Prevention of pain with the injection of microemulsion propofol: a comparison of a combination of lidocaine and ketamine with lidocaine or ketamine alone
Article information
Abstract
Background
Aquafol, a microemulsion propofol, causes more severe and frequent pain on injection than propofol. The purpose of this study was to compare a combination of lidocaine and ketamine on aquafol-induced pain with lidocaine or ketamine alone during the induction of anesthesia.
Methods
In this prospective, randomized, double-blinded study, 130 healthy patients who were undergoing elective surgery under general anesthesia were enrolled. The patients received IV lidocaine 40 mg plus ketamine 25 mg (Group LK, n = 43), lidocaine 40 mg (Group L, n = 42), or ketamine 25 mg (Group K, n = 45) with a rubber tourniquet on the forearm 1 min before the injection of microemulsion propofol. The pain score was assessed by a 4-point verbal rating scale (VRS) at 10 seconds after injection of microemulsion propofol 30 mg and during the injection of the remaining total dose.
Results
The incidence and severity of pain was significantly lower in Group LK than Group L or Group K at 10 seconds after the injection of microemulsion propofol 30 mg (P < 0.05). And the incidence and severity of pain was significantly lower in Group LK and Group K than Group L during the injection of the remaining total dose (P < 0.05).
Conclusions
Pretreatment with IV lidocaine 40 mg plus ketamine 25 mg with a rubber tourniquet on the forearm 1 min before the injection of microemulsion propofol is more effective than lidocaine 40 mg or ketamine 25 mg alone in preventing pain from the injection of microemulsion propofol.
Introduction
Propofol is commonly used in the induction and maintenance of general anesthesia owing to its rapid onset and short duration of action, but propofol causes pain on injection. One method to reduce this pain is pretreatment with lidocaine 40 mg given with a tourniquet 30 sec to 120 sec before the injection of propofol [1]. However, even this method cannot completely prevent injection pain. Another method is the pretreatment with lidocaine together with remifentanil, alfentanil, or ketamine [2-4]. Fujii and Nakayama [4] stated that pretreatment with a combined infusion of lidocaine and ketamine is more effective in reducing pain on injection than lidocaine alone.
Lipid emulsion propofol causes severe lipid solvent-related adverse effects, such as hypertriglyceridemia, pulmonary fat embolism, pancreatitis, propofol infusion syndrome, and drug contamination. To eliminate these problems, a hydrosoluble lipid-free microemulsion propofol (Aquafol®, Daewon Pharmaceutical Co., Ltd, Seoul, Korea) was introduced to clinical practice in 2009. Although the new drug is safer, its pain on IV injection is much greater, so its greatest drawback in clinical practice is that it cannot be used alone [5,6]. The clinical history of microemulsion propofol is relatively short, with little data on how to reduce pain on injection. Therefore, we tested whether pretreatment with lidocaine and ketamine, which can prevent pain on injection of lipid-emulsion propofol, also prevents the pain on IV injection of microemulsion propofol.
We measured the pain after IV injection of microemulsion propofol with pretreatment with a single administration of either lidocaine 40 mg or ketamine 25 mg, or the combined administration of lidocaine 40 mg and ketamine 25 mg, to find the most effective method for preventing injection pain.
Materials and Methods
After obtaining the approval of the ethics committee and informed consent from patients, 130 ASA class I and II patients, 18-70 years of age, undergoing elective surgery under general anesthesia were enrolled. Patients were excluded if they showed neurological disorders, a negative effect in communication, or hypersensitivity towards these drugs.
The patients were randomly placed into 3 groups. Before microemulsion propofol (Aquafol®, Daewon Pharmaceutical Co., Ltd, Seoul, Korea) was administered, Group L was pretreated with lidocaine 40 mg (n = 42), Group K was pretreated with ketamine 25 mg (n = 45), and Group LK was pretreated with a combination of lidocaine 40 mg and ketamine 25 mg (n = 43). The patients were premedicated with IM midazolam 3 mg and glycopyrrolate 0.2 mg 30 minutes prior to surgery. Upon arrival in the operating room, the blood pressure, EKG, and oxygen saturation were monitored. An 18 G angio-catheter was placed in a large vein of the lower arm for the IV line. Before anesthetic induction, the blood pressure and heart rate were measured to find the baseline value. With a rubber tourniquet, the veins were occluded, and lidocaine and/or ketamine was administered, 1 min later, the tourniquet was released and IV microemulsion propofol 30 mg was administered; 10 sec later, a 4-point verbal rating scale (VRS) was used to measure the pain on injection. Then the remainder of the total dose of microemulsion propofol was administered (2 mg/kg-30 mg), and the VRS was again measured. The nurse mixed all the pretreated drugs with normal saline so that they would be identically 3 ml, and the measurement of VRS scores was assessed by a blinded researcher who did not know which drugs were administered. When the patient fell asleep, anesthesia was induced with sevoflurane in oxygen and rocuronium (0.6 mg/kg) and intubated. Anesthesia was maintained with sevoflurane during the surgery.
