Introduction
Cesarean section is one of the most common operations performed worldwide. It is, however, associated with moderate to severe pain in almost four fifths of women [1] and, when compared to many other surgical procedures, it has been reported to be the ninth most painful operation on the first postoperative day [2]. Pain during and following cesarean section has been demonstrated to be of greatest concern to women [3], and inadequate pain relief has been related to negative effects on breastfeeding and infant care [1], maternal dissatisfaction [4], postpartum depression [5], and chronic pain [5,6].
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly used as part of a multimodal strategy in the perioperative period, and provide analgesia by the inhibition of cyclooxygenase enzymes that are involved in the formation of hyperalgesic prostaglandins [7]. In a meta-analysis that compared control to NSAIDs, NSAIDs decreased the pain score at rest at 12 h and 24 h and on movement at 24 h, lowered opioid consumption, and reduced the risk of sedation, the latter a recognized side effect of opioids [8]. Given this, the procedure specific postoperative pain management (PROSPECT) recommendations for elective cesarean section include the intraoperative use of intravenous NSAIDs and postoperative use of oral or intravenous NSAIDs [9]. It is still not clear, however, which NSAID is most effective in the setting of cesarean section. Different NSAIDs may produce varying pain relief efficacy and have differing side effect profiles, and hence a comparative analysis of NSAIDs is important. Several randomized trials investigating NSAIDs have been published recently [10,11], and a contemporary review would update the available evidence for the use of NSAIDs in cesarean section.
Our aim in this network meta-analysis and systematic review was to compare the influence of control and individual NSAIDs such as diclofenac and ibuprofen on the indices of analgesia, side effects, and quality of recovery. We hypothesized that we would establish the overall efficacy of NSAIDs in cesarean section, and potentially uncover differences among the NSAIDs studied.
Materials and Methods
We prospectively registered the protocol for the systematic review and network meta-analysis with PROSPERO (CRD42021264209), and our findings have been presented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [12]. The following databases, CDSR, CINAHL, CRCT, Embase, LILACS, PubMed, and Web of Science, were searched from inception to May 27, 2021, for free text keywords and subject headings associated with different permutations of terms related to cesarean section, obstetric analgesia, NSAIDs in general, and specific NSAID drug names (Supplementary Material 1).
Once duplicate citations were discarded, two authors (IM and ND) independently screened the titles and abstracts of the remaining citations against the inclusion and exclusion criteria in Rayyan (Qatar Computing Research Institute, 2016, Doha, Qatar) [13]. Inclusion criteria were defined as randomized controlled trials that compared a specific NSAID to either control or another NSAID in the context of elective or emergency cesarean section under general or neuraxial anesthesia. The timing of NSAID administration could be preoperative, intraoperative, and/or postoperative, and trials that investigated more than one NSAID, either combined or in more than one arm, were included. Exclusion criteria included trials in which regional anesthesia or wound catheters were utilized postoperatively. Trials that included intraoperative local anesthetic infiltration and single-shot transversus abdominis plane block, for example, were included, but those that used postoperative infusions of local anesthetic through catheters into the epidural space, transverse abdominis plane, or wound were excluded. No limits were placed on the language of publication. Cases of disagreement were resolved by a third author (BC). If a trial was thought to be eligible for inclusion, then we carried out a full text review to confirm this. In order to seek further trials not identified by our search strategy, one author (AC) searched the reference lists of included trials and previously published systematic reviews.
Data extraction was conducted and checked by five authors (IM, AC, PS, JO, and ND). The following characteristics of trials were extracted: number of patients in each group; nature of cesarean section; mode of anesthesia; intraoperative regional anesthesia and systemic analgesia; dose, route, and timing of NSAID administration; regular postoperative analgesia; and management of postoperative breakthrough pain. The primary outcome was the cumulative intravenous morphine equivalent consumption at 24 h, and the MCID was prespecified at 10 mg. It is the opinion of the authors that this outcome is particularly important as it provides a measure of pain and need for rescue analgesia on the first postoperative day, and increased opioid consumption has been associated with side effects such as nausea and vomiting, urinary retention, constipation, and sleep disturbance that can lead to distress and interfere with postoperative recovery [14]. In a systematic review, the clinician perceived the MCID estimate for this primary outcome in the setting of total hip and knee arthroplasty was 10 mg and, in the absence of evidence-based and patient-rated MCIDs, we concurred with this [15]. Secondary outcomes included: pain score at rest and on movement at 8–12 h, 24 h, and 48 h; need for rescue analgesia and time to first analgesic request; cumulative intravenous morphine consumption at 8–12 h, 48 h, and in-hospital; incidence of postoperative nausea and/or vomiting, pruritus, and sedation at 24 h, 48 h, and in-hospital; quality of recovery-15 (QoR-15) [16] at 24 h and 48 h; and hospital length of stay. No other secondary outcomes were considered. We extracted dichotomous data as numbers and continuous data as means and standard deviations. If data were presented as medians, these were assumed to be equal to the means, and the standard deviations were calculated by dividing the interquartile range by 1.35 or the range by 4 as per guidance from the Cochrane Collaboration [17]. In cases where data were presented only in graphical format, PlotDigitizerTM (Version 2.1, Free Software Foundation, USA) was utilized in order to facilitate numerical extraction. Opioid conversion was performed with reference to the British National Formulary [18] and Faculty of Pain Medicine [19]. Where the data were not published or unclear, the authors were emailed up to three times for clarification.
