Introduction
Since the brain is the target organ of many anesthetic drugs, clinical investigators have been interested in developing brain function monitors that reliably measure anesthetic drug effects. Several electroencephalography (EEG) monitoring devices have been introduced to measure frontal electrical cortical activity and process the EEG signal to generate indices of brain electrical activity that closely correlate with the hypnotic effects of anesthetics [1–3]. These brain function monitors are designed to measure the adequacy of anesthesia, including expired anesthetic gas concentrations, hemodynamic and respiratory variables, and clinical assessments such as patient movement as a complement to other techniques.
Although processed EEG (pEEG) monitors have been available for decades, they have not been widely used in clinical practice. Without adequate training, the clinical utility of raw EEG waveforms, indices of hypnosis, burst suppression ratios, spectral edge frequency, and various graphical displays on EEG are not obvious. Furthermore, in contrast to standard deterministic monitors, such as electrocardiograms, the pEEG is a stochastic measure that must typically be interpreted probabilistically; therefore, it is inherently less robust than routine clinical monitoring systems. In addition, as a clinical state monitor that requires 15–30 s of raw EEG waveform data, the pEEG indices reflect brain activity from the very recent past; however, real-time data cannot be retrieved as they can with standard deterministic monitors [4].
Despite these limitations, the application of pEEG monitoring in anesthesia patient care has increased. With advances in the understanding and interpretation of raw EEG waveforms, pEEG parameters, and graphical EEG displays (such as spectrograms), the technology has emerged as an important tool for optimizing anesthesia delivery. This review briefly outlines the clinical rationale underlying the application of pEEG monitoring in modern anesthesia practice.
Raw and processed EEG: key features
First, a brief review of basic features of the EEG waveform and how the raw waveform can be processed into various parameters and graphical displays is provided as a framework for EEG interpretation in the clinical setting. Additionally, data supporting the application of pEEG to improve anesthesia care is provided. Key elements include raw EEG waveform morphology, spectral analysis, burst suppression, and alpha power.
EEG waveform morphology
The raw EEG waveform, plotted in microvolts versus time, is characterized in terms of frequency and amplitude and continually cycles around electrical zero. Frequencies are arbitrarily described using five bands measured in cycles per second or Hertz (Hz): delta (< 4 Hz), theta (4–8 Hz), alpha (8–12 Hz), beta (14–32 Hz), and gamma (> 32 Hz). Amplitudes are described using power, defined as the amplitude squared (so that the amplitude is always a positive number), and reported in decibels (dB) using a logarithmic scale that provides a convention to visualize a wide range of amplitudes. The changes in amplitude are referred to as oscillations. Given that available commercial pEEG monitors require sensors that are placed over the forehead, waveform frequency and amplitude signals reflect electrical activity largely from the frontal cortex.
Spectral analysis
Spectral analysis is perhaps the most important of the EEG processing methods in clinical anesthesia because most inhaled and intravenous general anesthetics result in a generalized “slowing” of the raw EEG waveform, wherein the waveform exhibits increased power in lower frequency bands. The slowing of the raw EEG waveform can be characterized using spectral analysis. Applying Fourier’s theorem using a fast Fourier transform, spectral analysis is a mathematical technique used to separate a complex sine wave (like the raw EEG) into its component sine waves, thereby generating a power versus frequency histogram. Drugs used for general anesthesia, such as isoflurane or propofol, characteristically produce a leftward shift in the power versus frequency histogram. This leftward shift is reflected in a lower median frequency (i.e., frequency in the power versus frequency histogram in which 50% of the power is lower and 50% is higher) and a lower spectral edge frequency (frequency below which 95% of the power in the power versus frequency histogram is found).
