had the largest difference among BIS, SE and RE. It seems that BIS may be interfered by EMG less than entropy and mainly influenced by EEG. Further studies are needed to determine the mechanism that etomidate influences BIS and spectral entropy.
In the present study, the occurrence of myoclonus after etomidate injection was 62% in patients, and it was not significantly related to sex, weight, height and vital signs, whereas the mean age of patients who expressed myoclonus was younger than those who did not. The authors propose that younger patients may have more muscle mass, which might affect to the occurrence of myoclonus. It is necessary for additional studies investigating the association between age and myoclonus.
In this study, there was no significant difference between BIS, RE and SE after injection of the muscle relaxant. Muscle relaxants suppress muscle movement, so it may affect data like EMG activity. Several studies reported that muscle relaxants decrease BIS, RE and SE [15,16]. As a result, hypnotic levels may be misinterpreted by EMG activity [9,17]. The mechanisms of etomidate induced myoclonus are not clarified yet. Myoclonus has features like tonic-clonic seizures, as muscle movements generally increase [6]. When myoclonus occurred, RE and SE values were higher than those without myoclonus at T1, but BIS was rarely influenced by existence of myoclonus. It is presumed that RE and SE were strongly influenced by EMG activity.
Finally, when myoclonus occurred, RE and SE did not decrease similarly to BIS at the level of loss of consciousness during induction of anesthesia with etomidate. Therefore, BIS may reflect hypnotic levels better than spectral entropy in patients with myoclonus during induction of anesthesia with etomidate.