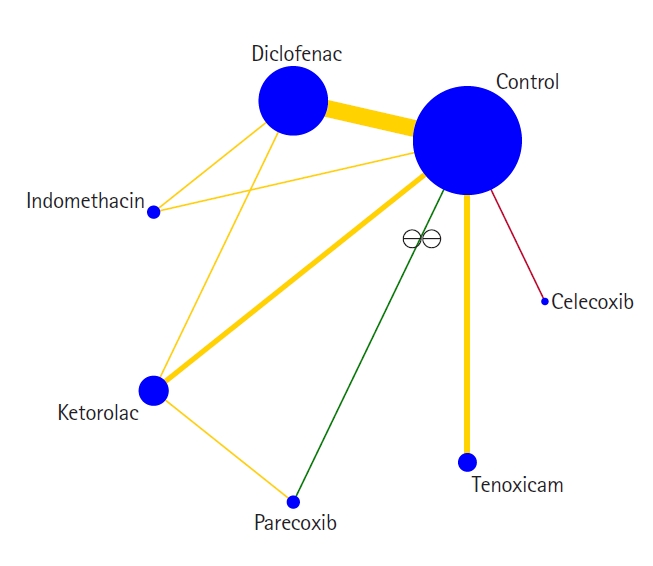
Subsequent to data extraction, the data were transferred from Microsoft Excel® (Microsoft, USA) into Stata (Version 16.1, StataCorp LLC, USA) by one author (ND) and then checked by a second author (IM). We conducted this network meta-analysis with a frequentist method on any outcome of interest if three or more competing interventions could be connected into a network through direct comparisons between the trials [20,21]. Network plots were produced for all outcomes subjected to network meta-analysis with a common heterogeneity parameter and multivariate methods. In these network plots, the nodes depicted the interventions and the connecting lines represented the direct comparisons between the interventions. If interventions were not directly compared within trials, indirect comparisons via a common comparator were mathematically derived using results from the various direct intervention effects. Consistency was locally and globally assessed between direct and indirect estimates by the Separating Indirect from Direct Evidence technique and with the design-by-treatment interaction test, respectively. The results of comparisons between the different interventions were presented in network league tables as mean differences and 95% CIs for continuous outcomes and odds ratios and 95% CIs for dichotomous outcomes. If serious imprecision was not present for a particular outcome, competing interventions were ranked in order. We performed pairwise meta-analysis in Review Manager® (Version 5.3, The Nordic Cochrane Centre, Denmark) for those outcomes that were not analyzable by network meta-analysis but were reported by two or more randomized controlled trials. Heterogeneity was calculated with predetermined thresholds for low (25%–49%), moderate (50%–74%), and high (≥ 75%) levels [22], and the fixed and random effects model used for low and moderate or high heterogeneity, respectively. Tests were two-tailed and statistical significance was represented at the 5% level. The results were presented as mean differences and 95% CIs for continuous outcomes and risk ratios and 95% CIs for dichotomous outcomes.
The quality of evidence for every outcome was evaluated by two authors (IM and ND) using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system [23] and with the CINeMA software® (Institute of Social and Preventative Medicine, University of Bern, Switzerland). Fundamental components of quality include: risk of bias, indirectness, imprecision, inconsistency, and publication bias. Risk of bias was determined by two authors (JO and DO) using the Cochrane Risk of Bias 2 (RoB 2) tool [24] to examine the following: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Cases of disagreements were resolved by a third author (ND). Publication bias was examined with a comparison-adjusted funnel plot and the Egger’s linear regression test.