Spectrogram
In addition to numerical parameters such as the median frequency and spectral edge frequency, the results of spectral analysis can also be visualized in the form of a spectrogram. A spectrogram plots the power across a spectrum of frequencies as they change over time [5]. Time is displayed along one axis and frequency and power along the opposite axis (some commercial devices plot time on the horizontal axis, others plot time on the vertical axis). The frequency typically ranges from 0–30 Hz. Applying a “heat map” approach, the power is presented using colors from blue (-40 dB) to red (15 dB). The “warmer” the color, the greater the power (e.g., blue represents lower power, red represents higher power). The spectrogram is intended to reduce the cognitive workload required for EEG interpretation, making it easier to visualize where most of the power in the EEG signal resides [6]. Fig. 1 presents differences in the alpha band power between two patients.
Burst suppression
When anesthetic concentrations (e.g., halogenated agents, propofol, etomidate, and thiopental) reach sufficiently high levels, periods of isoelectricity are generated in the raw EEG. These periods of isoelectricity are typically interspersed with “bursts” of EEG activity. Higher concentrations of anesthesia can result in complete burst suppression, wherein the EEG is completely isoelectric. Computed as part of a signal processing technique known as aperiodic analysis, the burst suppression ratio is the proportion of time in which the EEG is isoelectric over a specified length of time (usually 15–60 s). Other conditions can also result in burst suppression or isoelectricity, including hypothermia and cerebral ischemia. Advanced age is associated with burst suppression at lower anesthetic concentrations.
Alpha power
The alpha band is of particular interest since it changes with general anesthesia and declines with age more than other frequency bands [7]. Alpha power is thought to originate from thalamocortical electrical activity, which plays a role in integrating sensory information and synchronizing different cortical regions of the brain [8]. Therefore, alpha band power has been the subject of several studies exploring its potential utility as a biomarker of brain health in the perioperative period [9].
The vulnerable brain
The term “vulnerable brain” has emerged as a description of patients who may exhibit increased sensitivity to anesthesia and/or may develop adverse neurocognitive effects after receiving anesthesia. Patients with advanced age, neurovascular disease, intracranial pathology, traumatic brain injury, or an overwhelming infectious or metabolic disorder are some potential examples.
Neuroscientists suggest that neurons in vulnerable brains have a lower mitochondrial production of energy substrates, which reduces neuronal electrical activity and synaptic neurotransmission [10]. Significant cerebral ischemia or hypoperfusion during anesthesia can be detected using EEG changes. Particularly during stable anesthesia, a sudden alteration in the EEG (i.e., a shift in power to lower frequency ranges, decrease in amplitude, periods of burst suppression, isoelectricity, and/or a drop in the pEEG index) may indicate incidental cerebral ischemia.
A large body of work has explored pEEG-guided titration of anesthesia to improve clinical outcomes associated with the vulnerable brain, including postoperative delirium (POD), postoperative cognitive dysfunction (POCD), and mortality. Table 1 presents a summary of results from four randomized controlled trials (RCTs) exploring the effect of pEEG-guided anesthesia delivery on the incidence of POD and POCD.
In a recently published large RCT, the Electroencephalography Guidance of Anesthesia to Alleviate Geriatric Syndromes (ENGAGES) trial [11], the authors compared pEEG-guided (target bispectral index [BIS] value ≥ 40) with routine anesthesia delivery. The main finding was that pEEG-guided anesthesia did not decrease the incidence of POD, despite a modest reduction in anesthetic exposure (a decrease in the median end-tidal anesthesia concentration from 0.8 to 0.7 minimum alveolar concentration [MAC]) and a reduction in the duration of EEG suppression (the median duration of time with a BIS value < 40 decreased from 60 min to 32 min) (Table 1).
In an independent analysis of the ENGAGES trial data, Ackland and Pryor [12] importantly identified that prior retrospective observational studies have established that EEG burst suppression in the presence of low anesthesia concentrations is associated with a higher incidence of POD [13]. They also found that the published threshold for increased risk of POD is a burst suppression duration ≥ 4 min. In the ENGAGES trial, the median EEG burst suppression duration was 7 and 13 min in the pEEG-guided and control groups, respectively. The duration for both groups exceeded the threshold for increased delirium risk. They suggested that with the burst suppression duration above the threshold for POD, it was difficult to draw any conclusions about the utility of pEEG-guided anesthesia delivery for reducing the incidence of POD.
