Introduction
Anesthetic awareness can cause perioperative pain and discomfort, as well as temporary after-effects, such as postoperative anxiety, sleep disorder, nightmares, and recall. In some cases, it can cause post-traumatic stress disorder. Therefore, the anesthesiologist has to carefully maintain anesthetic depth.
Anesthetic depth is judged from observing vital signs and can be adjusted by the dose of administered anesthetics, depending on the patient's vital signs. Monitoring anesthetic depth makes it possible to administer the appropriate dose of anesthetics and prevent anesthetic awareness, side-effects of over-dose, and economic and environmental waste. Therefore, anesthetic management, using proper anesthetic administration, is equally important as maintaining the patient's vital signs.
Entropy monitoring allows for the quantification of cerebral neural activity. The increase and decrease in entropy scores are related to the level of consciousness under anesthesia. EEG-entropy is an entropy monitor based on EEG analysis used in measuring hypnosis levels [1]. EEG-entropy has two signals: State entropy (SE) receives information from the brain waves; response entropy (RE) incorporates information from the frontal eletromyography. SE is computed using EEG data from the previous 15 s, between 0.8-32 Hz, and shows the value in the range of 0-91. RE is computed from 32-47 Hz with 1.92 s, and reflects fast muscular activity from the frontal muscle, and shows the value in the range of 0-100. Similar to BIS, 100 signifies awake; 60, clinically significant anesthetic state; 40, low possibility of consciousness; and 0, suppression of cortical activity [2].
The authors maintained the appropriate anesthetic depth for patients undergoing entropy-monitored gynecological surgery and controlled anesthetic depth by titrating the concentration of the inhaled anesthetic - sevoflurane. In this study, the authors attempted to compare the ET sevoflurane concentration (ET) when using continuous infusion of sevoflurane alone, against ET when using remifentanil as a supplement to sevoflurane, to determine the difference in administered doses of sevoflurane.
Materials and Methods
Upon receiving the approval of the hospital ethics committee and the consent of the patients after they were informed about the study during preanesthetic visitation, we performed the study on 40 patients of ASA class I & II, electing for gynecological surgery under general anesthesia.
Patients were excluded if they had a neurologic or psychiatric disease, past history of cardiovascular disease, or if they had consumed sedatives, antidepressants, anticonvulsants, or opioids. Also, patients were excluded if intubation was expected to be difficult or had been difficult in the past.
The patients were randomly divided into two groups that were infused with remifentanil (Group R) or normal saline (Group S). Normal saline (40 ml) and remifentanil (40 ml) diluted with normal saline (50 ┬Ąg/ml) were prepared in continuous infusors. The anesthesiologist was blinded for the study and no patient was given premedication. Upon arrival onto the operating table, electrocardiography, non-invasive blood pressure, and pulse oxymetry were attached for monitoring. The entropy sensor was attached to the patient's forehead (Entropy Sensor, Disposable, GE Healthcare, Helsinki, Finland), connecting the patient to the entropy monitor (S/5 Entropy Module, Datex-Ohmeda, Madison, WI, USA).
Anesthesia was induced using thiopental sodium (5 mg/kg) in both groups. After loss of consciousness, rocuronium (1.0 mg/kg) was administered, and manual mask ventilation was performed using 4 vol% sevoflurane. After sufficient muscle relaxation, before intubation, IV remifentanil (1.0 ┬Ąg/kg) was slowly administered for 1 min in both groups. Following intubation, O2-N2O-sevoflurane was used for the maintenance of anesthesia. In the two groups, either the prepared normal saline or remifentanil was administered with the continuous infusor at the rate of 0.002 ml/kg/min, 2 vol% sevoflurane was inhaled, and the SE value was maintained between 40-60 by titrating 0.5 vol% sevoflurane every 5 minutes. Despite controlling the concentration of sevoflurane to maintain SE value, when the hemodynamics could not be stabilized, cardiovascular drugs were used and recorded afterwards. The surgery proceeded, and when skin suturing (SS) was started, the continuous infusion of either saline solution or remifentanil and the administration of sevoflurane were stopped and the patient was ventilated with 100% O2. After the surgery, muscle relaxation was reversed.
The systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), RE, SE, and end-tidal sevoflurane concentration (ET) measurements were recorded by a blinded medical resident immediately after intubation, at 5 min intervals over a 25 min period, at the beginning of SS and at the end of surgery. The measurements of the two groups were compared. The mean ET scores taken every 5 min immediately after intubation until the end of surgery were averaged and analyzed for the purpose of comparing sevoflurane.
All statistical analyses were performed on SPSS (version 18.0, SPSS Inc., IL, USA). The values were expressed as mean ┬▒ SD. To test homogeneity, age height, weight and the administration time of sevoflurane were analyzed using an independent t-test and ASA classes using a chi-square test. The comparison of the mean ET measured from post-intubation until the end of the surgery for the two groups was analyzed using an independent t-test. ET, RE, SE, SBP, DBP, and HR values were analyzed using a repeated measure one-way ANOVA. When time affected a line, a contrast test was performed on the values taken 5 min post-intubation to the end of surgery. The analysis of each period was done using an independent t-test; P < 0.05 was considered statistically significant.
Results
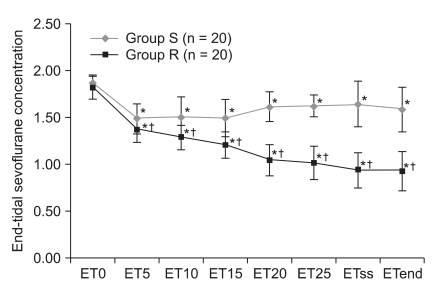
The demographic data analysis showed no statistical differences in the patient age, weight, or height (Table 1). The two groups showed significant differences in ET (Fig. 1) (P < 0.05). During time periods from 5 min post-intubation to the end of surgery, ET values were significantly lower in Group R compared to Group S (Fig. 1) (P < 0.05). Perioperative mean ET in Group S (1.63 ┬▒ 0.15) was significantly lower than in Group R (1.11 ┬▒ 0.10) (P < 0.05).
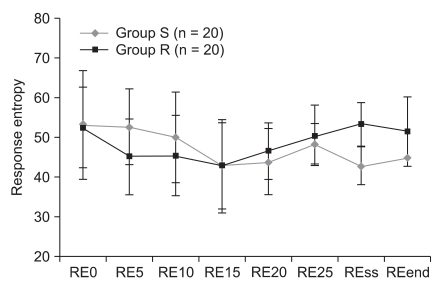
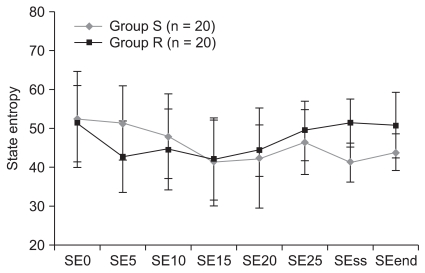
RE and SE were maintained in both groups between 40-60, and there were no significant differences amongs subjects in both groups (Fig. 2 and 3) (P > 0.05).