Results
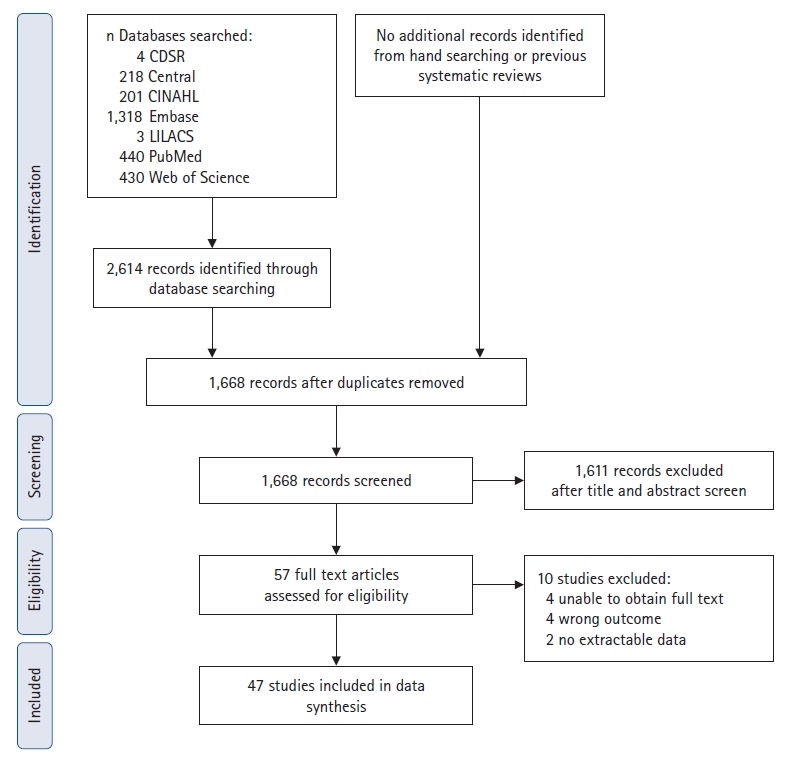
In all, we included 47 trials in this review [10,11,25–69] and details of the screening process are illustrated in Fig. 1. The following interventions were compared: control vs. celecoxib in two trials [35,46]; control vs. celecoxib + parecoxib in one trial [57]; control vs. diclofenac in 24 trials [11,25–34,36–43,65–69]; control vs. diclofenac vs. indomethacin in one trial [44]; control vs. diclofenac vs. ketoprofen in one trial [45]; control vs. ibuprofen vs. ketorolac in one trial [47]; control vs. indomethacin in one trial [48]; control vs. ketorolac in six trials [10,49–53]; control vs. naproxen in one trial [54]; control vs. parecoxib in one trial [55]; control vs. tenoxicam in six trials [56,58–62]; diclofenac vs. ketoprofen in one trial [63]; and ketorolac vs. parecoxib in one trial [64]. The findings of the risk of bias assessment are presented in Fig. 2. Overall, only four trials were deemed to be at low risk of bias [10,54,55,68], and 30 and 13 of the remaining trials were evaluated to have some concerns [25,27–35,37,38,43–45,47,49,52,53,57–67] or be at high risk of bias [11,26,36,39–42,46,48,50,51,56,69], respectively. Many of the concerns were related to the randomization process, measurement of the outcome, and the selection of the reported result. Of the 21 authors we emailed to clarify on methodology or results, nine responded with the requested information [38,42,43,50,53,55,61,62,65].
Characteristics of the trials are presented in Table 1. In regard to the nature of the cesarean section, it was elective, elective or emergent, and not specified in 30 [10,26,29,31–35,37,38,45,48–51,53–58,60–62,64–69], six [11,30,40–43], and 11 [25,27,28,36,39,44,46,47,52,59,63] trials, respectively. The mode of anesthesia was spinal, combined spinal-epidural (CSE), epidural, or general anesthesia in 27 [10,11,29,32–35,37–39,41–44,46,48,50,54–56,60–64,68,69], two [51,57], three [49,66,67], and 11 [25–28,30,31,47,53,58,59,65] trials, respectively. Of the remaining trials, one performed spinal or epidural anesthesia [45], two used neuraxial or general anesthesia [40,52], and one did not specify the type of anesthesia [36]. Single-shot transversus abdominis plane block was utilized in one trial [11]. In addition to NSAIDs, women received propacetamol or paracetamol in four trials [32,33,37,57]. The route of administration of NSAIDs was as follows: oral in two trials [35,46]; intramuscular in 13 trials [25,27,28,31,34,36,38,40,43,49,65–67]; intravenous in 16 trials [10,11,39,45,50–53,55,56,58–62,64]; rectal in 11 trials [26,29,30,32,33,41,42,44,48,68,69]; oral or intramuscular in one trial [47]; intravenous and oral in one trial [57]; intramuscular or intravenous in one trial [63]; and rectal and oral in two trials [37,54]. In 21 trials, just one dose of NSAIDs was administered [10,11,26,35,36,39,46,49,55,56,58–63,65–69] and in further 21 trials, more than one dose or an infusion of NSAIDs was given [25,29–33,37,38,40,42–45,48,50–54,57,64]. Some trials provided NSAIDs only when the pain was reported to be at least moderate in intensity [34,41], or the pain score was greater than or equal to seven on a scale of zero to 10 [27,28] or higher than or equal to 60 on a scale of zero to 100 [47].