The VRS of the pain on injection of microemulsion propofol consisted of the evaluation of facial expression, withdrawal of the hand, tears, and pain compliants. 'None' was defined as no pain experienced. 'Mild pain' described patients who responded to feeling pain when questioned but had no facial grimacing and did not cry. 'Moderate pain' was when the patients had facial grimacing, withdrawal of the hand, and responded positively to feeling pain or complained of pain spontaneously. 'Severe pain' was when the patient voluntarily complained of pain, had facial grimacing, and withdrawal of hand (Table 1).
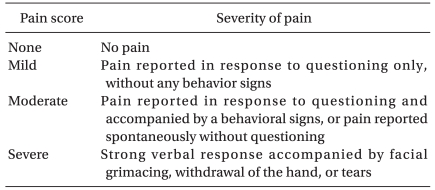
Assessment of Pain Scores of 4-point Verbal Rating Scale (VRS) during Injection of Microemulsion Propofol
Based on the bibliography references [5], the incidence rate of moderate to severe pain on the injection of microemulsion propofol was hypothesized to be 82%. After administering the tested drug, a reduction of moderate to severe pain on injection by 40% was considered clinically significant. Using α = 0.05 with a power 90%, the minimum sample size was predetermined as 40 patients per group. Statistical analysis was performed on SPSS (version 12.0, SPSS Inc., Chicago, IL, USA). The age, weight, and height of the groups were compared using one way ANOVA with a post-hoc Bonferroni's test. Gender and the 4-point VRS were analyzed using the chi-square test. P < 0.05 was considered statistically significant.
Results
After assessing the pain incidence and severity after the injection of microemulsion propofol 30 mg, 4 patients in Group K and 4 patients in Group LK fell asleep before receiving the remaining total dose of microemulsion propofol, making it impossible to assess their pain. They were excluded from the study, leaving 122 patients in the study. There was no significant difference between the groups in age, gender, weight, and height (Table 2).
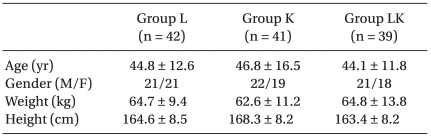
Demographic Data
After the IV administration of microemulsion propofol 30 mg, no pain was experienced by 32 patients in Group LK, but only 16 in Group L, and 19 in Group K. The incidence of moderate to severe pain was significantly lower in Group LK than Group L and Group K, with only 1 patient in Group LK, 7 in Group L, and 12 in Group K (P < 0.05) (Table 3). When the remaining dose of microemulsion propofol was administered, there were 28 patients in LK who experienced no pain; there were 10 patients in Group L; and 21 patients in Group K. Of moderate to severe pain, Group LK (N = 3) and Group K (N = 10) had significantly fewer patients than Group L (N = 22) (P < 0.05). There was no significant difference between Group LK and Group K (P > 0.05) (Table 4).
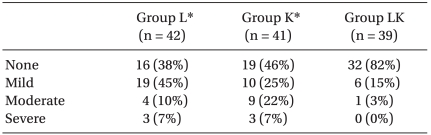
4-point Verbal Rating Scale (VRS) for Pain at 10 seconds after Injection of Microemulsion Propofol 30 mg
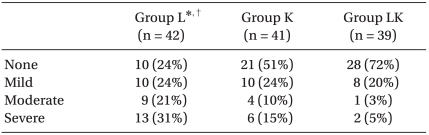
4-point Verbal Rating Scale (VRS) for Pain during the Injection of Remaining Microemulsion Propofol
Discussion
After venous occlusion using a tourniquet 1 minute before microemulsion propofol, the combined pretreatment of lidocaine and ketamine prevented propofol-induced pain better than either alone. Pain on injection is the most common side effect of lipid emulsion propofol, with an incidence of 70% to 92% in adults, and may be severe [1,7]. In pediatric patients, it can occur in 100% of the cases [2]. Pain on injection can decrease when the vessel being injected into has a large diameter, when the infusion speed is increased, and when drugs are at 4℃. Pretreatment with lidocaine, ketamine, metoclopramide, alfentanil, and remifentanil reduce pain incidence and severity [2-4, 8-10].
