Introduction
Although airways can be managed initially by intubation with an endotracheal tube [1], prolonged endotracheal intubation has been associated with serious complications. Tracheostomy is an essential procedure for long-term mechanical ventilation and has many additional advantages, including effective removal of secretions, secure tube positioning, improved oral nutritional intake, and ease of weaning from mechanical ventilation.
Percutaneous dilatational tracheostomy (PDT) is a simpler, safer, and less expensive procedure compared to conventional surgical tracheostomy [2]. Fiber-optic bronchoscopy (FOB) during PDT has been shown to prevent complications such as pneumothorax and subcutaneous emphysema, and to confirm proper endotracheal placement [3]. Bronchoscopy can cause complications including hypercarbia and hypoventilation during manipulation of the bronchoscope. This, in turn, may result in acute elevation of intracranial pressure (ICP), especially in patients with acute brain injury [4]. FOB also requires additional medical personnel and equipment [5]. Studies have therefore assessed the safety of PDT without the aid of a bronchoscope [6,7], with several studies reporting that PDT can be safely performed under ultrasound guidance [8,9]. However, as with FOB, not all institutions have sophisticated medical devices such as an ultrasonograph.
We previously reported that PDT was safely performed 2 cm below the cricothyroid membrane without bronchoscopy in 186 patients by confirming the underlying structures through palpation [10]. Although this simplified method is convenient and does not require sophisticated equipment, its biggest drawback was the inability to confirm the precise location for PDT, which is critical when performing PDT [11,12]. Although PDT performed approximately at the level of the 2TR [13], patient characteristics can result in anatomical differences [14]. Thus, we examined the effects of patient characteristics on the distance between the cricoid cartilage and the second tracheal ring.
Materials and Methods
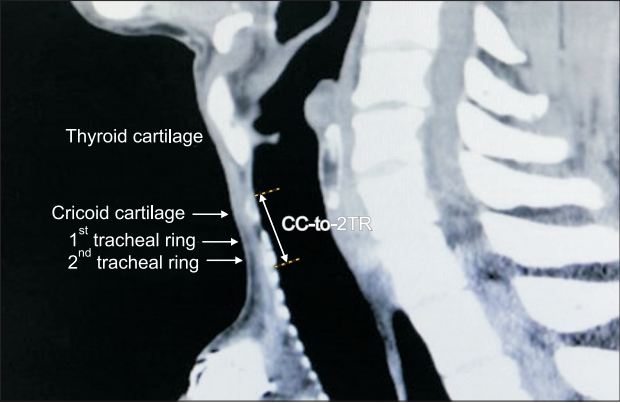
The protocol for this retrospective study was approved by the Institutional Review Board of Chungnam National University Hospital (2015-09-035-005). This study was also registered by the Clinical Research Information Service (KCT0002737). Data from patients who underwent three-dimensional (3D) computed tomography (CT) from January 1, 2012, to December 31, 2015, were retrieved from the Electronic Database of Chungnam National University Hospital. Patients aged > 18 years with physical status of IŌĆōIII according to the American Society of Anesthesiologists classification system were eligible for inclusion. Patients were excluded if they had a history of neck surgery, chemotherapy, radiation therapy, or any procedure that may have caused an anatomical variation. The 3D neck CT images were analyzed using the picture archiving and communication system (PACS; Maroview, Marosis, Korea) software, and the linear distance from the upper part of the cricoid cartilage (CC) to the lower part of the second tracheal ring (2TR) was measured along the sagittal plane in the 3D CT images (Fig. 1).
Statistical analysis
Statistical analysis was performed using the R software version 3.5.1 (R Project for Statistical Computing, Austria) and web-based R version 3.5 (web-r.org). One-sample t-test was performed to compare our previous position (2 cm below the cricothyroid membrane) with the measured CC-to-2TR distances. The correlations between the CC-to-2TR distance and patient characteristics (sex, height, weight, and age) were assessed by linear regression analysis. Multicollinearity between variables, which can be assessed with the variation inflation factor (VIF), is considered problematic if ŌłÜVIF is above 2. Following univariate analysis, variables with P value < 0.2 were selected for multivariate backward stepwise regression. AkaikeŌĆÖs An Information Criterion (AIC) was used for final model selection. To determine the difference between the model and the actual data, we also calculated the mean absolute percentage error (MAPE) and the root mean squared error (RMSE).