To synthesize a consensus from this body of work, meta-analyses have systematically found that pEEG-guided anesthesia has the potential to reduce the incidence of POD and POCD. Punjasawadwong et al. [14] analyzed data from three RCTs to explore the incidence of POD and POCD in combined cohorts of 2,529 and 2,051 patients, respectively. They reported a reduction in the incidence of POD in patients aged > 60 years undergoing non-cardiac and non-neurosurgical procedures from 21% without to 15% with pEEG monitoring. They also reported a small reduction in the incidence of POCD at three months post-operation from 9% to 6% with pEEG monitoring [14]. In another meta-analysis of five RCTs, which included 2,654 patients, MacKenzie et al. [15] determined that the use of a pEEG monitor was associated with a 38% reduction in the odds of developing POD but data were insufficient to assess the relationship between pEEG and POCD.
Expanding this line of investigation, researchers have identified select measurements for neuronal electrical activity, burst suppression, and changes in the alpha band that may serve as an electrophysiological phenotype of the vulnerable brain [9]. Both are available with newer conventional pEEG monitors; however, they do require some expertise for proper interpretation at the point of care.
Many studies have suggested that anesthesia-induced burst suppression is a risk factor for POD [7,16–19]. For example, Purdon et al. [7], in their study of EEG changes in patients aged 18–90 years who received either propofol or sevoflurane as a maintenance anesthetic, found decreased power in all EEG frequency bands with increasing age. Alpha power was found to decrease more than the other frequency bands and burst suppression was more evident in elderly patients.
In an observational cohort analysis, Fritz et al. [18] enrolled 619 patients who underwent general anesthesia with planned intensive care unit (ICU) admission after surgery. They assessed delirium using the Confusion Assessment Method (CAM) for the ICU and measured the burst suppression. They found that 162 patients developed POD and that patients with more burst suppression were more likely to develop delirium. Approximately 15% of patients who developed POD had no burst suppression; however, 35% of those with ≥ 18 min of burst suppression developed POD. These authors also reported a similar finding, with a BIS value < 20, and found that those patients who received fewer intraoperative opioids were likely to experience more burst suppression. Similar findings have been reported in patients following cardiac surgery [19]. In a retrospective analysis of the same patient cohort, Fritz et al. [16] explored patient sensitivity to inhaled anesthetics. They found that patients who experienced burst suppression at lower concentrations of inhaled anesthesia had a higher incidence of POD and concluded that burst suppression in the presence of low concentrations of inhaled anesthesia may serve as a phenotype of anesthetic sensitivity, increasing their risk for poor cognitive outcomes.
Giattino et al. [20] studied 15 patients who underwent a preoperative neurocognitive assessment and then measured alpha power among other EEG metrics during anesthesia and surgery. They found a correlation between frontal alpha-band activity and preoperative cognitive function that was not present in other EEG frequency bands such as delta, theta, or beta [20]. The authors concluded that lower intraoperative frontal alpha power may be useful for identifying patients with poor cognitive function before surgery who may benefit from practices that minimize or prevent POD and POCD.
In a large multicenter trial, Hesse et al. [17] studied EEG changes during emergence from anesthesia and the development of delirium in the post-anesthesia care unit (PACU). They characterized a set of seven different EEG patterns during emergence from anesthesia, defined as emergence trajectories. Emergence trajectories were compared with the power in the alpha band and other EEG frequency bands. Patients with the various emergence trajectories who did not develop oscillations in alpha power were at a higher risk for POD in the PACU [17]. Of note, this phenomenon was more pronounced in patients who received ketamine or nitrous oxide.
Taking this concept one step further, Shao et al. [9] demonstrated an important relationship between changes in alpha band power and burst suppression. These authors analyzed EEG data for the presence of burst suppression and diminished alpha band power in patients maintained with either propofol or sevoflurane. They characterized the relationship between burst suppression and alpha power using logistic regression and found that for each dB decrease in frontal alpha power, the odds of experiencing burst suppression increased 1.33-fold. From their analysis, they proposed that these findings represent an EEG phenotype of the vulnerable brain.