Microemulsion propofol is safer because it removes the severe side-effects of lipid emulsion propofol, but pain severity is worse and it cannot be used alone [5,6]. Jung et al. [5] found that moderate to severe pain on injection after aquafol administration (microemulsion propofol) was 81.9%, and was 29.2% after diprivan 30 mg (lipid emulsion propofol). The median VAS score for microemulsion propofol (72.0) was 6 times as great as for lipid emulsion propofol (11.5). Microemulsion propofol may cause pain because it has an aqueous free propofol concentration that is 7 times as great as in lipid-emulsion propofol [6,11]. Pain may occur when aqueous free propofol directly stimulates the free nerve endings or nociceptive receptors of the myelinated A delta fibers [5,6,12]. Lidocaine can prevent pain on propofol injection. Lidocaine is not only effective as a local anesthetic effects on the vein but also as a stabilizer for the kinin cascade [10]. King et al. [13] mixed 5, 10, and 20 mg of lidocaine with lipid emulsion propofol and found that a greater dose reduces pain on injection. Jonson et al. [9] stated that lidocaine 40 mg is more effective than 20 mg in reducing pain on injection from lipid emulsion propofol. The use of a tourniquet isolates the arm veins from the rest of the circulatory system and presents a useful model for studying the peripheral actions of a drug in the absence of a central effect [14]. Mangar and Holak [15] found that when lipid emulsion propofol is IV administered, pretreatment with lidocaine after a tourniquet is inflated to 50 mmHg is more effective than not using a tourniquet. Picard and Tramèr [1] did a meta-analysis of 56 research papers and found the best way to prevent injecting pain from lipid emulsion propofol was first by venous occlusion by a rubber tourniquet, pretreating with lidocaine 40 mg, releasing the tourniquet 30-120 sec afterwards, and then administering lipid emulsion propofol. Therefore, we followed the method suggested by Picard and Tramèr [1]: we placed a rubber tourniquet, pretreated with either lidocaine (40 mg) or ketamine or both, released the tourniquet 1 min later, and then administered microemulsion propofol.
Ketamine is an N-methyl-D-aspartate (NMDA) receptor antagonist and has a strong analgesic effect even at small doses. It effectively reduces pain on injection from lipid emulsion propofol, potentially via 1) central or peripheral analgesic action of the NMDA receptor block or 2) afferent pain pathway block by the peripheral local anesthesia action [16,17]. Bano et al. [18] believed that using a rubber tourniquet and pretreating with ketamine 0.5 mg/kg 1 minute before lipid emulsion propofol administration reduced pain on injection without causing hemodynamic changes. Therefore we chose ketamine 25 mg because it is close to 0.5 mg/kg. Fujii and Nakayama [4] found that the pretreatment of a mixture of lidocaine and ketamine significantly reduced pain on injection from lipid emulsion propofol more than pretreating with lidocaine alone.
The incidence of moderate to severe pain after administering microemulsion propofol 30 mg was 17% for Group L, 29% in Group K, and 3% in Group LK, lower than the 82% of moderate to severe pain on injection in the study by Jung et al. [5]. Lidocaine, ketamine, or the combination, therefore reduce pain on injection from microemulsion propofol as for lipid emulsion propofol. Some patients experienced no pain: 38% in Group L, 46% in Group K, and 82% in Group LK, indicating that the combination is more effective than either alone.
In the most studies, the initial 30 mg or 25% of the total propofol dose is administered to evaluate pain, because patients can accurately express the degree of pain at this point. However, in clinical practice, patients complain of greater pain when the remainder of the dose is infused. Therefore, we measured pain during both periods. The incidence of moderate to severe pain were increased when the remainder of the dose is infused than during the initial administration: 52% of the cases in Group L, 24% in Group K, and 8% in Group LK. Group L started with 17% of patients with moderate to severe pain initially, but 52% for the remaining dose, whereas Group LK showed low levels during both periods. Group K also did not change during the administration times. Ketamine's central effect may produce analgesic and sedative to block pain later in administration, whereas pain reduction during the initial administration is from a ketamine's local effect. Eight patients that fell asleep (4 from both Group K and Group LK) before the remaining propofol was administered were removed from the study, but support the theory that ketamine has a central sedative effect.
Ketamine shows sympathetic stimulation leading to increases in blood pressure and heart rate. However, venous occlusion with a tourniquet and ketamine 0.5 mg/kg treatment reduces hypotension from lipid emulsion propofol during anesthetic induction creates hemodynamic stability [18,19]. Furuya et al. [20] stated that ketamine 0.5 mg/kg 1 min before lipid emulsion propofol injection prevented not only an excessive decrease prior to intubation, but also prevented any excessive increase in arterial pressure after intubation, and maintains hemodynamic stability. We will evaluate these effects in the future studies.
A larger dose of 2 mg/kg of ketamine alone can cause psychomimetic emergence reactions. However, doses of 1 mg/kg or below used with hypnotics (such as thiopental), benzodiazepines, inhalation anesthetics, and opioids can prevent this [21-23]. Moreover, ketamine 0.5 mg/kg can also prevent pain when sedation or general anesthesia is induced with lipid emulsion propofol [24-26]. Here we show that ketamine 25 mg is safe as pretreatment before administering microemulsion propofol.
We did not compare lidocaine or ketamine pretreatment with placebo because of the ethical issues around causing severe pain.
In conclusion, a combination of lidocaine 40 mg and ketamine 25 mg with venous occlusion using a rubber tourniquet 1 min before the injection of microemulsion propofol is more effective than lidocaine 40 mg or ketamine 25 mg alone in preventing pain from the injection of microemulsion propofol.