Our primary outcome, the cumulative intravenous morphine equivalent consumption at 24 h, was evaluated in 1,228 patients and 18 trials [27–29,32–34,37,39,44–46,50,52,55,58,61,62,64]. In the network plot, nine direct and 12 indirect comparisons were established between seven interventions (Fig. 3). With an MCID of 10 mg, control was clinically and statistically inferior to diclofenac, indomethacin, ketorolac, and tenoxicam (Table 2). No other statistical differences were demonstrated between the various NSAIDs. Evidence for local or global inconsistency was not found and the standard deviation of between-trials heterogeneity was 11.08. Inspection of the comparison-adjusted funnel plot (Supplementary Fig. 1) and the results of Egger’s test (P = 0.011) revealed the presence of publication bias. The quality of evidence was graded as very low (Supplementary Material 2), and the network ranking of interventions was not performed in view of the serious imprecision (Supplementary Material 3).
Details of the results of the secondary outcomes are presented in Table 3 and Supplementary Material 3, and information related to their network plots, inconsistency plots, contribution plots, predictive interval plots, and comparison-adjusted funnel plots is provided in Supplementary Material 4. Differences between NSAIDs were shown for some of these outcomes. For the pain score at rest at 8–12 h, indomethacin was clinically and statistically superior to celecoxib, and for the pain score on movement at 48 h, indomethacin was clinically and statistically superior to celecoxib + parecoxib, diclofenac, and ketorolac. In regard to the need for rescue analgesia, ketoprofen was clinically and statistically superior to celecoxib + parecoxib, and with respect to the time for rescue analgesia, diclofenac, ibuprofen, indomethacin, and ketorolac were clinically and statistically superior to celecoxib. In terms of side effects, ketoprofen was clinically and statistically superior to celecoxib + parecoxib for the rate of in-hospital pruritus, and diclofenac was clinically and statistically superior to control for the rate of sedation at 24 h and in-hospital. The hospital length of stay was statistically but not clinically different between diclofenac and control.
Discussion
Our systematic review and network meta-analysis demonstrated that, compared to control, the administration of diclofenac, indomethacin, ketorolac, or tenoxicam led to a clinically significant decrease in the primary outcome, namely cumulative morphine consumption at 24 h, using an MCID of 10 mg. The quality of evidence, however, was very low due to serious limitations, imprecision, and publication bias. Differences between various NSAIDs were found, with indomethacin clinically superior to celecoxib and celecoxib + parecoxib, diclofenac, and ketorolac for the pain score at rest at 8–12 h and the pain score on movement at 48 h, respectively, when an MCID of 10 on a pain scale of 0–100 was applied. Indomethacin may be preferable, although it must be recognized that the evidence for other NSAIDs continues to emerge and is currently limited by the presence of imprecision.
In contrast to diclofenac, indomethacin, ketorolac, and tenoxicam, control was not inferior to other NSAIDs such as celecoxib and parecoxib for the cumulative morphine consumption at 24 h. It is likely that this could be a reflection of the limited evidence base for these NSAIDs, resulting in imprecision and wide CIs, and the different dosing regimens employed in the included trials. In many trials that investigated diclofenac, indomethacin, and ketorolac, more than one dose of the NSAID was administered in 24 h [25,27–33,37,38,40,42–45,48,50–53]. Further, tenoxicam has a long mean elimination half-life of 67 h [70], explaining its beneficial effects on morphine consumption despite only being given once in the relevant trials [56,58–62]. Similarly, the various dosing strategies in the included trials may explain, at least in part, the superiority of ketoprofen to celecoxib + parecoxib in regard to the need for rescue analgesia and diclofenac, indomethacin, and ketorolac, but not ibuprofen, over celecoxib with respect to the time to rescue analgesia. Selective COX-2 inhibitors such as celecoxib have gained popularity as effective analgesics, particularly as they can produce fewer gastrointestinal side effects [71]. Their inferiority to other NSAIDs could be indicative of their slow absorption from the small intestine following oral administration [72], and their relatively homogenous distribution in body tissue in comparison to acetic acid derivatives with acidic functional groups such as diclofenac, ketorolac, and indomethacin. NSAIDs that are acetic acid derivatives as well as those with high protein binding can selectively accumulate and persist in areas of inflammation [72,73], and this may facilitate their increased analgesic effectiveness at sites of tissue injury subsequent to cesarean section. The superiority of indomethacin to other NSAIDs might be representative of its potential to act as a positive allosteric modulator at the type one cannabinoid receptor, modifying the endocannabinoid system and increasing its antinociceptive properties [74].