Although these findings may allow for the early detection of patients who are vulnerable to adverse neurocognitive outcomes, their clinical value requires further investigation and will likely be part of a comprehensive approach to brain health in the perioperative period. In addition to monitoring EEG values, anesthesia care providers will likely have to utilize more refined approaches to anesthesia titration, implement tools to assess cognitive function throughout the perioperative period, and implement postoperative patient care pathways that minimize adverse outcomes [21,22]. Implementing these patient care adjuncts will likely unveil gaps in anesthesia care providers’ experience in conducting a preoperative cognitive assessment and awareness of the adverse consequences of their anesthetic technique on long-term brain health because of limited follow-up with their patients during a period when neurocognitive deficits may appear after surgery.
Recent consensus guidelines from the Periopeartive Quality Initiative (POQI) report insufficient evidence to recommend the use of pEEG monitoring to minimize the risk of POD and POCD in older high-risk patients undergoing general anesthesia [23]. It is important to emphasize, however, that the POQI group of experts noted that three large, randomized trials demonstrated a decrease in POD with EEG-guided general anesthesia, while only the ENGAGES trial showed no effect. We anticipate that future work will explore the use of pEEG monitoring to detect unintended burst suppression that includes recommendations on spectral displays and alpha band power that clinicians can easily interpret to guide anesthetic delivery in the vulnerable brain population.
In summary, when determining which anesthetic approach to use with a patient who is known to have or suspected of having vulnerable brain, EEG monitoring with focused attention on the suppression ratio, alpha band power, and pEEG indices, along with other measures, may prove useful to minimize postoperative neurocognitive decline. Avoiding excessive anesthesia and the use of anesthetics known to increase POD and providing prompt treatment of physiological and metabolic disorders (e.g., low hematocrit, hyponatremia, acidosis, etc.) are also important for minimizing POD.
Reducing awareness during total intravenous anesthesia
There are no monitors available for measuring the concentrations of exhaled drugs when administering total intravenous anesthesia (TIVA). TIVAs commonly consists of a continuous infusion of propofol in combination with bolus administrations or a continuous infusion of an opioid. Anesthesia care providers rely on clinical signs of an adequate depth of anesthesia to ensure continuous delivery of intravenous drugs. This is in stark contrast to potent inhaled agents, for which continuous monitoring of exhaled drug concentrations is routine. Anesthetic drug delivery is confirmed by the presence of exhaled drug concentrations. Another sign of inadequate anesthesia is patient movement. When a neuromuscular blockade is used, which removes patient movement as a sign of inadequate anesthesia, the risk of awareness is higher with TIVA.
Investigators have explored the incidence of awareness with varied results. In a retrospective observational study conducted by the Fifth National Audit Project (NAP5), over 2.8 million patient records over a 12-month period were reviewed to explore the incidence of accidental awareness as spontaneously reported by patients during general anesthesia [24]. The authors reported that 147 patients experienced accidental awareness with an overall incidence of 1 : 19,000 or 0.005%. However, the incidence of awareness varied according to the anesthetic technique. Twenty-eight patients undergoing TIVA reported awareness. TIVA was found to have a higher incidence of 1 : 14,000 or 0.007%, which increased to 1 : 8,333 or 0.012% when it was combined with a neuromuscular blockade. The NAP5 report emphasized that, compared to other anesthetic techniques, awareness with TIVA was largely avoidable and likely related to inadequate drug delivery. In the absence of monitoring to confirm propofol concentrations, the authors suggested that the use of pEEG monitors may help prevent awareness when using TIVA in combination with a neuromuscular blockade. This recommendation is especially important when considering propofol as the maintenance anesthesia. Variability in propofol effects is substantial and requires careful titration to achieve the desired effects while avoiding the adverse effects. For example, recommended target concentrations have been found to range from 3 to 6 μg/ml with target-controlled infusions and can vary further depending on the co-administration of opioids and patient traits such as anxiety or frailty in elderly patients [25].