The reliability of the predictive model was internally validated by 10-fold cross-validation. This analysis was performed automatically by the Caret package in R [15]. Four hundred and ninety cases were randomly divided into 10 subsamples (1 test set, 9 training sets). The test group data was examined based on the estimated regression equation developed from the data in the training sets (multiple linear regression [by linear model function in R]). This procedure was repeated until all groups had been tested. The RMSE of 10-fold cross-validation was automatically calculated and may vary from trial to trial, since the 10 subsamples were changed for each trial.
Results
Of the 496 patients who underwent neck CT, six were excluded due to cervical vertebral fractures. The characteristics of the included patients and their measured CC-to-2TR distances are shown in Table 1. The mean CC-to-2TR distance was 25.2 mm (95% CI 25.0ŌĆō25.5 mm, compared with 2 cm, P < 0.001). The correlations between CC-to-2TR distance and patient sex, height, weight, and age were determined by simple regression analysis (Fig. 2). All variables were selected for multivariate backward stepwise regression analysis and there was no problem with multicollinearity. The results of the multivariate linear regression analysis for the CC-to-2TR distance are displayed in Table 2. The relative importance of the included factors was 54.5% for height, 37.3% for sex, 6% for weight, and 2.2% for age (Fig. 3). The final selected model:
The in-sample RMSE was 1.72 (mm), indicating that the difference between the actual distance and the estimated distance of the model was 1.72 (mm). The MAPE was 5.8%. This indicates that the predicted value of the model may vary by 5.8%. The RMSE of the 10-fold cross validation was 1.73 (mm).
Discussion
Despite tracheostomy being a common procedure in modern medicine, the ideal location to performe tracheostomy has not yet been determined. Both open tracheostomy and PDT are usually performed between the sternal notch and the thyroid cartilage, with the latter being performed approximately at the level of the 2TR [13]. Tracheostomy between the CC and the first tracheal ring is avoided because it may damage the CC, the only circular cartilage of the upper airways. Tracheostomy under the third tracheal ring is also avoided due to the possible presence of the brachiocephalic artery.
Precise positioning has been shown to be important when performing PDT [11,12]. The risk of tracheal cartilage fracture, a unique complication that may occur during PDT when the Ciaglia method is used, is also increased in the upper level of the trachea. Due to the backwards angulation of the trachea at its entrance to the thorax, additional force must be applied to dilate the intercartilage space at the upper level near the CC. Because the CC is denser than other types of cartilage, the force is transmitted to the lower cartilage, increasing the risk of cartilage fracture. PDT at lower levels reduces the angle between the dilator and trachea, so that less force is needed [16].
The purpose of this study was to determine the relationship between patient characteristics and the CC-to-2TR distance. Confirmation of these relationships may further enhance the safety of performing PDT in the absence of ultrasound or bronchoscopy guidance. Although previous study have examined the relationships between patient demographics and tracheal anatomy (e.g., length, AP diameter, transverse diameter, and cross-sectional area) [17], no study to date has focused on the distance between the cricothyroid membrane and the tracheal rings. CC-to-2TR distances in our study were measured on 3D CT images. Unlike bronchoscopy and autopsy, CT does not affect anatomy and is therefore ideal for measurement [18]. Our results suggest that patient characteristics are correlated with the CC-to-2TR distance.
The present study has several limitations. First, our model needs to be externally validated to determine the accuracy of the predictive model. Our regression equation was tested only by internal validation using RMSE and cross validation. Further studies using sophisticated equipment such as an ultrasound may provide additional support for our prediction model. Another important limitation is the difference in patient positioning during tracheostomy and CT scan (tracheostomy, neck extended position; CT scan, neutral neck position). This difference may alter the CC-to-2TR distance. However, Wong et al. [19] reported that the tracheal elongation from a neutral to extended neck position was 1.01 ┬▒ 0.57 cm when measured with a bronchoscope. Considering the distance from the vocal cords to the carina, which is 13.48 ┬▒ 1.48 cm in the neutral position, this is only 7% of the whole tracheal length. The variation due to patient positioning may be insignificant. The third limitation was the homogeneity of the patient population, in that, all patients were Korean. Because the characteristics of patients in western societies differ from those in Korea, our results may not be applicable to other populations.
In conclusion, our results suggest that patient characteristics should be considered when performing PDT without bronchoscopic guidance. The CC-to-2TR distance depends on patient characteristics, especially height and sex. The use of our model may enhance patient safety when performing PDT without the guidance of sophisticated equipment.