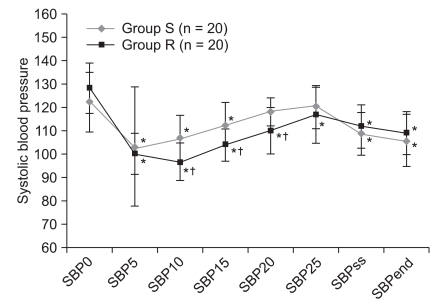
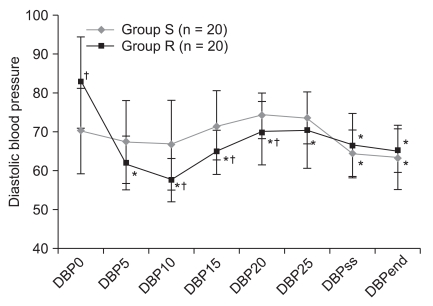
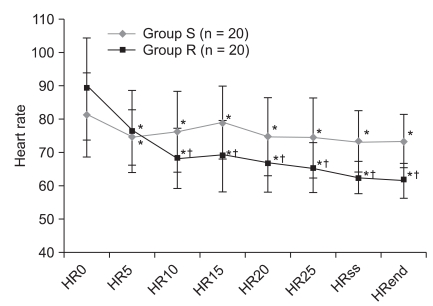
The SBP and DBP were not significantly different and they were similar with the progress of time (P > 0.05). Comparing intervals, Group R compared to Group S had low SBP and DBP 10 min and 15 min post-intubation, but there were no differences afterwards (Fig. 4 and 5). HR values were significantly different (P < 0.05). Although Group R, compared to Group S, had lower HR values from 10 min post-intubation (Fig. 6) (P < 0.05), this was clinically insignificant. Neither group required drug administration for intra-operative hemodynamic stabilization.
Discussion
In general anesthesia, correctly judging and maintaining anesthetic depth is very important. Judging the depth of anesthesia from observing patient cardiovascular response and then titrating the dose of anesthetics is common, but with the introduction of EEG-entropy, one can monitor the depth of anesthesia and the hypnosis level, and it measures anesthetic depth similar to BIS in anesthesia using propofol or sevoflurane [1-4].
Vakkuri et al. [2] stated that in sevoflurane-anesthesia, the appropriate depth of anesthesia has the entropy value of 40-60. In the current study, sevoflurane concentration was adjusted so the entropy value could be maintained between 40-60. Comparisons of RE and SE between the two groups showed no significant differences, and they followed similar changes with time.
Remifentanil is an opioid, with a rapid onset of effect and a short duration that selectively affects the ┬Ą-receptor [5]. Because of its pharmacokinetic characteristics, it is commonly used as a supplement in general anesthesia performed with inhaled or intravenous anesthetics [6]. However, it has side-effects such as hypotension, postoperative nausea and vomiting (PONV), respiratory depression, and increased postoperative pain. O'Hare et al. [7] stated that a bolus infusion of remifentanil (1 ┬Ąg/kg) can control the balance of hemodynamic response at the time of intubation and reduce the risk of post-intubation hypotension. Lee et al. [8] stated that a bolus infusion of remifentanil (1.0 or 2.0 ┬Ąg/kg) effectively suppresses the increase in post-intubation mean arterial blood pressure (MAP) and HR. A remifentanil dose of 2.0 ┬Ąg/kg can permit hypotension to persist, so 1.0 ┬Ąg/kg is considered the more appropriate dose. Song and White [9] stated that in desflurane-anesthesia, a low supplementary dose of remifentanil (0.07 ┬Ąg/kg/min) can effectively control the autonomic nervous system response to nociceptive stimulation during laparoscopic surgery, and allows for fast awakening without postoperative side-effects. Song et al. [10] compared the usage to the non-usage of remifentanil (0.05-0.2 ┬Ąg/kg/min) in patients under sevoflurane-anesthesia for a laparoscopic cholecystectomy and found that the patient awakening and extubation times were shorter without raising PONV rates and without the extra use of antiemetics or analgesics.