Exploring a similar question, Errando et al. [26] conducted a prospective single-center observational study investigating the incidence of awareness using a structured interview in the PACU. Investigators, blinded to the anesthetic technique, interviewed 4,001 patients who received anesthesia from 42 different anesthesia care providers. Of these, over 1,200 patients received TIVA and the overall incidence of awareness was 1 : 100 or 1%. According to the anesthetic technique, the incidence with potent inhaled agents was 1 : 167 or 0.6% and with TIVA it was 1 : 91 or 1.1%. The authors found that the incidence was higher in younger patients, with emergency procedures, and with anesthesia delivery at night and the incidence was lower in patients who were premedicated with a benzodiazepine.
The large difference in the incidence of awareness reported in these two studies is likely due to differences in the detection of awareness. The NAP5 study relied on patients’ self-reporting, followed by documentation that could be identified in their retrospective analysis. In the prospective observational study, all patients were interviewed about awareness in the PACU and those that reported events consistent with awareness had follow-up interviews 7 and 30 days later. As such, the methodology used to report awareness likely played a significant role in the reported rates. With a larger patient population, it is more difficult to employ thorough reporting methods.
Many investigators have explored whether pEEG monitoring can be used to detect brain electrical activity associated with awareness [27–29]. Although laudable, this effort is hampered by studying an adverse event that rarely occurs using a monitor that characterizes brain electrical activity but is not a direct measure of patient responsiveness or consciousness. As such, the notion that pEEG monitors could be reliable monitors of awareness remains somewhat controversial. Nevertheless, experts have recommended “the use of end-tidal anesthesia gas monitoring with alarms or pEEG to reduce the risk of awareness with recall in patients receiving general anesthesia” [23].
In summary, when administering anesthesia to patients who may benefit from TIVA and require a moderate-to-deep neuromuscular blockade (e.g., patients with a history of severe postoperative nausea and vomiting undergoing a laparoscope procedure), pEEG monitoring and vigilant attention to intravenous drug administration may minimize the risk of awareness.
Anesthetic titration in patients with hemodynamic instability
Discovering an optimal approach for managing intraoperative hemodynamic instability can be difficult. For example, the best initial treatment of high or low blood pressure may be adjusting the anesthetic dose, administrating a vasoactive agent, or both. However, the most prudent choice is not always evident. As suggested by Fehr et al. [30], pEEG monitors may offer information that would clarify which treatment to apply. However, there is a paucity of research exploring their benefits in this setting. Researchers have explored how pEEG indices in combination with hemodynamic and anesthetic dosing levels may predict adverse outcomes and mortality with inconsistent results [31–34].
As an example, in a large retrospective single-center analysis conducted by Sessler et al. [35], the authors described a triple low phenomenon that consisted of a mean arterial pressure < 80 mmHg, BIS value < 40, and MAC < 0.8, which served as a strong predictor of 30-days mortality. The authors concluded that the triple low was a promising triad, but additional studies are warranted to confirm it is a predictor of perioperative mortality. Follow-up prospective validation comparing mortality between two patient groups exhibiting triple low physiology was conducted. In one group, anesthesia care providers were advised via the electronic anesthetic record to “consider hemodynamic support,” while in the control group, no warning was offered. An effective response to the warning was to administer a vasoactive agent within 5 min of the warning or decrease the end tidal anesthesia by more than 20%. They found that the warning did not change 90-days mortality. The anesthesia care providers, however, had ignored the warning approximately half of the time, which was unanticipated. The authors had anticipated that anesthesia care providers in the advisory group would respond more frequently and fewer would respond in the non-advisory group. They concluded that their data were inadequate to properly explore whether a triple low advisory would improve outcomes [36].