In terms of side effects, diclofenac compared to control resulted in decreased sedation at 24 h and in-hospital. This probably underlines its capacity to influence the pain score at 8–12 h and 24 h as well as the need for and time to rescue analgesia, hence reducing the cumulative morphine consumption and these secondary undesirable effects. Interestingly, in the absence of differences in the cumulative morphine consumption, ketoprofen decreased the rate of in-hospital pruritus compared to celecoxib + parecoxib. NSAIDs do not have any recognized direct antipruritic effects [75], and it is possible that the lack of difference in the cumulative morphine consumption was once again a reflection of imprecision rather than absence of true underlying differences.
Our findings corroborate and expand upon the systematic reviews and meta-analyses conducted to date. Consistent with what we have shown, in a prior meta-analysis of 22 randomized controlled trials, NSAIDs were reported to be superior to control in the context of cesarean section for the pain score at 12 h and 24 h and the cumulative morphine consumption [8]. NSAIDs have been compared in settings outside that of cesarean section in other systematic reviews [76–78]. In a previous network meta-analysis of 26 randomized controlled trials, etoricoxib was superior to celecoxib, ketoprofen, and tenoxicam for pain relief in ankylosing spondylitis [76], and in a prior systematic review of 76 randomized controlled trials, diclofenac, etoricoxib, and rofecoxib were ranked highest for the reduction of pain in hip and knee osteoarthritis [77].
We acknowledge the limitations related to this meta-analysis. First, there were a limited number of trials comparing different NSAIDs. Second, few trials were evaluated to be at low risk of bias, and concerns were present in the remaining trials in regard to the randomization process, measurements of the outcome, and the selection of the reported result. Third, the included trials investigated patients who had emergency and/or elective cesarean section under neuraxial, with or without intrathecal opioids, or general anesthesia. Moreover, the strategy of NSAID administration was inconsistent with varied dosing, route, and duration. Such variability introduces heterogeneity, although it increases the generalizability of the findings. Fourth, the standard practice of multimodal analgesia with paracetamol was, surprisingly, only used in a minority of trials. The combination of paracetamol and NSAIDs has been recommended due to their additive effect [79,80]. Fifth, a change in the pain score of 10 on a pain scale of 0–100, including in obstetrics, has been revealed to represent a clinically important difference in the intensity of pain [81]. It is likely, however, that the MCID for any individual patient may vary depending on the severity of the pain, with a greater MCID needed for more severe pain [82]. The MCID for many indices remains undetermined in cesarean section [83], and the authors thus used their experience in this systematic review to select the different thresholds for clinical significance. Sixth, concerns with respect to imprecision for most outcomes precluded the ranking of various NSAIDs. Last, we did not examine which NSAID was best in terms of minimizing transfer to breast milk and increasing safety in breastfeeding women. Those NSAIDs with low oral bioavailability, high protein binding, short half-life, and inactive metabolites as well as reassuring data on breast milk transfer and long record of safe use are likely to be optimal in this respect [80,84]. Interestingly, ibuprofen is thought to be the ideal NSAID for women who are breastfeeding, but our results do not provide sufficient data to confirm its superior properties in the context of cesarean section.
Our network meta-analysis and systematic review demonstrated that diclofenac, indomethacin, ketorolac, and tenoxicam compared to control decreased cumulative morphine consumption at 24 h. No differences were found between different NSAIDs in the cumulative morphine consumption at 24 h, and the quality of evidence was very low. Differences in the secondary outcomes between various NSAIDs were uncovered, with indomethacin clinically superior to celecoxib and celecoxib + parecoxib, diclofenac, and ketorolac for the pain score at rest at 8–12 h and the pain score on movement at 48 h. In light of this emerging but limited evidence, our review suggests the presence of minimal differences among the NSAIDs studied. Nonselective NSAIDs may be more effective than selective NSAIDs, and some NSAIDs such as indomethacin might be preferable to other NSAIDs. Further trials with designs relevant to modern obstetric anesthesia practice are required to increase the strength and quality of the evidence base and the recommendations related to the selection of NSAIDs in the setting of cesarean section.