Lee et al. [11] also similarly found that patients undergoing laparoscopic cholecystectomy, who were anesthetized with sevoflurane with the continuous infusion of remifentanil (0.1 ┬Ąg/kg/min), did not have higher rates of PONV, pain, or a greater use of analgesics. Calder├│n et al. [12] found that when either remifentanil (0.05 ┬Ąg/kg/min or 0.1 ┬Ąg/kg/min) was continuously infused in patients undergoing elective abdominal and thoracic surgery, postoperative pain was effectively managed in both groups, without side-effects such as respiratory depression or PONV. Also, the group continuously infused with remifentanil (0.1 ┬Ąg/kg/min) required less additional analgesics. Therefore, the current study sought to stabilize hemodynamic response to intubation while reducing the risk of post-intubation hypotension by slowly infusing IV remifentanil (1.0 ┬Ąg/kg) for 1 min. To effectively control post-intubation perioperative autonomic nervous system response and to allow for faster awakening without side-effects, a low dose of remifentanil (0.1 ┬Ąg/kg/min) was continuously infused. The vital signs were then measured, and showed that they were lower for Group R than Group S. Neither group required drugs to safely maintain hemodynamics.
G├│mez de Segura et al. [13] found through a rat experiment, that the continuous infusion of remifentanil in rats under sevoflurane-anesthesia decreased sevoflurane MAC proportionally to the dose of remifentanil. Manyam et al. [14] found that remifentanil decreased the required dose of sevoflurane when they performed anesthesia using TCI of sevoflurane (0.3-6 vol%) and the effect-site concentration of remifentanil was 0.5-15 ng/ml. Pavlin et al. [15] used a BIS monitor to titrate the dose of sevoflurane and found that ET was reduced by 13%. Aim├® et al. [16] found that in sevoflurane-anesthesia using either BIS or an entropy monitor to titrate the administered dose of anesthetics, both monitoring methods equally reduced the administered dose of sevoflurane by 29%.
Therefore, the current study used an entropy monitored titration of sevoflurane and the continuous infusion of remifentanil to determine if the administered dose of sevoflurane could be reduced, and the results were significantly different. Compared to Group S, Group R had significantly lower ET, and significantly lower mean ET when measured during surgery. When sevoflurane alone is used in anesthesia, compared to when remifentanil is used as a supplement, it is believed that a greater dose of sevoflurane is unnecessary.
Many factors affect the patient's recovery from anesthesia, and the level of the residual anesthetic can be a factor. Also, if an individual's methabolism rate of the drug is consistent, the determinant factor is the administered dose of the anesthetic. Recart et al. [17] studied 90 patients to determine the effect of desflurane dose on the recovery time. Patients who were administered low doses of desflurane, from titrating to the auditory evoked potential or BIS monitor, had shorter extubation times and shorter lengths of PACU stay. Thus, the dose of anesthetics was found to directly affect recovery rates. Also, many studies have found that compared to the single use of sevoflurane, the combined use of remifentanil and sevoflurane reduces the required dose of sevoflurane and allows for faster patient recovery [18,19]. Although the current study did not measure the extubation or recovery times, the authors found that the continuous infusion of remifentanil proved to reduce the necessary dose of sevoflurane, and may also help in the recovery from anesthesia.
The current study monitored the depth of anesthesia when sevoflurane alone and when sevoflurane plus a low dose of remifentanil (0.1 ┬Ąg/kg/min) were administered; and the authors found that with the combined use of remifentanil, low doses of sevoflurane can also maintain anesthetic depth. The intra-operative mean ET was reduced approximately 32%. In the combined use of sevoflurane and remifentanil, the authors kept the dose concentration consistently at 0.1 ┬Ąg/kg/min, but titrating remifentanil's concentration to hemodynamic changes may also be helpful.
In conclusion, in entropy monitoring of anesthetic depth, administering a low dose of remifentanil (0.1 ┬Ąg/kg/min) as a supplement to inhaled anesthetics, will allow for a decreased dose of inhaled anesthetics, compared to when inhaled anesthetics are used alone. This will prevent the delay in recovery resulting from overdose and circumvent economic and environmental waste. Even without the entropy-monitoring of anesthetic depth, the combined use of sevoflurane and remifentanil can reduce the inhaled dose of sevoflurane, without perioperative awareness.