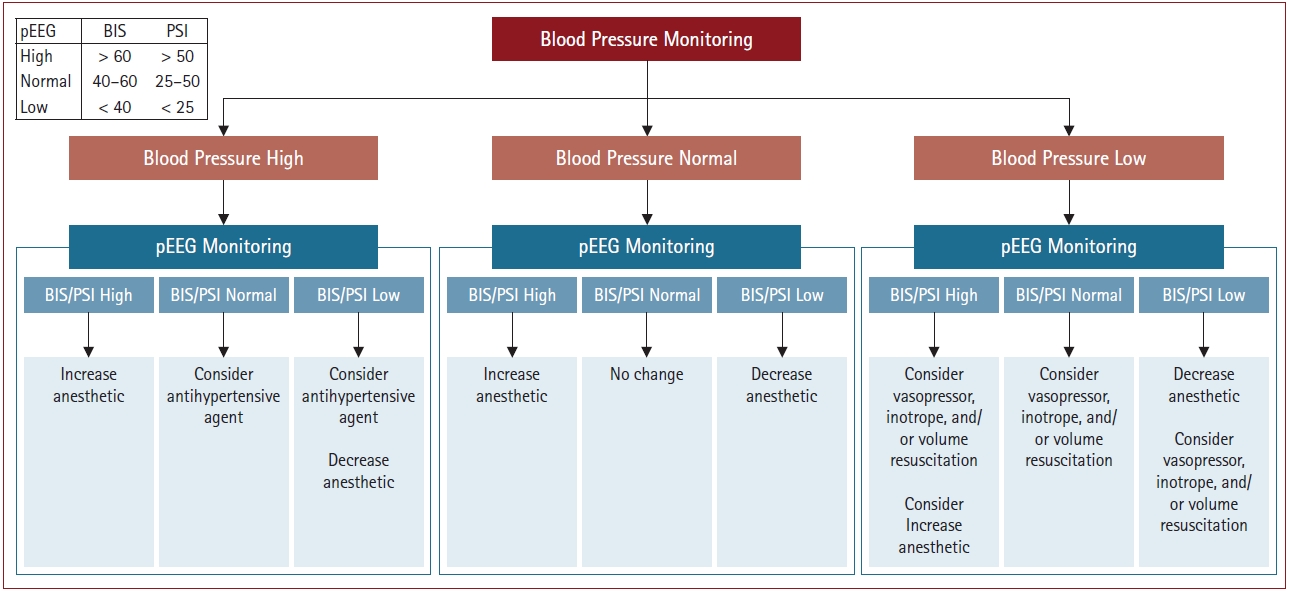
We suggest that this unanticipated finding may represent an education gap among anesthesia care providers. Specifically, anesthesia care providers may lack an understanding of how pEEG indices in combination with other physiologic measures can be used to improve outcomes and address hemodynamic perturbations. We propose that pEEG monitoring could contribute to an adequate discrimination between the need for a vasoactive agent, volume resuscitation, or an adjustment in the anesthesia in a variety of clinical scenarios. As an example, we considered the hemodynamic pEEG profiles that inform intraoperative management. Fig. 2 presents options for normal, low, and high blood pressure conditions versus normal, low, and high pEEG indices.
For example, if a patient exhibits high blood pressure but has a low pEEG index (e.g., a BIS value ≤ 40), even though increasing the anesthesia is likely effective at lowering the blood pressure, it may lead to excessive anesthesia and prolonged emergence. Therefore, antihypertensive agents may be more appropriate. In this scenario, the likely source of high blood pressure is essential hypertension and not inadequate anesthesia. Considering hypertension in the context of pEEG values is useful when caring for patients for whom unnecessary administration of anesthetics may increase the risk of worrisome postoperative adverse events [30].
Under select conditions of mild-to-moderate low blood pressure, in addition to administering vasopressors, inotropic agents, and intravenous fluids, pEEG monitoring may inform appropriate adjustments of the anesthetic. For example, if a patient exhibits mild hypotension and low pEEG indices, corrective actions include reducing the anesthetic and administering vasoactive drugs and intravenous fluids. Although less likely, if a patient exhibits hypotension and high pEEG indices, it may be prudent to restore the blood pressure with vasoactive agents and intravenous fluids before reducing the anesthesia.
