Introduction
The laryngeal mask airway (LMA) is recommended to be removed when patients are fully awake because of the possibility of complications [1]. However, characteristics of children are different from those of adults, and some children respond poorly to verbal commands; so it is difficult to judge whether the child is awake or lightly anesthetized. Therefore, several reports suggest an anesthetized state for the safe LMA removal in children [2,3].
However, the question is how deep the anesthesia should be, because if the LMA is removed at too deep a level of anesthesia, the patient's airway is at risk of being left unprotected for a relatively long time. So it might be ideal to preserve the advantage of extubation under the anesthetic state while reducing the recovery time after the LMA removal. Though a previous study quantified the sevoflurane concentration required for LMA removal without an airway complication in children [4], it should be useful if any other method can further reduce the sevoflurane requirement.
Neuraxial anesthesia exhibits sedative properties that may reduce requirements for general anesthesia [5-9], and caudal epidural block is one of the most commonly performed regional techniques with a reliable perioperative analgesia in pediatric patients. So it is expected that the caudal analgesia would reduce the sevoflurane requirement for a smooth LMA removal in children.
The purpose of this study was to evaluate how much caudal block reduces the sevoflurane requirement for LMA removal without an airway complication in children. So we determined the EC50 of sevoflurane for a smooth LMA removal in children with and without caudal block and compared the EC50 of sevoflurane of each group.
Materials and Methods
After the approval by the institutional review board (IRB), forty-three children (1-6 years) of ASA 1, scheduled for elective inguinal hernia repair, were enrolled in this study. Written informed consent was obtained from the parents of each participant. Patients with an abnormal airway, reactive airway disease, chronic respiratory disease, or a history of an upper respiratory tract infection in the preceding 6-week period were excluded.
The patients were assigned to two groups: to receive caudal analgesia (caudal group) or not (control group), based on parents' consent of caudal analgesia. All children were not premedicated. Upon arrival at the operating room, patients were monitored with pulse oximetry, capnography, inhaled and exhaled sevoflurane concentrations, electrocardiography, and noninvasive arterial blood pressure. Anesthesia was induced using an inhaled technique with 8 vol% of sevoflurane in oxygen via a pediatric circle system. After loss of consciousness, the sevoflurane was adjusted to 3-3.5% according to the vital signs of the patient, and the same concentration of sevoflurane was maintained for several minutes until an adequate jaw relaxation was attained for a LMA (LMA™, The laryngeal mask company Ltd, UK) insertion. The LMA size was determined by the manufacturer's guidelines, which suggests size 1.5 for 5-10 kg, size 2 for 10-20 kg, and size 2.5 for 20-30 kg. After the LMA insertion and before the operation, patients enrolled in the caudal group received caudal block with 1 ml/kg of 0.2% ropivacaine by the attending anesthesiologist. Caudal block was not performed for the patients in the control group. Anesthesia was maintained with sevoflurane in 50% oxygen in air with a total inflow of 2 L/min, and the sevoflurane concentration was adjusted in response to clinical signs. Spontaneous ventilation was maintained throughout the anesthetic maintenance of all patients, and the end-tidal CO2 ranged from 35 to 50 mmHg during the procedure.
At the end of the surgery, the inhaled sevoflurane concentration was adjusted to the 'predetermined' concentration in approximately 50% oxygen in air with a total inflow of 6 L/min and maintained until the exhaled end-tidal sevoflurane concentration was the same as the inhaled concentration; this steady state was kept for at least 10 min. The 'predetermined' concentration of sevoflurane for a particular patient was determined by the response of the previous patient to a larger or smaller concentration (with 0.2% as a step size) using Dixon's up-and-down sequential method [10], starting at 1.8%. Because the patients were not randomly allocated, another anesthesiologist, who didn't know whether the caudal block was performed or not, performed a LMA removal for the blinded study being blinded to the predetermined concentration of sevoflurane. This anesthesiologist removed a LMA with the cuff inflated and recorded whether the LMA removal was successful or not. A successful LMA removal was defined as the absence of any coughing, clenching, breath holding, laryngospasm, desaturation to SpO2 < 90%, and gross movement during or within 1min of the LMA removal [4,11-13]. If a LMA was removed successfully, the sevoflurane concentration for the LMA removal of the next patient was decreased by 0.2%. Conversely, if any of the above complications developed, a LMA removal was regarded as unsuccessful, and the sevoflurane concentration was increased by 0.2% in the next patient. After a LMA removal, a facemask of 100% oxygen was routinely applied for 5 min. If a laryngospasm was suspicious, breath holding persisted for more than 30 s, or tidal volumes were less than 6 ml/kg, positive pressure ventilation was applied. When any complication was settled and adequate ventilation without any assistance was confirmed, the patient was transferred to the recovery room. In the recovery room, pain or emergence delirium was controlled by a 1 mcg/kg intravenous fentanyl injection, with close observation.