In instances of severe hypotension due to blood loss, pEEG monitoring may be especially helpful. Hemorrhagic shock results in an increase in the concentration of intravenous anesthesia due to altered distribution and metabolism. The increased drug levels produce a more pronounced anesthetic effect that is reflected in lower pEEG indices, providing a rational basis for anesthesia administration [37]. Cardiac output is reduced by altering the pharmacokinetics of anesthetic drugs. As the volume of distribution contracts, conventional dosing can lead to elevated blood and effect-site drug concentrations with pronounced effects. When managing an anesthesia under these conditions, anesthesia providers often decrease drug delivery.
An example of this phenomenon was presented in a case report describing the blood pressure and BIS values resulting from significant blood loss in a 70-year-old woman who underwent abdominal aneurysm repair [38]. The patient was anesthetized with propofol-alfentanil (TIVA). Notably, the hemorrhage-associated drop in blood pressure was preceded by a drop in the BIS. The authors suggested that pEEG values may serve as an early warning of altered drug pharmacokinetics due to severe blood loss.
In summary, we suggest that pEEG monitoring may play a role in anesthesia and resuscitative management when faced with adverse changes in blood pressure. We also suggest addressing education gaps that exist in clinicians’ understanding of how pEEG monitoring in combination with conventional physiological monitors may be used to improve intraoperative and long-term patient outcomes.
Patients with a history of substance abuse
Formulating an appropriate anesthetic dose in patients with a history of substance abuse to achieve the desired level of sedation, analgesia, and immobility presents challenges. Prolonged exposure to opioids, alcohol, and stimulants or the use of drugs to treat opioid use disorders may make it difficult to find an appropriate anesthetic dose. The primary concern is the risk of unintended awareness during general anesthesia [39]. Prior work exploring the scientific foundation behind this concern is limited, but that which exists is interesting and perhaps unexpected. The selected substances are briefly discussed below.
Researchers have studied how painful stimuli processing is altered in chronic pain. Chronic opioid use differentially affects the level of consciousness and spinal cord responses to surgical stimulation. For example, Oh et al. [40] measured end-tidal sevoflurane concentrations needed to maintain a BIS value < 50 (SEVOBIS50) in both chronic opioid users and opioid-naïve patients. They defined chronic opioid users as those who received a stable dose of oral morphine of at least 60 mg per day for at least 4 weeks. The SEVOBIS50 was determined using Dixon’s up-down method and probit analysis. The predetermined consistent end-tidal sevoflurane concentration was confirmed and maintained for 15 min to ensure equilibrium in end-tidal and effect site concentrations. Subsequently, BIS values were obtained for 1 min at 10-s intervals in the absence of a surgical stimulus. If the average of the five values was < 50, the authors decreased the sevoflurane by 0.2% for the next patient, and if the average was > 50, the authors increased the sevoflurane by 0.2% for the next patient. They reported a modest decrease in the SEVOBIS50 levels for chronic opioid users compared to opioid-naïve patients (0.84 [95% CI: 0.58, 1.11] and 1.18% [95% CI: 0.96, 1.40], respectively). Although not intuitive, patients who chronically consume opioids may require less maintenance anesthesia.
The mechanism behind this observation is not well understood; however, it may be a function of how the data were collected and how the results were interpreted. SEVOBIS50 is not defined in the same manner as the MAC. The MAC is defined as the concentration needed to blunt a response to a standard stimulus such as surgical incision in 50% of patients, whereas the BIS is a pEEG index of brain electrical activity suppression. Although the authors did not explore changes in the MAC of sevoflurane due to chronic opioid use, they did evaluate how chronic opioid use influences brain electrical activity under general anesthesia. A limitation of this approach was that the SEVOBIS50 was not evaluated in the presence of a nociceptive stimulus. Unlike with MAC studies, the impact of sevoflurane on spinal cord transmission from nociceptive stimuli has not been determined.
As with the vulnerable brain, patients with chronic pain exhibit unique characteristics in the spectral display. Specifically, patients with chronic pain exhibit changes in the theta frequency band (3–8 Hz) that are not observed in opioid-naïve patients [41]. The clinical implications of these changes are yet to be elucidated. Future work is warranted to explore how changes in the theta frequency band can be used to titrate anesthetic delivery to this patient population.
In response to the opioid epidemic, buprenorphine has been used to manage patients with opioid use disorders and chronic pain. Buprenorphine is a partial opioid mu receptor agonist and an opioid kappa and a delta receptor antagonist. It has a much higher affinity for mu receptors than several commonly used opioids, such as fentanyl, hydrocodone, oxycodone, and morphine, but has a similar affinity as hydromorphone [42]. With a higher affinity, it displaces opioid agonists and competitively occupies up to 80%–95% of receptors at clinical doses. As a partial agonist, it is considered safer since there is an associated ceiling effect on ventilatory depression, although the analgesic effect may be less pronounced [43]. Conflicting concerns have emerged regarding its use during the perioperative period, such as a concern for inadequate acute pain control because buprenorphine occupies mu receptors, displacing pure opioid agonists. Conversely, cessation of buprenorphine increases the risk of opioid use disorder relapse and is associated with adverse outcomes.
Recent recommendations propose maintaining buprenorphine at preoperative doses throughout the perioperative period [43,44]. Under select conditions, reducing the buprenorphine dosage may be considered with procedures associated with significant pain. This is done to allow for more receptors to be occupied by full opioid agonists.
Although these guidelines focus on the challenges of providing adequate and safe perioperative care, they are based on lower levels of evidence, such as case series, case reports, observational studies, studies without control groups, and expert consensus. Future work is therefore warranted to establish evidence on how to best manage buprenorphine administration during the perioperative period. Therefore, when determining the appropriate anesthesia for patients receiving buprenorphine, the anesthesia and the dose require individualized and timely adjustments to achieve the desired effects. Opioid analgesic efficacy and interactions with sedatives and potent inhaled agents are likely altered, making conventional approaches to dosing challenging and even inadequate. Using pEEG indices and end-tidal inhaled agent concentrations may prove useful in titrating anesthetic delivery in this patient group.
Alcoholics can have varied anesthesia requirements based on the state of inebriation. If acutely intoxicated, they require less anesthesia, and if sober, they can have increased anesthesia requirements. Acute alcohol intoxication slows the EEG and may influence BIS values. Gerstman et al. [45] found a moderate correlation between BIS values and venous blood alcohol concentration (r = –0.49, P = 0.029) in healthy young adults. In their study, 21 participants consumed a median of 90 g of alcohol over a 3-hour period. The authors concluded that BIS values may decrease in the presence of alcohol.
Fassoulaki et al. [46] compared the induction and maintenance propofol dose requirements in alcoholics and non-alcoholics. They defined chronic alcoholics as those who had consumed an average of 40 g/day of ethanol for at least 2 years. They defined non-alcoholics as those who consumed alcohol only occasionally or not at all. They found that with induction, the mean propofol dose required for loss of responsiveness was modestly increased in alcoholics compared to non-alcoholics (2.7 ± 0.4 vs. 2.2 ± 0.4 mg/kg, respectively). Similarly, when using propofol as the maintenance anesthesia, the total amount was increased in alcoholics compared to non-alcoholics (4.2 ± 1.0 vs. 3.2 ± 0.8 mg/kg, respectively) [46].
In summary, providing anesthesia to patients with known or suspected substance use is difficult, since they may have unanticipated increased or decreased requirements. The use of pEEG monitoring with attentive hemodynamic monitoring may be better for identifying anesthesia requirements and guiding anesthetic titration to avoid excessive or inadequate anesthesia administration.
In conclusion, advances in understanding the nuances in intraoperative EEG monitoring at the point of care are emerging to better guide anesthesia delivery in select patient populations. In this article, we reviewed well-supported, but perhaps poorly appreciated, key features of EEG waveforms, and their clinical implications. These key features include EEG waveform morphology, spectral analysis, burst suppression, and alpha power. We recommend anesthesia providers receive education to increase awareness of the clinical utility of these key EEG features at the point of care. This review article also posits that in select patient groups and anesthetic techniques, pEEG monitors can improve patient outcomes and minimize adverse events.