Demographic data were collected and presented as a median and range, or mean ± SD, and were analyzed using the Mann-Whitney test or Fisher's exact test. Dixon's up-and-down method needs at least six pairs of failure-success for a statistical analysis of EC50, and the number of enrolled patients came from the basis of Dixon's method. In this study, EC50 was calculated from the mean of seven pairs of failure-success. To evaluate the effect of caudal analgesia on the sevoflurane requirement for a successful LMA removal, we compared EC50 of sevoflurane with caudal block to that without caudal block by a rank-sum test. P < 0.05 was considered statistically significant.
Results
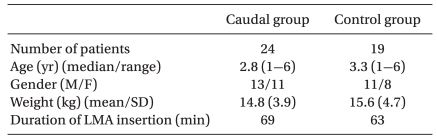
The demographic data and the anesthetic duration are presented in Table 1.
The sequences of successful and unsuccessful LMA removal in each group are shown in Fig. 1. In the control group, EC50 of sevoflurane for LMA removal without airway complication was 1.81 ± 0.11%. However, in the caudal group, EC50 of sevoflurane was 1.47 ± 0.08%; these EC50 were significantly different between two groups (P < 0.001).
In the caudal group, 5 of the 13 children with a successful LMA removal required a chin lift for upper airway support. However, in the control group, all 10 children with a successful LMA removal required a chin lift and/or jaw thrust against upper airway obstruction. In unsuccessful LMA removal cases, most of the airway complications that occurred were treated without any problem; mild laryngospasm, which was defined as an inspiratory stridor without complete obstruction, occurred in 5 patients in the caudal group and in 4 patients in the control group. They were treated with continuous positive airway pressure with 100% oxygen. Desaturation (SaO2 < 90%) was not noticed in any of the patients.
Discussion
From our results, EC50 of sevoflurane for a smooth LMA removal was reduced from 1.81% to 1.47% when caudal block was accompanied in pediatric patients aged 1-6 years.
In children, several studies suggest that the anesthetic state is a better condition for LMA removal in the aspect of reducing airway complication, such as coughing, biting, hypersalivation, and hypoxia [2,3]. However, when an airway device is removed during too deep of an anesthetized state, the risk of prolonged upper airway obstruction or a delayed return of protective reflexes is of main concern [14,15]. In the study about the laryngeal tube, which is a supraglottic airway device similar as the LMA, its removal under an anesthetic state of 2% sevoflurane significantly reduced airway complication but was related to a double incidence of upper airway obstruction compared to its removal in the awake state [16]. In addition, LMA removal in the anesthetic state carries a disadvantage of active pharyngeal reflexes remaining suppressed, resulting in a delayed return of the airway reflex, which causes a potential risk of the patient's airway being left unprotected. Therefore, when a LMA would be removed under the anesthetic state, it is important to apply the least amount of anesthesia, if possible. Several previous studies quantified the adequate depth of anesthesia for LMA removal [4,11,13]; but if caudal block could reduce the sevoflurane requirement more, it would be useful because caudal block is a commonly performed procedure without any direct effect on the airway reflex. Our study showed the expected result-that caudal block reduced about 20% of the sevoflurane concentration for LMA removal without an airway complication.
Xiao et al. studied the effect of caudal anesthesia on the enflurane concentration for LMA removal [12], and the neuraxial anesthesia is known to potentiate sedative drug effects or decrease the minimum alveolar concentration (MAC) of inhalational anesthetics [5-9]. This phenomenon has been explained by several mechanisms. First, pain is considered to play the most important role in the arousal from an anesthesia [17]; caudal analgesia blocks pain from the surgical site, and it decreases the general anesthetic demand. The local anesthetic volume used in this study, 1 ml/kg of 0.2% ropivacaine, is expected to block about T 12 dermatome [18]. Therefore the considerable decrease in the sevoflurane requirement for a smooth LMA removal would be induced by the blockade of nociceptive stimuli throughout caudal analgesia. Secondly, neuraxial block reduces the anesthetic requirement to suppress movement in response to a noxious stimulus above the level of sensory block. The afferentation theory proposes that tonic sensory and muscle-spindle activity modulate cerebral activity and maintain a state of wakefulness, and decreased afferent input to the brain could lessen the excitatory descending modulation of the spinal cord motoneurons and suppress motor function [19-21]. Through these mechanisms, caudal block could reduce the sevoflurane requirement for LMA removal despite the fact that caudal block does not have a direct analgesic effect on the upper airway.
The limitation of our study is that there were no data of time intervals between LMA removal and the return of airway reflex in each group. This study was focused on the effect of caudal block on reducing the sevoflurane requirement for a smooth LMA removal, and so was designed to compare sevoflurane concentrations. We thought the interval in the caudal group might be shorter than that in the no-caudal group owing to the difference in the sevoflurane concentration for LMA removal between the two groups; if the time intervals between the two groups were significant, this study would have been weightier.
In conclusion, caudal analgesia can reduce the sevoflurane requirement for a smooth LMA removal-0.6 MAC is sufficient for LMA removal without any airwayz-related complication in 50% of children while 0.8 MAC is required when caudal analgesia is not performed. Less anesthetic requirements for LMA removal by caudal block would be beneficial for a faster recovery after the LMA removal.